 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Mem Inst Oswaldo Cruz, Rio de Janeiro, Vol. 97(6) September 2002, pp. 893-896 SHORT COMMUNICATION
Biological Variability in Clinical Isolates of Trichomonas vaginalis Alicia Gómez-Barrio+, Juan J Nogal-Ruiz, David Montero-Pereira, Ester Rodríguez-Gallego, Esperanza Romero-Fernández, José A Escario
Departamento de Parasitología,
Facultad de Farmacia, Universidad Complutense, Ciudad Universitaria, 28040 Madrid,
España This study was supported by the Universidad Complutense, Project PR181/96. We declare that all experiments performed comply with current Spanish laws. Received 4 December 2001 Code Number: oc02171
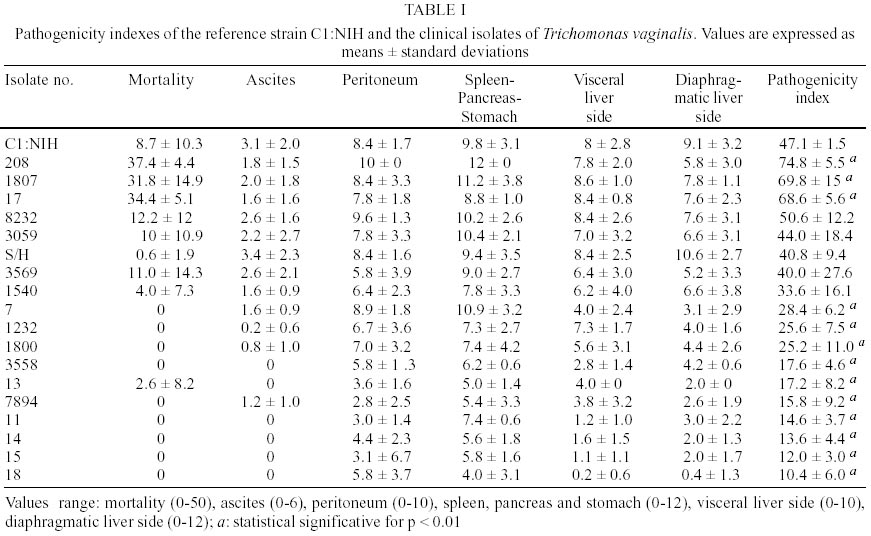
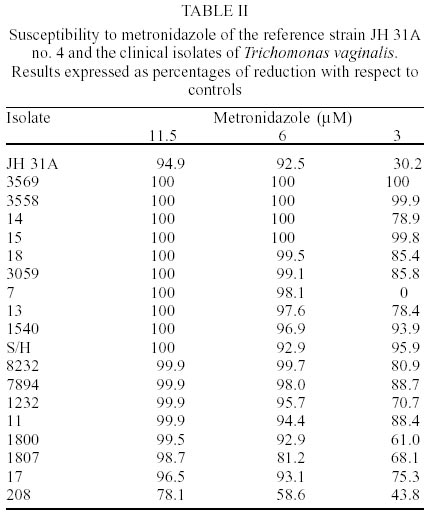
Eighteen clinical isolates of Trichomonas vaginalis were obtained from women who attended health centers of the Goverment of Madrid. A total of 1,848 vaginal specimens recovered during the gynaecological examination were seeded in culture tubes containing liquid Diamond medium. Pathogenicity to mice was determined after intraperitoneal inoculation of mice by quantification of mortality and gross damage to abdominal organs. As could be expected, a broad variability was obtained, being some of the isolates more virulent than the reference strain. Regarding to metronidazole susceptibility, none resistant isolate was found but different degrees of susceptibility were determined.
Key words: Trichomonas vaginalis - pathogenicity to mice - metronidazole Trichomonas vaginalis is the causative agent of the most common, non-viral sexually transmitted disease (STD). This parasite is the main cause of vaginitis, cervicitis and urethritis in women and may be responsible for prostatitis and other genito-urinary syndromes in men. Moreover, it has been related to more serious diseases as cervical neoplasia (Gram et al. 1992, Zhang & Begg 1994, Viikki et al. 2000). An association between T. vaginalis infection and an increased risk of transmission of other STDs, including human immunodeficiency virus, has been also suggested (Laga et al. 1993, Sorvillo & Kerndt 1998). The total amount of women affected per year worldwide is around 170 millions (WHO 1997). In Spain, three studies concerning the prevalence of trichomoniasis and other STDs have been published (Perea et al. 1981, Orduña Domingo et al. 1991, Ulla et al. 1993), but in Madrid only an epidemiological survey has been recently made (Alonso Sanz et al. 1996) among the female prison population of Carabanchel. Although the parasite does not usually cause important sequelae, there is a great variability in the pathological manifestations, from asymptomatic presentation to increased risk of pelvic inflammatory disease and tubal infertility (Cates et al. 1993). The reasons for such variation and how the characteristics of every clinical isolate impact the clinical manifestations of trichomoniasis are not well known. Despite the high prevalence and associated risks of trichomoniasis, very little is also known about the biological variability of the parasite. Experimental pathogenicity is one of the parameters that can be applied to the characterization of isolates, because of it varies so broadly as clinical pathogenicity does. Regarding to treatment, during the last two decades about 20 metronidazole-resistant strains have been described from Europe (Meri et al. 2000). If, as Meri et al. (2000) suggest, the metronidazole resistance of T. vaginalis is an emerging threat in Europe, it is of great interest the study of the susceptibility to drug of isolates from patients. A total of 1,848 women who were attending from June 1994 to June 1995 in 12 health centers of the Goverment of Madrid were tested for T. vaginalis. The diagnosis of trichomoniasis was based on cultivation the cervical or vaginal specimens in tubes cointaining 2 ml of Diamond's medium (Diamond 1957). Initially, endocervical samples were taken for culture, being examined a total of 381 women with negative result for T. vaginalis. So, the 1,467 new samples were obtained from vaginal site. Vaginal specimens were obtained during the gynaecological examination on cotton-tipped applicators that were immediately seeded in the culture tubes. The bottom portion of the swab was broken off into the tubes. The cultures were incubated for 24 h at 37ºC and 5% CO2 in air. Microscopic examination was made for every specimen first at x100 and then at x400 for motile trichomonads. All negative cultures were again incubated at the same conditions above mentioned and were examined at 7 days by using exactly the same procedure of the first microscopic examination. All the isolates from positive specimens were then axenized by daily reseedings in fresh Diamond's medium containing 500 µg/ml streptomycin, 500 UI/ml penicillin and 100,000 U/ml nistatin and cryopreserved in liquid N2. In order to know the pathogenicity of each isolate, batches of 10 NMRI mice, bred under standard conditions in our laboratory were used for experimental infections. Animals weighed 20-25 g at the beginning of the experiments. To inoculate the animals, 107 trichomonads from axenic cultures were injected by the intraperitoneal route. Surviving animals were sacrified at day 15 postinfection. Both surviving animals and those that had died earlier were necropsied in order to determine the index of pathogenicity according Nogal Ruiz et al. (1997). Briefly, mortality, ascites, and the gross damage produced to the peritoneum, spleen, pancreas and stomach, and to the visceral and diaphragmatic liver faces were numerically valued to a maximum of 100 points. Stastitical differences between the pathogenicity indexes of every isolate and the reference strain were calculated by using the nonparametric Mann-Whitney U analysis. Susceptibility to metronidazole was determined by seeding 100,000 organisms/ml in glass tubes containing a final volume of 2 ml. Cultures were incubated at 37ºC and 5% CO2 in air. Metronidazole was dissolved in saline solution and added to the cultures 6 h after seeding. Twenty four hours later, viable protozoa were assessed after incubation in the presence of trypan blue using a Neubauer chamber. Three concentrations were probed, and every assayed in sextuplicate. Percentages of reduction were calculated with respect to the growth control as follows: Percentage of reduction = 100-(GR metronidazole/GR control)x100 being the growth rate (GR) the relation between the number of viable protozoa at 24 h and the number counted 6 h after seeding. C1:NIH and JH 31A no. 4 T. vaginalis strains, both from American Type Culture Collection, were used as reference for pathogenicity and sensitivity to metronidazole assays, respectively. Only 18 of 1,467 (1.2%) women had a T. vaginalis infection as diagnosed by culture. If trichomoniasis serves as a marker for other STDs (Rein 1990), the low prevalence found in global population from Madrid could demonstrate how the control is improving, because of the regular access to health care. However, the size and heterogenicity of the population surveyed obligates to consider the results about prevalence with caution. Only 6 (33.3%) of the women infected presented symptomatic infection, being the vaginal discharge (22.2%) and vulvovaginal pruritus (11.1%) the most common presenting complaints. Moreover, 50% of the women who harbored T. vaginalis revealed concomitant infection with Candida. Two characteristics were selected to study the biological variability of the natural isolates of T. vaginalis: pathogenicity to mice (Table I) and susceptibility to metronidazole (Table II). Although some attempts (Bhatt et al. 1997) to correlate the clinical picture in the natural hosts and pathogenicity in mice have failed, Teras and Roigas (1966) had found that the occurence of strains with higher virulence for mice was considerably lower in patients with latent and chronic disease than in those with acute and subacute trichomoniasis. Other studies (Kulda 1990, Malyszko et al. 1991) about the correlation between relative virulence of T. vaginalis strains for murine and human hosts have been reported. According to Kulda (1990), the severity of an experimental infection with the parasite, although dependent on the responsiveness of the individual animal, reflects the inherent virulence of the inoculated strain. As an attempt to find differences among isolates, we used a murine model standardized recently (Nogal Ruiz et al. 1997). As could be expected, a broad variability was obtained, ranging the pathogenicity indexes from 9 to 75. When compared to reference strain C1:NIH, three of the new isolates, those named 208, 1807 and 17, were found to be significantly more pathogenic for mice. In a previous paper (Escario et al. 1995) the maximum value we found for pathogenicity index of five other Spanish clinical isolates was 43, so indicating the high potential pathogenicity of the isolate 208. Regarding to metronidazole resistance tests, all the isolates could be termed as non-resistant since values revealed slight differences among the here studied isolates. All of them showed some growth inhibition after incubation for 24 h with 0.5 µg metronidazole/ml (3 µM), which is according to Meingassner et al. (1978). Recently, Snipes et al. (2000) have performed in U.S.A. a genetic analyses on 109 clinical isolates of T. vaginalis. They demonstrate a high level of relatedness among isolates with in vitro metronidazole resistance. In spite of the existence of the genetic markers suggested by the authors, it must be considered that clinical isolates of T. vaginalis exhibit different degrees of susceptibility to metronidazole. In our work, it is moreover noteworthy the fact that the less susceptible isolate (208) is just the most pathogenic to mice. Although new assays are need to find a possible relation between both characteristics in T. vaginalis, at moment this work has provide interesting biological data that can be useful to access pathogenicity assays and pharmacological screening.
ACKNOWLEDGMENTS
To all the involved health centers for providing us with the Trichomonas vaginalis isolates and Government of Madrid for technical assistance. REFERENCES
Copyright 2002 Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc02171t2.jpg] [oc02171t1.jpg] |
| |||||||||

{kind=link}
{kind=link}