
|
Memórias do Instituto Oswaldo Cruz
Fundação Oswaldo Cruz, Fiocruz
ISSN: 1678-8060 EISSN: 1678-8060
Vol. 97, Num. 7, 2002, pp. 947-952
|
Mem Inst Oswaldo Cruz, Rio de
Janeiro, Vol. 97(7), October
2002, pp. 947-952
High Prevalence
Anti-Trypanosoma cruzi Antibodies, among Blood Donors in the State
of Puebla, a Non-endemic Area of Mexico
MC Sánchez-Guillén/***,
C Barnabé***, JF Guégan***, M Tibayrenc***, M Velásquez-Rojas,
J Martínez-Munguía*, H Salgado-Rosas, E Torres-Rasgado, MI Rosas-Ramírez**,
R Pérez-Fuentes****/+
Laboratorio de Parasitología,
Centro de Investigación Biomédica de Oriente *Banco Central de
Sangre **Coordinación Delegacional de Epidemiología, Hospital
de Especialidades, Centro Médico Nacional Manuel Ávila Camacho,
IMSS Puebla, México ***Centre d'Etude sur le Polymorphisme des Micro-organismes,
Institute de Recherche pour le Devélopement, Montpellier, France ****Facultad
de Medicina, Benemérita Universidad Autónoma de Puebla, Puebla,
México
+Corresponding author and permanent address: Facultad
de Medicina, Benemérita Universidad Autónoma de Puebla, 13 Sur
2901, Col. Volcanes, Puebla, México. Fax: +52-222-243.14-44. E-mail:
rycardoperez@hotmail.com
This research was
supported by a grant from the FOSIZA-CONACYT 960802009.
Received 10 December 2001
Accepted 26 June 2002
Code Number: oc02216
Blood transfusion is the second
most common transmission route of Chagas disease in many Latin American countries.
In Mexico, the prevalence of Chagas disease and impact of transfusion of
Trypanosoma cruzi-contaminated blood is not clear. We determined the seropositivity
to T. cruzi in a representative random sample, of 2,140 blood donors
(1,423 men and 647 women, aged 19-65 years), from a non-endemic state of almost
5 millions of inhabitants by the indirect hemagglutination (IHA) and enzyme
linked immunosorbent assay (ELISA) tests using one autochthonous antigen from
T. cruzi parasites, which were genetically characterized like TBAR/ME/1997/RyC-V1
(T. cruzi I) isolated from a Triatoma barberi specimen collected
in the same locality. The seropositivity was up to 8.5% and 9% with IHA and
ELISA tests, respectively, and up to 7.7% using both tests in common. We found
high seroprevalence in a non-endemic area of Mexico, comparable to endemic countries
where the disease occurs, e.g. Brazil (0.7%), Bolivia (13.7%) and Argentina
(3.5%). The highest values observed in samples from urban areas, associated
to continuous rural emigration and the absence of control in blood donors, suggest
unsuspected high risk of transmission of T. cruzi, higher than those
reported for infections by blood e.g. hepatitis (0.1%) and AIDS (0.1%) in the
same region.
Key words:Chagas disease - seroprevalence
- blood donors - antibodies to Trypanosoma cruzi - autochthonous antigens
- Puebla - Mexico
Chagas disease, caused by the protozoan
parasite Trypanosoma cruzi, is now ranked as the most serious parasitic
disease of the Americas with an economic impact far outranking the combined
effects of the other parasitic diseases such as malaria, schistosomiasis and
leishmaniasis (Dias & Schofield 1999).
Current World Health Organization
estimation indicates about 16 to 18 millions people infected with T. cruzi
(WHO 1991). Sixty percent of them live in urban areas, and about 50% are
in a latent period. Therefore, since many infected people are potential blood
donors, one can expect that a further 100 millions are at risk of contracting
the disease (Schmunis 1991, Moncayo 1992, Moraes-Souza & Bordin 1996, Dias
& Schofield 1998).
Following the recent emphasis of
public health policies on vector control (Hayes & Schofield 1990), blood
transfusion has now become one of the most significant routes for Chagas disease
transmission (Dias 1992, Dodd 1998).
During the past decades, because
of the migration from rural to urban areas, while decreasing the rural population
exposed to infected vectors (Quintero et al. 1990), Chagas disease became frequent
in cities and a health problem in a non endemic countries, where it can be transmitted
vertically and by blood transmission (Schumunis 1999a) or organ transplantation
(Carvalho et al. 1997). This, thus increases the possibility of alternative
pathways to disease contamination.
To date, the status of Chagas disease
in Mexico is not clear, although an increasing number of cases of Chagas disease
has been reported (Cuartero et al. 1967, Velasco-Castrejón & García
1970, Gloss et al. 1990) since this disease was first recognized in 1940 by
Mazzotti. Thus, while the National Seroepidemiological Survey (NSS) (Velasco-Castrejón
et al. 1992) realized by the official Secretaría de Salud (SSa) showed
a prevalence of 1.6%, independent studies carried out, mainly in rural areas,
have shown that between 20-30% of the population was infected by the pathogen
(Monteon et al. 1989, Tay et al. 1992). Moreover, positive blood donors have
been detected at percentages of 0.2-17% of infected people (Goldsmith et al.
1978, Trujillo et al. 1993, Ramos-Echevarria et al. 1993, Rangel et al. 1998).
This reports highlights the need for a comprehensible evaluation of the prevalence
and risk of transmission of T. cruzi in endemic and non-endemic areas
in Mexico.
In this work we estimated the prevalence
of infection by T. cruzi in blood donors living in urban, suburban and
rural conditions from a non-endemic area, i.e. the Puebla state (Mexico), with
almost 5 millions of inhabitants, using two serological tests, i.e. enzyme linked
immunosor-bent assay (ELISA) and indirect haemagglutination (IHA), as suggested
by World Health Organization (WHO 1991), employing an autochthonous antigen
attributed to the genetic group T. cruzi I(Momen 1999).
POPULATION AND METHODS
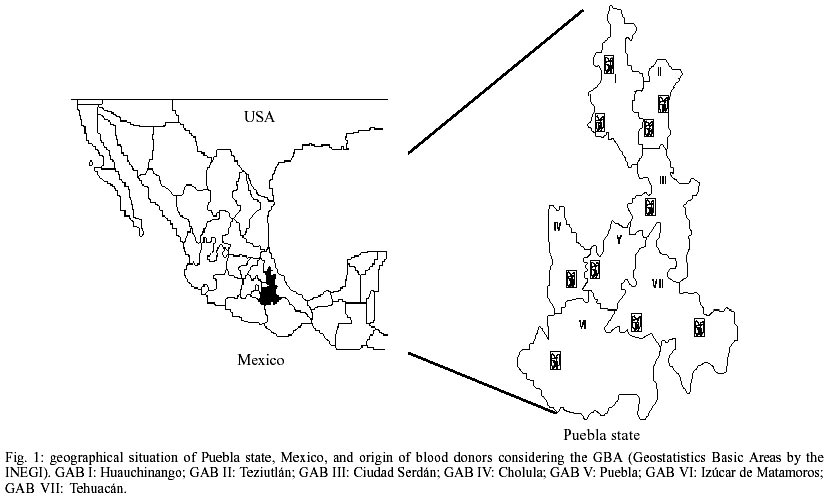
Study area - The study was
carried out in the Puebla state, which is located in the Southeast region of
Mexico (Fig. 1), in a valley up to
1,800 m above the sea level with a warm climate (average annual temperature
of 22ºC). The population is composed of around 4,579,810 inhabitants; 60%
of them live in rural and suburban conditions, which represents appropriate
ecological and socioeconomic conditions for the transmission of Chagas disease.
Studied population - Healthy
blood donors, from blood banks of the clinics and hospitals of Instituto Mexicano
del Seguro Social (IMSS), Puebla, Mexico, were selected. The criteria included
residents of Puebla, aged between 18-65, > 50 kg, health clinically and seronegative
to Hepatitis B Virus (HBC), Hepatitis C Virus (HCV), Brucella abortus
(BrA), Hepatitis B surface antigen (HBsAg), Venereal Disease Research Laboratory
(VDRL) and Human Immunodeficiency Virus (HIV) and without history of immunization,
transplantation, menstruation, pregnancy or lactation, according to the Technical
Norm for Banks of Blood protocol (TNBB). Detection of anti-T. cruzi antibodies
by the immunoenzymatic assay ELISA and IHA tests were performed in the Laboratorio
de Parasitología, Centro de Investigación Biomédica de
Oriente, IMSS, Puebla, México.
In the design of the statistic sample,
a stratified model was elaborated. The population was random-stratified considering
as total population 4,579,810 inhabitants, distributed in seven regions, denominated
Geostatistic Basic Areas (GBA) (National Institute of Geography Information,
INEGI), that include the 217 municipalities of the state (Fig.
1). This model represents the urban, suburban and rural populations of the
state, according to the socioeconomical, political and cultural levels. The
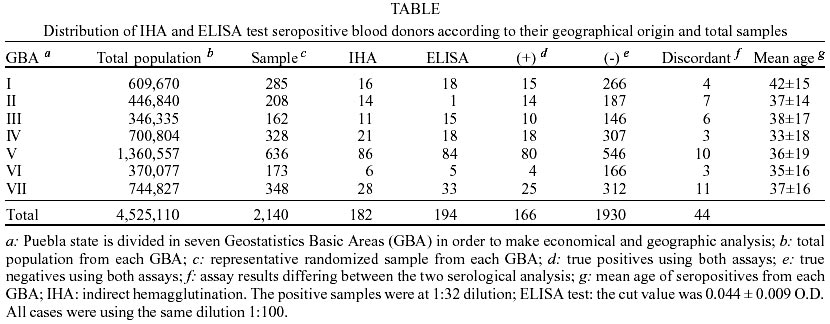
sample size was 2,140 individuals, stratified according the population density
in each GBA (Table). The sample was
determined with an estimated prevalence for T. cruzi antibodies based
on data obtained from the NSS, the desired level of precision for national estimates,
with a confidence level of 95% and a variation coefficient of 0.3, which corresponded
to a minimal expected prevalence of 0.01 (Velasco-Castrejón et al. 1992).
The level of precision was allowed to decrease for the different regions. The
rural area was characterized by the lacked of sanitary services and presence
of poor housing inhabit and coexistence with domestic and peridomestic animals.
The suburban population was identified by the poor-housing situated in peripheral
area of big cities and lacked of sanitary services and finally the urban population
included the individuals, living in an area with total sanitary services.
Serum samples - The sanguine
samples from blood donors, were collected of peripherical vein in Vacutainer
system, in each selected blood banks of the clinics, hospitals, and Banco Central
de Sangre, Hospital de Especialidades, Centro Médico Nacional Manuel
Ávila Camacho, IMSS, Puebla. The serum was separated by centrifugation
(1,200 g for 10 min), it was aliquoted in eppendorf tubes and it was frozen
at -4oC and transported to Laboratorio de Parasitología, Centro
de Investigación Biomédica de Oriente, IMSS, Puebla where it were
stored in freezing (-20º C) until use.
T. cruzi antigen characterization
- T. cruzi parasites, employed as autochthonous antigen, were obtained from
a Triatoma barberi specimen collected in the area locality, Puebla, Mexico.
The isolated parasites were characterized by Multilocus Enzyme Electrophoresis
(MLEE), RAPDs and Biodeme like TBAR/ME/1997/RyC-V1 (T. cruzi I ).
T. cruzi autochthonous antigen
preparation - Total antigen from the Puebla strain RyC-V1 were obtained
as previously reported (Pérez-Fuentes et al. 1998). In brief, the parasites
(epimastigotes) were cultured and propagated in a liver infusion tryptose medium,
supplemented with 10% fetal calf serum while growing at logarithmic phase was
harvested, then sonicated in the presence of protease inhibitors, and spun down
to 10,000 g x 30 min at 4ºC. The supernatant was used as a crude antigenic
extract whose protein concentrations, quantified by the method of Lowry were
adjusted to 1 mg/ml and stored at -70ºC.
Serological characterization -
Technique of ELISA - Briefly,polystyrene plaques (Dynatech) were sensitized
with the crude antigen extract of epimastigotes at a concentration of 100 µg/ml
in carbonates buffer pH 9.5 and blocked with bovine fetal serum to 1% in PBS-Tween
20 (0.01%). The blood donors and controls sera were diluted 1:100 and incubated
by 1 h, washed with PBS. It was employed conjugated human anti-IgG coupled to
radish peroxidase, the colorimetric reaction was developed with orto-phenilen-diamino
and peroxide of hydrogen. The reaction was stopped and it was reading at 490
nm in ELISA's reader.
Technique of IHA - The sensitization
of the blood red cells was required for this assay. Ram erythrocytes was used
at a concentration of 2.5% in buffer of phosphate pH 7.2, they were mixed with
tannic acid at a dilution of 1:60,000 and they were sensitized with autochthonous
antigen from T. cruzi at 37ºC for 20 min, they were washed themselves
with PBS pH 7.2 and adjusted at a concentration of 0.2 mg/ml. The problem sera
at dilutions 1:8, 1:32 and 1:64 were incubated by 2 h to room temperature. The
identification of the antibodies was determined by the agglutination presence
in the bottom of the wells of the plate. It was considered the title of 1:8
as infection and 1:32 as confirmatory. All samples were analyzed by triplicate
and repeated twice.
Positive and negative controls were
included in each test. A positive result was defined as titer > 1:32 for
the IHA test and > 0.200 for the ELISA. In both assays we employed the autochthonous
T. cruzi antigens. Soluble epimastigote antigen was prepared as previously
described.
RESULTS
A total of 2,140 random blood samples
of the seven areas of the Puebla were evaluated for anti T. cruzi antibodies
using ELISA and IHA tests. All subjects were > 18 years of age, weight >
50 kg, clinically healthy, and were residents from rural, suburban and urban
areas in Puebla. The average age of the individuals was 32 years old ranging
from 19 to 50 years with a female:male ratio of 1:3. All donors were seronegative
for HBC, HCV, (HBsAg), BrA, VDRL and HIV, and all of them fulfilled criteria
to Technical Norm of Bank of Blood. Due to the lack of serologic "gold
standard" for the diagnostic of Chagas disease, the sera employed in the
evaluation were characterized by both matched IHA and ELISA tests. In each case,
we tested for antibodies against T. cruzi using epimastigotes of autochthonous
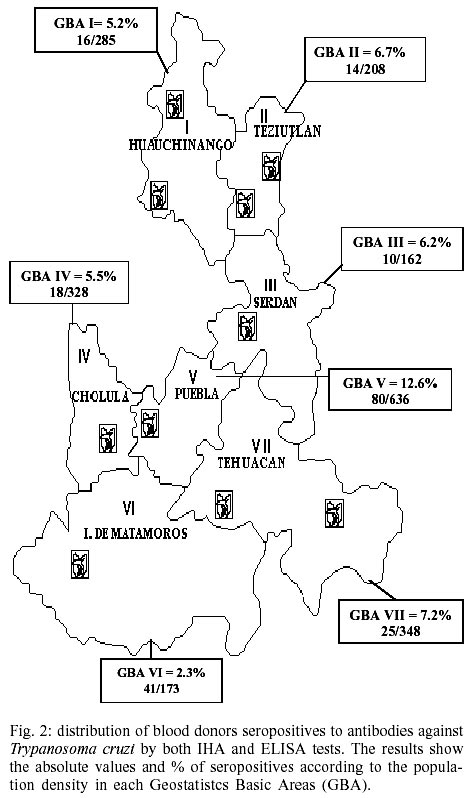
antigens. Of the 2,140 serum samples analyzed, 194 (9.1%) showed antibodies
against T. cruzi with ELISA and 182 (8.5%) for IHA techniques, respectively.
However, we considered as carriers of T. cruzi antibodies, the 166 (7.7%)
individuals (127 men and 39 women, mean age 36.8 ± 16.4), that were seropositive
to both assays, i.e. ELISA and IHA, according to WHO recommendations (1991).
Then, the samples were divided (Fig.
2) considering the distribution of seropositive blood donors for T. cruzi
antibodies by both ELISA and IHA tests and according to the stratification in
seven district regions proposed by the INEGI.
Table
illustrates the distribution of seropositive samples, including positive, negative
and discordant results, by studied areas. Prevalence rates were different between
urban, suburban and rural origins for patients tested by IHA (Fisher's exact
test with correction, p = 10-5), by ELISA (p = 2.4 x 10-4)
and by both tests (p = 10-4). In addition, comparison were also significant
between urban and suburban plus rural when plotted together by IHA (p = 10-5),
by ELISA (p = 10-5) and by both tests (p = 10-6).
DISCUSSION
While in many Latin American countries,
Chagas serological tests are mandatory for all blood donors, in Chile (Ministerio
da Saúde 1993) and in Mexico (Guzmán-Bracho et al. 1998) this
measure is applied only in endemic areas. Furthermore, screening in Mexico is
not routinely done in all endemic states (Schmunis 1999b).
The data presented in this work are
relevant because they clearly establish the seroprevalence of T. cruzi
antibodies in blood donors, and provide information on the prevalence of the
infection in Mexico, where the information regarding the importance of the transmission
of Chagas disease is either limited or under estimated.
This study shows that the seroprevalence
found in blood donors of a non-endemic area of Mexico (7.7%), i.e. the Puebla
state, is relatively high, and comparable to those found in endemic states of
others countries. These findings strongly contrast with the NSS in Mexico carried
out in 1987, and published in 1992, which showed a low prevalence of 1.6%. These
differences may be in part attributed to the fact that this last study was performed
with statistics specifically designed for the characterization of urban transmissible
diseases, such as AIDS, hepatitis, but not for rural transmissible diseases
such as Chagas disease (Velasco-Castrejón et al. 1992). Besides, our
findings (7.7%) contrast with the more recent study carried out by the official
SSa, that showed only 1.5% of national prevalence and specifically 1.8% from
Puebla (Guzmán-Bracho et al. 1998). The discrepancy could be explained
in part by the serologic tests employed (we used both ELISA and IHA assays),
strain of the parasite used in the antigen preparation (autochthonous antigen),
and mainly, by the size (random sample) and characteristic of analyzed population.
Thus, in this work was performed in 64,969 blood donors, where approximately
850,000 donations are done yearly, including samples from 18 of the 32 Mexican
states, and the study did not rely on any specific statistics.
The antibody based immunoassay play
a relevant role as diagnostic tool because of their high sensitivities. In the
particular case of Chagas disease, no serologic "gold" standard exists,
since detection of T. cruzi-specific antibodies depends on many factors.
Nevertheless, IFA is the most commonly used serologic test for Chagas disease
and, as result, is widely accepted as the gold standard (Ferreira & Moraes
de Avila 1995). Recent reports show that in-house IFA and in-house ELISA were
highly concordant (Oelemann et al. 1998). Like is suggested by Organización
Panamericana de la Salud (OPS), IHA is a screening technique while ELISA or
IFA is for confirmatory diagnosis with a higher specificity than IHA. In this
work, in total agreement with the OPS recommendations that mandatory serology
must be implemented in all countries where T. cruzi is endemic by using
at least two serological tests (OPAS 1998), we used two independent techniques,
i.e. in-house IHA and in-house ELISA with the same antigen, the last assay presented
a higher specificity to Chagas disease detection (Pérez-Fuentes et al.
1998).
However, few countries use more than
one test for blood donor screening (Schmunis 1999). A study carried out in 1998
in Cuernavaca (town of Morelos, Mexico) showed a seropositivity in blood donors
of 17%, using a commercial ELISA kit in consecutive blood samples from 318 donors
(Rangel et al. 1998).
Our findings can be explained in
part by the kind of antigen we have used in serologic tests, further studies
have suggested that the specificity of different methods depends on the selection
of an adequate antigen (Mendes et al. 1997), considering that T. cruzi
is polymorphic, and different parasite strains circulate in different areas
(Dias 1992). Then, genetic characterization of T. cruzi parasites have
shown that Mexican stocks belonging to T. cruzi I and are closely related
to each other (Bosseno et al. 2002). In Mexico, most studies have been performed
using T. cruzi antigens extracted from strains originating from other
geographical origins, mainly South America, that show different genotypes (Bucio
et al. 1999).
Previously, we have shown that assays
utilizing commercial antigens from other countries are lesser sensitive than
using T. cruzi authocthonous antigen in the diagnostic of Chagas diseases
(Pérez-Fuentes et al. 1998). Recently this finding was demonstrated by
other authors (Sánchez et al. 2001).
The specificity of our analysis was
to use autochthonous antigens from local T. cruzi strains isolated in
the same area and characterized as T. cruzi I, could be naturally reflect
locally adapted host immune response against T. cruzi natural clones
circulating in the area.
In Mexico, the infection by T.
cruzi is mainly silent. Thus, like in most countries of Latin America, Chagas
disease has become an urban disease, due to the migration of people from endemic
areas to the cities (Moraes-Souza 1999). In this work, although all of individuals
were resident of the region in study, the prevalence rate for T. cruzi
antibodies found in the blood donors of urban origin, i.e. Puebla (V Area),
were twice higher than those of rural regions, where the identification of T.
barberi, the insect vector and the conditions for natural infection and
transmission exist (unpublished data, Pérez-Fuentes R et al.). This could
be explained by the migration of infected people from rural to urban areas as
Puebla, capital city, due to the poor socioeconomic as in many Latin American
countries. This could be suggest that urban transmission is now overcoming the
classical rural transmission.
Many recent reports (Guzmán-Bracho
et al. 1998, Dumontiel 1999, Schmunis 1999) show the need for a comprehensive
evaluation of the prevalence and distribution of Chagas disease in Mexico. In
the present study, the identification of substantial prevalence of seropositive
blood donors to T. cruzi suggests the existence of a high risk of contamination
by blood transfusion. As others have proposed, the routine programs of serologic
screening with immunological techniques with high sensibility and specificity
definition, i.e. T. cruzi antigens extracted from local strains, are
urgently needed and applied. This should be done in all areas, including those
that are considered as non-endemic.
The last years, fortunately the situation
has improved in Mexico. The ministry of Health has approved a law about screening
for anti-T.cruzi antibodies in the whole territory. Also, epidemiological
surveillance and vector control programs have started to inform regulation (Guzmán-Bracho
2001).
Our results confirm that blood transfusion
is an important parameter in Chagas disease transmission in Mexico, besides
the classical vectorial transmission. Vector control therefore must be completed
by adequate screening measures in all Mexican transfusion centers.
ACKNOWLEDGEMENTS
To the personal from Clínicas
Comunitarias and Banco Central de Sangre del Centro Médico Nacional Manuel
Ávila Camacho del Instituto Mexicano del Seguro Social for the facilities
for this work; to the staff of U.M.R. 9926 C.N.R.S.-I.R.D. in Montpellier, France
for their invitation to come for a postdoctoral fellowship of RPF financed by
CONACyT (00208) and MCSG financed by IMSS.
REFERENCES
- Bosseno MF, Barnabé C,
Magallón-Gastélum E, Lozano-Kasten F, Ramsey J, Espinoza B,
Breniére SF 2002. Predominance of Trypanosoma cruzi lineage
I in Mexico. J Clin Microbiol 40: 627-632. [
Medline
]
- Bucio MI, Cabrera M, Segura EL,
Zenteno E, Salazar-Schettino M 1999. Identification of immunodominant antigens
in Mexican strains of Trypanosoma cruzi. Immunol Invest 28:
257-268. [ Medline
]
- Carvalho MF, de Franco MF, Soares
VA 1997. Amastigotes forms of Trypanosoma cruzi detected in a renal
allograft. Rev Inst Med Trop São Paulo 39: 223-226.
[ Medline
] [ Lilacs
] [ SciELO
]
- Cuartero L, Ponce D, Recco R 1967.
Cinco nuevos casos de enfermedad de Chagas en Zacatecas y Jalisco, en la Republica
Mexicana. Rev Invest Salud Publica Mex 27: 29-32.
- Dias JC 1992. Epidemiology of
Chagas disease. In S Wendel, Z Brener, ME Camargo, A Rassi (eds), Chagas
Disease (American Trypanosomiasis): its Impact on Transfusion and Clinical
Medicine, International Society of Blood Transfusion, São Paulo,
p. 49-80.
- Dias JC, Schofield CJ 1998. Controle
da transmissão transfusional da doença de Chagas na iniciativa
de cone sul. Rev Soc Bras Med Trop 31: 373-383.
- Dias JC, Schofield CJ 1999. The
evolution of Chagas disease (American trypanosomiasis). Control after 90 years
since Carlos Chagas discovery. Mem Inst Oswaldo Cruz 94 (Suppl.
I): 103-121.
- Dodd RY 1998. Transmission of
parasites by blood transfusion. Vox Sang 74 (Suppl. 2): 161-163.
- Dumontiel E 2001. Update on Chagas
disease in Mexico. Salud Publica Mex 41: 359.
- Ferreira AW, Moraes de Avila SL
1995. Laboratory diagnosis of Chagas heart disease. São Paulo Med
J/RPM 113: 767-771.
- Gloss G, Barrera MR, Monteon VM,
Reyes PA 1990. Tripanosomiasis americana y cardiopatia chagasica cronica en
el Instituto Nacional de Cardiologia Ignacio Chavez. Arch Inst Cardiol
Mex 60: 261-266. [ Medline
]
- Goldsmith RS, Zarate R, Kagan
I, Cedeño-Ferreira J, Galindo-Vasconcelos M, Antonio-Paz E 1978. El
potencial de la transmision en la enfermedad de Chagas por transfusion sanguinea:
hallazgos serologicos entre donadores en el estado de Oaxaca. Salud Publica
Mex 20: 439-444. [ Medline
]
- Guzman-Bracho C 2001. Epidemiology
of Chagas disease in Mexico: an update. Trends Parasitol 17: 372-376.
- Guzmán-Bracho C, García-García
L, Floriani-Verdugo J, Guerrero-Martínez S, Torres-Cosme M, Ramírez-Melgar
C, Velasco-Castrejón O 1998. Riesgo de transmisión de Trypanosoma
cruzi por transfusión de sangre en Mexico. Rev Panam Salud Pub
4: 94-99.
- Hayes RJ, Schofield CJ 1990. Estimación
de las tasas de incidencia de infecciones y parasitosis crónicas en
base a su prevalencia: la enfermedad de Chagas en América Latina. Bol
Oficina Sanit Panam 108: 308-316. [ Medline
] [ Lilacs
]
- Mendes RP, Hoshino-Shimizu S,
Moura da Silva AM, Mota I, Heredia RA, Luquetti AO, Leser PG 1997. Serological
diagnosis of Chagas disease: a potential confirmatory assay using preserved
protein antigens of Trypanosoma cruzi.J Clin Microbiol 35: 1829-1834.
[ Medline
]
- Ministerio da Saúde, Brasil
1990-1991 1993. Coordenação de sangue e hemoderivados. Relatório
de atividades: Anexo IX. Ministerio de Salud, Chile 1990-1991. Diagnostico
de la situacion de los bancos de sangre y medicina transfusional en Chile.
Ser Inf Tecnicos: 14.
- Momen H 1999. Taxonomy of Trypanosoma
cruzi: commentary on characterization and nomenclature. Mem Inst Oswaldo
Cruz 94: 181-184. [ Lilacs
] [ SciELO
]
- Moncayo A 1992. Chagas disease:
epidemiology and prospects for interruption of transmission in the Americas.
World Health Stat Q 45: 276-279. [ Medline
]
- Monteón VM, Sosa T, Reyes
PA 1989. Serological test for American trypanosomiasis: a comparative study.
Rev Latinoam Microbiol 31: 35.
- Moraes-Souza H 1999. Chagas infection
transmission control: situation of transfusional transmission in Brazil and
other countries of Latin America. Mem Inst Oswaldo Cruz 94 (Suppl.
I): 419-423.
- Moraes-Souza H, Bordin JO 1996.
Strategies for prevention of transfusion associated Chagas disease. Transfus
Med Rev 10: 161-170. [ Medline
]
- OPAS-Organizacion Panamericana
de la Salud 1998. Situación de los bancos de sangre en América
Latina. 1996: marcadores serológicos para enfermedades transmisibles
a donantes de sangre. Bol Epidemiol 19: 11-13.
- Oelemann WM, Teixeira MG, Da Costa
GV, Borges-Pereira J, De Castro JA, Rodríguez-Coura J, Peralta JM 1998.
Evaluation of three comercial enzyme-linked immunosorbent assays for diagnosis
of Chagas disease. J Clin Microbiol 36: 2423-2427.
- Pérez-Fuentes R, Sánchez-Guillén
MC, González-Álvarez C, Monteón VM, Reyes PA, Rosales-Encina
JL 1998. Humoral nitric oxide levels and antibody immune response of symptomatic
and indeterminate Chagas disease patients to commercial and autochthonous
Trypanosoma cruzi antigen. Am J Trop Med Hyg 58: 715-720.
[ Medline
]
- Quintero ZT, Troncoso MC, Arnesi
N, Boggio G, Sánchez S 1990. Comportamientos migratorios en dadores
de sangre y las probabilidades de transmitirla por medio de la transfusión.
Bol Chil Parasitol 24: 88-93.
- Ramos-Echevarria AA, Monteón-Padilla
VM, Reyes-López PA 1993. Detección de anticuerpos contra Trypanosoma
cruzi en donadores de sangre. Salud Publica Mex 35: 56-64.
[ Medline
]
- Rangel H, Gatica R, Ramos C 1998.
Detection of antibodies against Trypanosoma cruzi in donors from a
blood bank in Cuernavaca, Morelos, Mexico. Arch Med Res 29:
79-82.
- Sánchez B, Monteón
V, Reyes PA, Espinoza B 2001. Standardization of micro-enzyme-linked immunosorbent
assay (ELISA) and western blot for detection of Trypanosoma cruzi antibodies
using extracts from mexican strains as antigens. Arch Med Res 32: 382-388.
- Schmunis GA 1991. Trypanosoma
cruzi, the etiologic agent of Chagas disease: status in the blood supply
in endemic and non endemic countries. Transfusion 31: 547-557.
[ Medline
]
- Schmunis GA 1999a. Prevention
of transfusional Trypanosoma cruzi infection in Latin America. Mem
Inst Oswaldo Cruz 94 (Suppl. I): 93-101.
- Schmunis, GA 1999b. Risk of Chagas
disease through transfusions in the Americans. Medicina (B Aires) 59
(Suppl. 2): 125-134.
- Tay J, Schenone H, Sánchez
JT, Robert L 1992. Estado actual de los conocimientos sobre la enfermedad
de Chagas en la Republica Mexicana. Bol Chil Parasitol 47: 43-53.
[ Medline
] [ Lilacs
]
- Trujillo F, Lozano F, Soto M,
Hernández R 1993. Prevalencia de infeccion a Trypanosoma cruzi
en donadores de sangre en el estado de Jalisco, Mexico. Rev Soc Bras Med
Trop 26: 89.
- Velasco-Castrejón O, García
L 1970. Estudio clínico y epide-miológico de un nuevo caso humano
de enfermedad de Chagas en la Republica Mexicana. Prensa Med Mex 35:
438.
- Velasco-Castrejón O, Valdespino
JL, Tapia-Conyer R, Salvatierra B, Guzmán-Bracho C, Magos C, Llausas
A, Gutiérrez G, Sepúlveda J 1992. Seroepidemiología de
la enfermedad de Chagas en Mexico. Salud Publica Mex 34: 186-196.
[ Medline
]
- WHO-World Health Organization
1991. Control of Chagas disease. Report of a WHO Expert Committee, WHO Technical
Report Series 811: 95.
Copyright 2002 Instituto Oswaldo
Cruz - Fiocruz
The following images related to this document are available:
Photo images
[oc02216f2.jpg]
[oc02216f1.jpg]
[oc02216t1.jpg]
|

{kind=link}
{kind=link}
{kind=link}