
|
Memórias do Instituto Oswaldo Cruz
Fundação Oswaldo Cruz, Fiocruz
ISSN: 1678-8060 EISSN: 1678-8060
Vol. 97, Num. 7, 2002, pp. 953-957
|
Mem Inst Oswaldo Cruz, Rio de
Janeiro, Vol. 97(7), October
2002, pp. 953-957
Prevalence and
Genotypes of GB Virus C/Hepatitis G Virus among Blood Donors in Central Brazil
Luciana A Oliveira, Regina MB Martins/+,
Megmar AS Carneiro, Sheila A Teles, Simonne A Silva, Divina DP Cardoso, Elisabeth
Lampe*, Clara FT Yoshida*
Instituto de Patologia Tropical e
Saúde Pública, Universidade Federal de Goiás, Caixa Postal
131, 74605-050 Goiânia, GO, Brasil *Departamento de Virologia, Instituto
Oswaldo Cruz-Fiocruz, Rio de Janeiro, RJ, Brasil
+Corresponding
author. Fax: +55-62-202.3066. E-mail: rbringel@terra.com.br
Received 7 March 2002
Accepted 12 June 2002
This
work received financial support from Conciteg and CNPq.
Code Number: oc02217
A survey was conducted in a blood
donor population of Central Brazil aiming to investigate the prevalence of GB
virus C (GBV-C)/hepatitis G virus (HGV) infection and also to analyze the virus
genotypes distribution. A total of 241 voluntary blood donors were interviewed
at the State Blood Bank in Goiânia, State of Goiás, Brazil. Blood
samples were collected and serum samples tested for GBV-C/HGV RNA by polymerase
chain reaction. Genotypes were determined by restriction fragment length polymorphism
(RFLP) analysis. Seventeen samples were GBV-C/HGV RNA-positive, resulting in
a prevalence of 7.1% (95% CI: 4.2-11.1). A significant trend of GBV-C/HGV RNA
positivity in relation to age was observed, with the highest prevalence in donors
between 29-39 years old. Ten infected individuals were characterized by reporting
parenteral (30%), sexual (18%), both (6%) and intrafamiliar (6%) transmission.
However, 7 (40%) GBV-C/HGV RNA-positive donors did not mention any potential
transmission route. RFLP analysis revealed the presence of genotypes 1 and 2
of GBV-C/HGV; more precisely, 10 (58.9%) samples were found belonging to the
2b subtype, 4 (23.5%) to the 2a subtype, and 3 (17.6%) to genotype 1. The present
data indicate an intermediate endemicity of GBV-C/HGV infection among this blood
donor population, and a predominant circulation of genotype 2 (subtype 2b) in
Central Brazil.
Key words: hepatitis G virus - GB
virus C - blood donors - Goiânia - Central Brazil
GB virus C (GBV-C) and hepatitis
G virus (HGV) are independent isolates of the same virus which were identified
as possible aetiological agent of viral hepatitis in humans (Simons et al. 1995,
Linnen et al. 1996). The GBV-C/HGV can cause persistent infection, but its role
in causing liver diseases is still uncertain (Bowden 2001). However, some studies
showed that infection with GBV-C/HGV can be associated with lower progression
of human immunodeficiency virus (HIV) disease in coinfected patients (Lefrère
et al. 1999, Yeo et al. 2000, Tillmann et al. 2001, Xiang et al. 2001).
The GBV-C/HGV genome consists of
a single-stranded positive sense RNA of approximately 9.4 kb which has characteristics
of a flavivirus-like genome as in the case of the hepatitis C virus (HCV) (Muerhoff
et al. 1995), except that unlike HCV, the 5' noncoding region (5' NCR) of GBV-C/HGV
is variable, and can be used initially to classify natural isolates into three
genotypes. Genotype 1 is frequently found in West Africa, genotype 2 predominates
in the USA and Europe, and genotype 3 is commonly observed in parts of Asia
(Muerhoff et al. 1996, 1997, Mukaide et al. 1997, Okamoto et al. 1997, Katayama
et al. 1998). In addition to this classification, 2 novel genotypes were identified.
Genotype 4 was described in Myanmar and Vietnam (Naito et al. 2000), and genotype
5 has been found in South Africa (Tucker et al. 1999, Tucker & Smuts 2000).
GBV-C/HGV is transmitted through
blood transfusion and blood components (Schmidt et al. 1996, Roth et al. 1997,
Heuft et al. 1998). Epidemiological data suggest that this virus is also spread
by sexual and vertical transmission (Bourlet et al. 1999, Stark et al. 1999,
Wejstål et al. 1999). However, little is known about other modes of transmission
that could explain the high prevalence and worldwide distribution of this virus.
In Brazil, high GBV-C/HGV RNA prevalence
rates were found in blood donors from Southeast and Northeast regions (Bassit
et al. 1997, Lampe et al. 1998a, Goubau et al. 1999, Pinho et al. 1999). As
data concerning GBV-C/HGV infection in other Brazilian regions are still rare,
we sought to assess the prevalence of GBV-C/HGV RNA in blood donors in Central
Brazil and also to investigate the virus genotypes distribution.
MATERIALS AND METHODS
Subjects - From June to September
2000, a total of 241 voluntary blood donors accepted for blood donation, after
clinical evaluation, at the State Blood Bank in Goiânia, State of Goiás
(1,000,000 inhabitants), Central Brazil, were invited to take part of this study,
and informed consent was obtained from all participants. The study was approved
by the Ethical Committee of the Federal University of Goiás.
A standardized form was used to collect
sociodemo-graphic and data as number of previous blood transfusions, acupuncture,
tattooing, surgery, intravenous drug use, dental procedure with non-licensed
dentist, multiple sex partners, sexually transmitted diseases, and possible
household contact with hepatitis.
Serological tests - Blood
samples were collected from all donors and sera were stored at -20ºC. They
were screened for hepatitis B surface antigen (HBsAg), hepatitis B core antibody
(anti-HBc) and hepatitis C antibody (anti-HCV) by enzyme-linked immunosorbent
assays (ELISA) (Abbott Laboratories, USA). All samples were also tested for
alanine aminotransferase (ALT) levels by a colorimetric method (Dolles Laboratory,
Brazil).
Detection of GBV-C/HGV RNA
- All samples were submitted to RNA extraction, reverse transcription, and a
nested polymerase chain reaction (PCR) with primers complementary to the conserved
area of the NS5 region of the genome, essentially as described by Lampe et al.
(1997).
GBV-C/HGV genotyping - GBV-C/HGV
RNA-positive samples were amplified by PCR using primers complementary to the
5' non-coding region (NCR). Genotypes were determined by means of RFLP method
(Quarleri et al. 1999). Briefly, amplicons were initially cleaved with Hinf
I, and depending on the restriction pattern observed, a second digestion was
performed either with Aci I or Aat II. Restriction fragments were
resolved in ethidium bromide-stained 3% agarose gels.
Statistical analysis - Prevalence
and 95% confidence intervals (CI) were calculated. Chi-square test, Chi-square
for trend test or Fisher's exact test were performed to evaluate the distribution
of characteristics associated with GBV-C/HGV infection. Statistical significance
was assessed at the 0.05 probability level in all analyses. Statistical evaluations
were performed using Epiinfo 6.0 program developed by the Centers for Disease
Control and Prevention (Atlanta, GA).
RESULTS
The studied population ranged in
age from 18 to 60 years (mean ± SD = 30.2 ± 8.5 years). The majority
of the blood donors (86.7%) were men. Almost 70% of them earned less than U$
200 per month and also had less than 8 years of schooling. Forty-eight (19.9%)
were first-time blood donors and 193 (80.1%) were regular donors. This population
consisted of relatives or close friends of hospitalized patients needing blood
transfusions.
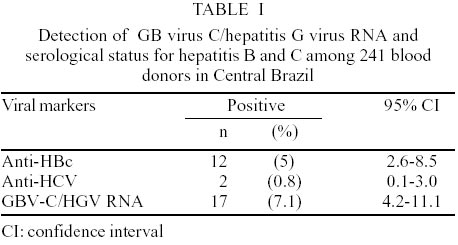
As shown in Table
I, a prevalence of 7.1% (95% CI: 4.2-11.1) was found for GBV-C/HGV infection.
This donor population showed positivity rates of 5% and 0.8% for hepatitis B
(anti-HBc) and C (anti-HCV), respectively. All serum samples were negative for
HBsAg.
Analysis of the characteristics of
this population showed that only age was significantly associated with GBV-C/HGV
infection. This infection reached a peak at an age range from 29 to 39 years
old; 13.5% of the blood donors were infected. Moreover, 2.5% of the age group
under 28 years and 6.1% of age group over 40 years were GBV-C/HGV RNA- positive
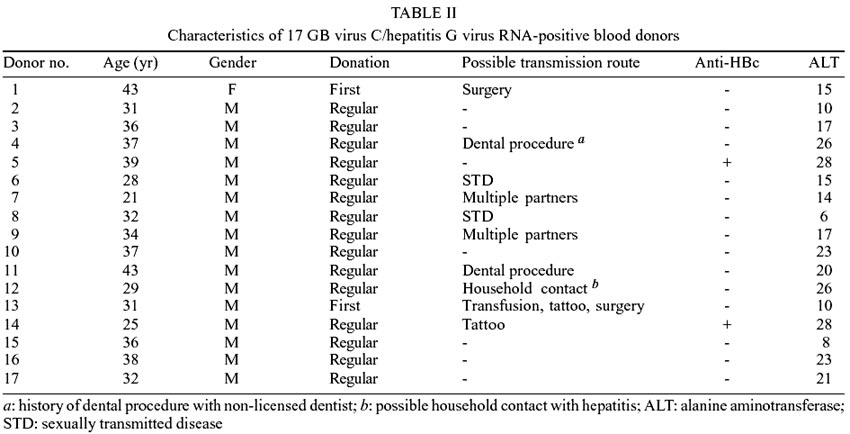
(c² for trend = 9.98; p = 0.018). On the other
hand, potential transmission routes associated with parenteral (30%), sexual
(18%), both (6%) and intrafamiliar (6%) were reported by GBV-C/HGV RNA-positive
donors. However, 40% of them did not mention any known source for infection
(Table II). GBV-C/HGV RNA-positive
individuals ranged in age from 21 to 43 years. All but one were men. The majority
of them were regular blood donors. Two of these donors (nos. 5 and 14) were
anti-HBc positive. All GBV-C/HGV infected individuals had normal ALT levels.
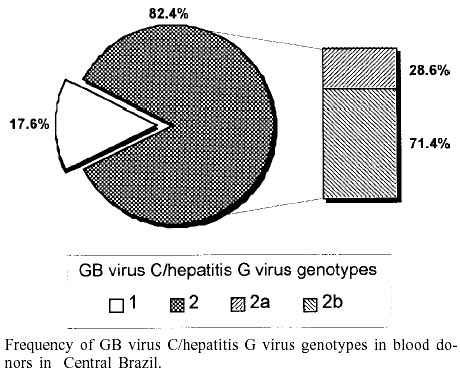
All 17 GBV-C/HGV RNA-positive samples
were genotyped by RFLP pattern. It was observed that 3 (17.6%) were of genotype
1 and 14 (82.4%) of genotype 2. Of these, 4 isolates belonged to the 2a subtype
and 10 to the 2b subtype (Figure).
DISCUSSION
Epidemiological investigations demonstrated
that GBV-C/HGV RNA prevalence among blood donors ranges from 0.5-4% in the USA,
Europe and Japan (Orito et al. 1996, Gutierrez et al. 1997, Nübling et
al. 1997, Blair et al. 1998, Mercier et al. 1999, Sauleda et al. 1999) to 10-18.9%
in some African countries (Casteling et al. 1998, El-Zayadi et al. 1999, Sathar
et al. 1999). In South America, it has also been reported at a varying range
from 5.5% in Argentina (Oubiña et al. 1999) to 14.6% in Bolivia (Konomi
et al. 1999). In Brazil, rates of 9% and 10% were detected in blood donors in
São Paulo and Rio de Janeiro (Southeastern region), respectively (Bassit
et al. 1997, Lampe et al. 1998a). In addition, 5.2% and 6.5% of donors with
normal and elevated ALT levels were GBV-C/HGV RNA-positive (Pinho et al. 1999).
A prevalence of 8.6% was found in Fortaleza (Northeastern region) (Goubau et
al. 1999). Thus, the prevalence of 7.1% found in blood donors in Goiânia
could be placed in an intermediate position.
The highest prevalence of GBV-C/HGV
RNA was seen in the group from 29 to 39 years (13.5%). A similar finding of
age-specific prevalence has been reported by Konomi et al. (1999), with a peak
at an age range from 20 to 39 years in healthy Bolivian individuals. In addition,
among 170 blood donors in Rio de Janeiro, the seropreva-lence of antibody against
GBV-C/HGV envelope E2 protein increased with age, from 5.6% (group with ages
between 18 and 24 years) to 35.3% (donors from 43 to 60 years) (Lampe et al.
1998b). These data may suggest a role for sexual transmission of GBV-C/HGV.
In the present study, prevalence
rates of 5% and 0.8% were found for hepatitis B and C, respectively. Of the
17 GBV-C/HGV RNA-positive blood donors, two were positive for anti-HBc, but
negative for HBsAg, and none of them was coinfected by HCV. In addition, no
association was found between GBV-C/HGV RNA status and serum ALT levels. These
data indicate that this virus has been independently widespread in healthy individuals
in Central Brazil.
We observed the characteristics of
the GBV-C/HGV RNA-positive donors. Ten individuals had exposure to one or more
factors associated with parenteral (30%), sexual (18%), both (6%) and intrafamiliar
(6%) transmission. However, it is interesting to note that 40% of the infected
donors did not mention any identifiable source of infection, but they earned
less than US$ 200 per month and had a low level of education. Thus, low socioeconomic
status and poor hygienic conditions occurring in developing countries may contribute
to GBV-C/HGV dissemination (Konomi et al. 1999).
To analyze the genetic diversity
of GBV-C/HGV isolates among blood donors in Central Brazil, all GBV-C/HGV RNA-positive
samples were genotyped by RFLP. Three samples (17.6%) belonged to genotype 1
and the remaining 14 (82.4%) to genotype 2. These data demonstrate the simultaneous
circulation of both genotypes, already reported to be predominant in West Africa
(genotype 1) and USA/Europe (genotype 2) (Tucker & Smuts 2000). Recently,
the same genotypes were detected in 35 serum samples in a Brazilian rural population
(Northeastern region); more precisely, 82.9% and 17.1% were characterized as
genotypes 2 and 1, respectively (Gallian et al. 1998). Also, Lampe et al. (1998b)
showed that 31 isolates from individuals living in Rio de Janeiro (Southeastern
region) belonged to three clusters, 2 of which were classified as genotypes
1 and 2. The presence of both genotypes in Brazil is likely to reflect the European
and African origin of the population. In the present study, genetic diversity
of genotype 2 revealed that 4 donors were infected with subtype 2a and 10 with
subtype 2b. In Argentina, genotype 2 was also predominant among blood donors,
and subtypes 2a and 2b were equally detected (Oubiña et al. 1999). Genotype
3 was not observed in Brazilian isolates in spite of immigration from Asian
countries, but it was found in other populations of South America, such as native
Indians from Colombia (Tanaka et al. 1998) and in Bolivians (Konomi et al. 1999).
In conclusion, our data point out
an intermediate endemicity of GBV-C/HGV infection in Central Brazil, and that
the parenteral route was the presumed means of virus transmission for only one-third
of the infected blood donors. This investigation also demonstrates the simultaneous
circulation of genotypes 1 and 2, with a high prevalence of subtype 2b of GBV-C/HGV
in the study population.
REFERENCES
- Bassit L, Kleter B, Santos GR,
Maertens G, Sabino E, Chamone D, Quint W, Sáez-Alquézar A 1997.
Hepatitis G virus: prevalence and sequence analysis in blood donors of São
Paulo, Brazil. Vox Sang 74: 83-87.
- Blair CS, Davidson F, Lycett C,
Mcdonald DM, Haydon GH, Yap PL, Hayes PC, Simmonds P, Gillon J 1998. Prevalence,
incidence and clinical characteristics of hepatitis G virus/GB virus C infection
in Scottish blood donors. J Infect Dis 178: 1779-1782. [ Medline
]
- Bourlet T, Guglielminotti C, Evrard
M, Berthelot P, Grattard F, Frésard A, Luncht FR, Pozzetto B 1999.
Prevalence of GBV-C/hepatitis G virus RNA and E2 antibody among subjects infected
with human immunodeficiency virus type 1 after parenteral or sexual exposure.
J Med Virol58: 373-377.
- Bowden S 2001. New hepatitis viruses:
contenders and pretenders. J Gastroenterol Hepatol 16: 124-131.
[ Medline
]
- Casteling A, Song E, Sim J, Blaauw
D, Heyns A, Schweizer R, Margolius L, Kuun E, Field S, Schoub B, Vardas E
1998. GB virus C prevalence in blood donors and high risk groups for parenterally
transmitted agents from Gauteng, South Africa. J Med Virol 55: 103-108.
[ Medline
]
- El-Zayadi AR, Abe K, Selim O,
Naito H, Hess G, Ahdy A 1999. Prevalence of GBV-C/hepatitis G virus viraemia
among blood donors, health care personnel, chronic non-B non-C hepatitis,
chronic hepatitis C and hemodialysis patients in Egypt. J Virol Meth
80: 53-58.
- Gallian P, Rodrigues V, Cantaloube
JF, Dessein H, Micco P, Dessein AJ, Lamballeri X 1998. High prevalence of
GB-C/hepatitis G virus in a Brazilian population with helminth infection.
J Med Virol 56: 310-315. [ Medline
]
- Goubau P, Andrade FB, Liu H, Basilio
FPS, Croonen L, Barreto-Gomes VAF 1999. Prevalence of GB virus C/hepatitis
G virus among blood donors in north-eastern Brazil. Trop Med Intern Health
4: 365-367.
- Gutierrez RA, Dawson GJ, Knigge
MF, Melvin SL, Heynen CA, Kyrk CR, Young CE, Carrick RJ, Schlauder GG, Surowy
TK, Dille BJ, Coleman PF, Thiele DL, Lentino JR, Pachucki C, Mushahwar IK
1997. Seroprevalence of GB virus C and persistence of RNA and antibody. J
Med Virol 53: 167-173. [ Medline
]
- Heuft HG, Berg T, Schreier E,
Künkel U, Tacke M, Schwella N, Hopf U, Salama A, Huhn D 1998. Epidemiological
and clinic aspects of hepatitis G virus infection in blood donors and immunocompromised
recipients of HGV-contaminated blood. Vox Sang 74: 161-167.
- Katayama K, Kageyama T, Hoshino
FB, Fukushi S, Kurihara C, Ishiyama N, Okamura H, Oya A 1998. Full-lengh GBV-C/HGV
genomes from nine Japanese isolates: characterization by comparative analyses.
Arch Virol 143: 1063-1075.
- Konomi N, Miyoshi C, Zerain CF,
Li T, Arakawa Y, Abe K 1999. Epidemiology of hepatitis B, C, E and G virus
infection and molecular analysis of hepatitis G isolates in Bolivia.J ClinMicrobiol
37: 3291-3295.
- Lampe E, Oliveira JM, Pereira
JL, Saback FL, Yoshida CFT, Niel C 1998a. Hepatitis G virus (GBV-C) infection
among Brazilian patients with chronic liver disease and blood donors. Clin
DiagVirol 9: 1-7.
- Lampe E, Saback FL, Viazov S,
Roggendorf M, Niel C 1998b. Age-specific prevalence and genetic diversity
of GBV-C/hepatitis G virus in Brazil. J Med Virol 56: 39-43.
[ Medline
]
- Lampe E, Saback FL, Yoshida CFT,
Niel C 1997. Infection with GB virus C/hepatitis G virus in Brazilian hemodialysis
and hepatitis patients and asymptomatic individuals. J Med Virol 52:
61-67. [ Medline
]
- Lefrère JJ, Férec
C, Roudot-Thoraval F, Loiseau P, Cantaloube JF, Biagini P, Mariotti M, LeGac
G, Mercier B 1999. GBV-C/hepatitis G virus (HGV) RNA load in immunodeficient
individuals and in immunocompetent individuals. J Med Virol 59: 32-37.
[ Medline
]
- Linnen J, Wages J, Zhang-Zeck
ZY, Fry KE, Krawczynski KZ, Alter H, Koonin E, Gallagher M, Alter M, Hadziyannis
S, Karayiannis P, Fung K, Nakatsuji Y, Shih JWK, Young L, Piatak Jr M, Hoover
C, Fernandez J, Chen S, Zou JC, Morris T, Hyams KC, Ismay S, Lifson JD, Hess
G, Foung SKH, Thomas H, Bradley D, Margolis H, Kim JP 1996. Molecular cloning
and disease association of hepatitis G virus: a transfusion transmissible
agent. Science 271: 505-508. [ Medline
]
- Mercier B, Barclais A, Botte C,
Cantaloube JF, Coste J, Defer C, Gautreau C, Giannoli C, Halfon P, Lepot I,
Loiseau P, Martial J, Montcharmont P, Merel P, Ouzan D, Ravera N, Follana
J, Césarie R, Janot C, Lemarie JM, De Micco JM, Venoz G, Férec
C 1999. Prevalence of GBV-C/HGV RNA and GBV-C/HGV antibodies in French volunteer
blood donors: results of a collaborative study. Vox Sang 76:166-169.
[ Medline
]
- Muerhoff AS, Leary TP, Simons
JN, Pilot-Matias TJ, Dawson GJ, Erker JC, Chalmers ML, Schlauder ML, Desai
SM, Mushahwar IK 1995. Genomic organization of GB viruses A and B: two new
members of the Flaviviridae associated with GB agent hepatitis. J
Virol 69: 5621-5630. [ Medline
]
- Muerhoff AS, Simons JN, Leary
TP, Erker JC, Chalmers ML, Pilot-Matias TJ, Dawson GJ, Desai SM, Mushahawar
IK 1996. Sequence heterogeneity within the 5'-terminal region of the hepatitis
GB virus C genome and evidence for genotypes. J Hepatol 25: 379-384.
[ Medline
]
- Muerhoff AS, Smith DB, Leary TP,
Erker JC, Desai SM, Mushahwar IK 1997. Identification of GB virus C variants
by phylogenetic analysis of 5'-untranslated and coding region sequences. J
Virol 71: 6501-6508. [ Medline
]
- Mukaide M, Mizokami M, Orito E,
Ohba K, Nakano T, Ueda R, Hikiji K, Iino S, Shapiro S, Lahat N, Park YM, Kim
BS, Oyunsuren T, Rezieg M, Al-Ahdal MN, Lau JYN 1997. Three different GB virus
C/hepatitis G virus genotypes. Phylogenetic analysis and a genotyping assay
based on restriction fragment length polymorphism. FEBS Lett 407:
51-58. [ Medline
]
- Naito H, Hayashi S, Abe K 2000.
The entire nucleotide sequence of two hepatitis G virus isoltes belonging
to a novel genotype: isolation in Myanmar and Vietnam. J Gen Virol
81: 189-194.
- Nübling CM, Bialleck H, Fürsch
AJ, Scharrer I, Schramm W, Seifried E, Schmidt U, Staszewski S, Lower J 1997.
Frequencies of GB virus C/ hepatitis G virus genomes and of specific antibodies
in German risk and non-risk populations. J Med Virol53: 218-224.
- Okamoto H, Nakano H, Inoue T,
Fukuda M, Kishimoto J, Ilizuda H, Tsuda F, Miyakawa Y, Mishiro M 1997. The
entire nucleotide sequence of two GB virus C/hepatitis G virus isolates of
distinct genotypes from Japan. J Gen Virol 78: 737-745.
- Orito E, Mizokami M, Nakano T,
Wu R, Cao K, Ohba K, Ueda R, Mukaide M, Hikiji K, Matsumoto Y, Iino S 1996.
GB virus C/hepatitis G virus infection among Japanese patients with chronic
liver diseases and blood donors. Virus Res 46: 89-93. [ Medline
]
- Oubiña JR, Mathet V, Feld
M, Della Lata MP, Ferrario D, Verdun R, Libonatti O, Fernández J, Carballal
G, Sánchez DO, Quarleri JF 1999. Genetic diversity of GBV-C/HGV strains
among HIV infected-IVDU and blood donors from Buenos Aires, Argentina. Virus
Res 65: 121-129. [ Medline
]
- Pinho JRR, Zanotto PMA, Ferreira
JLP, Sumita LM, Carrilho FJ, Silva LC, Capacci ML, Silva AO, Guz B, Gonçales
Jr FL, Gonçales NSL, Buck GA, Meyers GA, Bernardini AP 1999. High prevalence
of GB virus C in Brazil and molecular evidence for intrafamiliar transmission.
J Clin Microbiol 37: 1634-1637. [ Medline
]
- Quarleri JF, Mathet VL, Feld M,
Ferrario D, Della Lata MP, Verdun R, Sánchez DO, Oubinã JR 1999.
GB virus C/hepatitis G virus groups and subgroups: classification by a restriction
fragment length polymorphism method based on phylogenetic analysis of the
5' untranslated region. J Clin Microbiol 37: 1340-1347. [ Medline
]
- Roth WK, Waschk D, Marx S, Tschauder
S, Zeuzem S, Bialleck H, Weber H, Seifried E 1997. Prevalence of hepatitis
G virus and its strain variant, the GB agent, in blood donations and their
transmission to recipients. Transfusion 37: 651-655. [ Medline
]
- Sathar MA, Soni PN, Naicker S,
Conradie J, Lockhat F, Gouws E 1999. GB virus C/hepatitis G virus infection
in KwaZulu Natal, South Africa. J Med Virol 59: 38-44. [ Medline
]
- Sauleda S, Esteban JI, Hernandez
JM, Reesink H, Castella D, Quer J, Hess G, Esteban R, Guardia J 1999. Evaluation
of RNA and E2 antibodies in prospectively followed recipients of hepatitis
G virus-infected blood. Transfusion 39: 633-688. [ Medline
]
- Schmidt M, Korn K, Fleckenstein
B 1996. Molecular evidence for transmission of hepatitis G virus by blood
transfusion. Lancet 347: 909.
- Simons JN, Leary TP, Dawson GJ,
Pilot-Matias TJ, Muerhoff AS, Schlauder GG, Desai SM, Mushahwar IK 1995. Isolation
of a novel virus-like sequence associated with human hepatitis. Nature
Med 1: 564-569.
- Stark K, Doering CD, Bienzele
U, Pauli G, Hamouda O, Engel AM, Schreier E 1999. Risk and clearence of GB
virus C/hepatitis G virus infection in homosexual men: a longitudinal study.
J Med Virol 59: 303-306.
- Tanaka Y, Mizokami M, Orito E,
Ohba K, Nakano T, Kato T, Kondo Y, Ding X, Ueda R, Sonoda S, Tajima K, Miura
T, Hayami M 1998. GB virus C/hepatitis G virus infection among Colombian native
Indians. Am J Trop Med Hyg 59: 462-467. [ Medline
]
- Tillmann HL, Heiken H, Botor-Knapik
A, Heringlake S, Ockenga J, Wilber JC, Goergen B, Detmer J, McMorrow M, Stoll
M, Schmidt RE, Manns MP 2001. Infection with GB virus C and reduced mortality
among HIV-infected patients. N Engl J Med 345: 715-724. [ Medline
]
- Tucker TJ, Smuts HE 2000. GBV-C/HGV
genotypes: proposed nomeclature for genotypes 1-5. J Med Virol 62:
82-83.
- Tucker TJ, Smuts HE, Eickhaus
P, Robson SC, Kirsch RE 1999. Molecular characterization of the 5' non-coding
region of South African GBV-C/HGV isolates: major deletion and evidence for
a fourth genotype. J Med Virol 59: 52-59. [ Medline
]
- Wejstål R, Månson
A, Widell A, Norkrans G 1999. Perinatal transmission of hepatitis G virus
(GB virus type C) and hepatitis C virus infections - a comparison. Clin
Infect Dis 28: 816-821. [ Medline
]
- Xiang J, Wunschmann S, Dikema
DJ, Klinzaman D, Patrick KD, George SL, Stapleton JT 2001. Effect of coinfection
with GB virus C on survival among patients with HIV infection. N Engl J
Med 345: 707-714. [ Medline
]
- Yeo AET, Matsumoto A, Hisada M,
Shih JM, Alter HJ, Goedert JJ 2000. Effect of hepatitis G virus infection
on progression of HIV infection in patients with hemophilia. Ann Intern
Med 132: 959-963. [ Medline
]
Copyright 2002 Instituto Oswaldo
Cruz - Fiocruz
The following images related to this document are available:
Photo images
[oc02217t1.jpg]
[oc02217f1.jpg]
[oc02217t2.jpg]
|

{kind=link}
{kind=link}
{kind=link}