
|
Memórias do Instituto Oswaldo Cruz
Fundação Oswaldo Cruz, Fiocruz
ISSN: 1678-8060 EISSN: 1678-8060
Vol. 97, Num. 7, 2002, pp. 965-970
|
Mem Inst Oswaldo Cruz, Rio de
Janeiro, Vol. 97(7), October
2002, pp. 965-970
Clinical and Epidemiological
Aspects of Human Parvovirus B19 Infection in an Urban Area in Brazil (Niterói
City Area, State of Rio de Janeiro, Brazil)
Solange Artimos de Oliveira/+,
Luiz Antonio Bastos Camacho*, Antonio Carlos de Medeiros Pereira, Tereza Filomena
Faillace**, Sérgio Setúbal, Jussara Pereira do Nascimento***
Disciplina de Doenças Infecciosas
e Parasitárias, Hospital Universitário Antonio Pedro, Rua Marques
do Paraná 303, 2o. andar, 24030-210 Niterói,
RJ, Brasil *Departamento de Epidemiologia, Escola Nacional de Saúde Pública-Fiocruz,
RJ, Brasil **Policlínica Comunitária Santa Rosa, Fundação
Municipal de Saúde de Niterói, Niterói, RJ, Brasil ***Instituto
Biomédico, Universidade Federal Fluminense, Niterói, RJ and Departamento
de Desenvolvimento Tecnológico, Biomanguinhos-Fiocruz, Rio de Janeiro,
RJ, Brasil
+Corresponding author. Fax: + 55-21-2719.7262.
E-mail: artimos@vm.uff.br
This work was supported
by Conselho Nacional de Pesquisa e Desenvolvimento (CNPq, grant No. 52-0689/96-8)
and Fundação de Amparo à Pesquisa do Rio de Janeiro (Faperj,
grant No. E-26-170-579-99).
Received 11 April 2002
Accepted 9 July 2002
Code Number: oc02219
This study was designed to analyse
the clinical and epidemiological data from human parvovirus B19 cases in a six-year
study of rash diseases conduct in an urban area in Brazil (Niterói city
area, State of Rio de Janeiro). A total of 673 patients with acute rash diseases
were seen at two primary health care units and at a general hospital. A clotted
blood sample was collected from all subjects at the time of consultation. Forty-nine
per cent (330 cases) of the patients were negative for dengue, rubella and measles
IgM or for low avidity IgG to HHV-6. Of these 330, 105 (31.8%) were identified
as IgM positive to parvovirus B19 by using an antibody capture EIA. During the
study period, three distinct peaks of parvovirus infection were detected, suggesting
that the disease appears to cycle in approximately 4-5 years. B19 infection
was characterized by variable combinations of fever, flu-like symptoms, arthropathy,
and gastrointestinal symptoms. Frequency of fever and arthropathy was substantially
higher in adults, 75% [c2 (1 D.F.) = 11.39,
p = 0.0007] and 62.5% [c2 (1 D.F.) = 29.89,
p = 0.0000], respectively. "Slapped-cheek" appearance and reticular
or lace-like rash were seen in only 30.1% of the children. No adult presented
this typical rash. The lack of the typical rash pattern in a large proportion
of parvovirus B19 and the similarity of clinical manifestations to other rash
diseases, specially to rubella, highlight the difficulty of diagnosing B19 infection
on clinical grounds alone.
Key words: human parvovirus B19 -
diagnosis - IgM - epidemiology - clinical features - Niterói, Rio de
Janeiro - Brazil
Human parvovirus B19, discovered
by Cossart et al.(1975) in 1974, commonly infects children, causing erythema
infectiosum, a mild rash illness characterized by a facial rash ("slapped-cheek")
and a lacy, reticular, evanescent macular eruption over the trunk and proximal
extremities (Anderson et al.1983). Adults, particularly females, with erythema
infectiosum, frequently present joint symptoms (Reid et al.1985). Parvovirus
B19 also causes transient aplastic crisis in patients with underlying hemolytic
anemia (Pattison et al. 1981), persistent anemia in immunocompromised patients
(Kurtzman et al. 1989) and hydrops fetalis and fetal loss during pregnancy (Brown
et al. 1984).
Although the association between
parvovirus B19 and erythema infectiosum has been established since 1983 (Anderson
et al.1983), reports on B19 infections have been scarce in Brazil. Notwithstanding,
prevalence studies conducted by Nascimento et al. (1990), Freitas et al. (1993,
1999) have shown that the infection is widespread in some states of the country.
The objective of the present study
is to analyze the clinical and epidemiological data from B19 cases in a six-year
study of rash diseases conducted in the municipality of Niterói, State
of Rio de Janeiro, Brazil. Analysis of the other rash diseases were presented
elsewhere (Oliveira et al. 2001b).
PATIENTS AND METHODS
Study population - Data collection
was conducted from January 1994 to December 1999. A total of 673 patients with
acute rash diseases were seen at the two largest primary health care units (Policlínica
Comunitária Santa Rosa and Centro de Saúde Carlos Antonio da Silva)
and at a general hospital (Hospital Universitário Antonio Pedro) from
the public network with a catchment comprising approximately 50% of the population
of the metropolitan area of Niterói. A questionnaire was used to collect
demographic, clinical and epidemiological data. Informed consent was obtained
for participants and from the parents or guardians of patients younger than
18 years of age. The study protocol was approved by the hospital's Institutional
Review Board.
Laboratory tests - A
clotted blood sample was collected from all subjects at the time of consultation.
A second sample was also obtained between 7 and 10 days later from 29 patients.
The samples were centrifuged and serum was separated and frozen at -20oC
until the serological analysis was performed. All serum samples were tested
for the presence of anti-rubella IgM virus antibodies by using a commercial
enzyme immunoassay (EIA) (Rubenostika IgM, Organon), for anti-measles virus
IgM by using an antibody capture EIA developed at the Centers for Disease Control
and Prevention (Atlanta, USA) (Hummel et al. 1992), and for anti-dengue virus
IgM by using an in-house EIA (Kuno et al. 1987, Nogueira et al. 1992). Those
specimens, negative for rubella, measles and dengue virus antibodies, were also
tested for anti-human parvovirus B19 IgM using an antibody capture EIA (MACEIA)
(Cubel et al. 1994, Nascimento et al. 1998). Primary infection with human herpesvirus
type 6 (HHV-6) was diagnosed by an indirect immunofluorescence test for low
avidity HHV-6 IgG (Ward et al. 1989).
Data (statistical) analysis -
Age and sex distribution, clinical features and time of occurrence of cases
of parvovirus B19 infection were analyzed and compared to those in other rash
diseases investigated during the study. The study population was divided in
age groups and patients with ³ 15 years of age
were considered as adults. The chi-squared test was used to compare proportions
and p < 0.05 was considered statistically significant. Data were analyzed
using Epi Info Version 6 (Dean et al. 1994).
RESULTS
Forty-nine per cent (330 cases) of
the patients were negative for dengue, rubella and measles IgM or for low avidity
IgG to HHV-6. Of these, 105 (31.8%) were identified as IgM positive to parvovirus
B19.
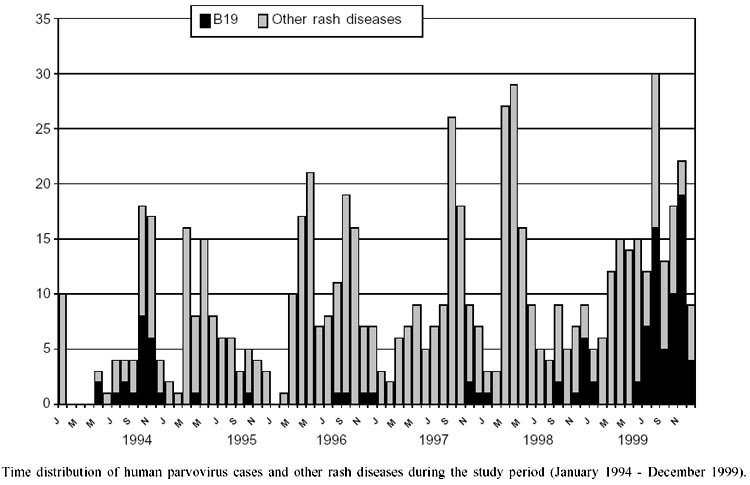
The distribution of the cases throughout
the years (Figure), showed peaks
of occurrence in which different rash diseases prevailed (Oliveira et al. 2001b).
Parvovirus B19 infection showed a clear seasonal variation, being most frequent
in late winter and spring (July-December): 92.4% of the cases were seen in the
second semester of the study years. During the study period, three distinct
peaks of parvovirus infection were detected, in the second part of 1994, 1998
and 1999. The 1999 peak of infection, was most prominent, comprising 60% (63/105)
of the study cases. The proportion of parvovirus B19 infections among rash diseases
varied from 23.1% to 58.7% in the second semester of the years of high incidence.
In nonepidemic years, the proportion varied from 3.9% to 5.9%.
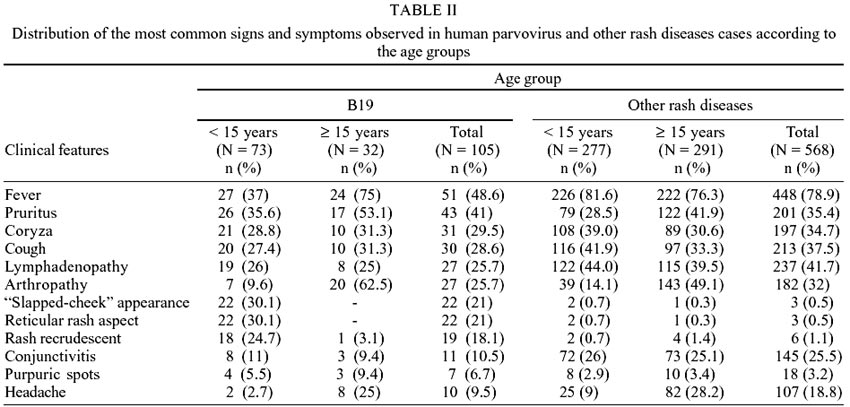
Most B19 cases (69.5%) occurred in
children, whereas the other rash diseases had a more balanced age distribution
(Table I). Male and female gender
were equally distributed among parvovirus B19 infections as well as among other
rash diseases, in the age group < 15 years old. However, in adult B19 cases
there was a clear predominance of females (26/32 - 81.3%), which was less pronounced
in other rash diseases (190/291 - 65.3%).
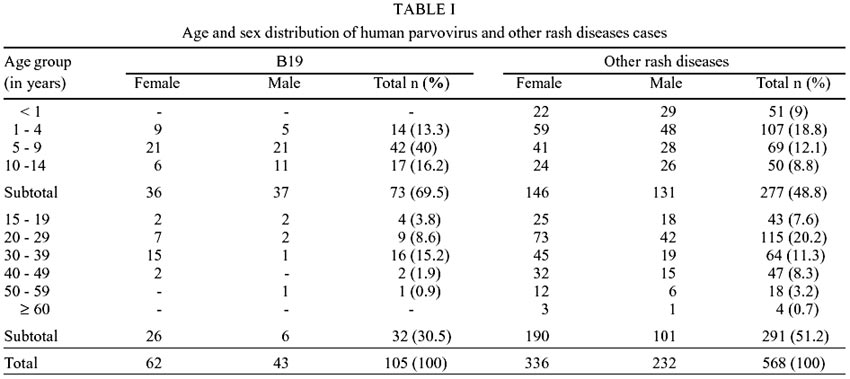
B19 infection was characterized by
variable combinations of fever, flu-like symptoms, arthropathy, and gastrointestinal
symptoms (Table II). Frequency of
fever and arthropathy was substantially higher in adults, 75% [c2
(1 D.F.) = 11.39, p = 0.0007] and 62.5% [c2
(1 D.F.) = 29.89, p = 0.0000], respectively. Although pruritic rash was reported
more frequently in adults (53.1%) than in the age group < 15 years old (35.6%),
this difference was not statistically significant [c2
(1 D.F.) = 2.14, p = 0.1432].
A large proportion of B19 cases presented
with an erythematous maculopapular rash, whereas purpuric spots occurred only
in seven (6.7%) cases. "Slapped-cheek" appearance and reticular or
lace-like rash were seen in only 30.1% of the children. No adult presented this
typical rash. Recrudescence of the rash (precipitated by exercise or heat) occurred
in 18.1% of the cases and the vast majority (94.7%) was noted in children. The
distribution and recrudescence of the rash showed the most striking contrasts
between B19 cases and other rash diseases. Differences in the frequency of other
symptoms were narrower and more difficult to interpret given the heterogeneity
of the group of rash diseases.
Arthropathy was reported more frequently
in adults with B19 infection than in adults with other rash diseases. In general,
it was symmetrical, affecting preferentially the small joints of the hands,
feet, knees and writs. Less frequently, ankles, elbows and cervical spine were
affected. The acute polyarthropathy completely resolved within two weeks, but
for one woman it lasted for three months.
Exposure to an exanthematic disease
was reported by 46 (43.8%) patients and the most frequently reported site of
transmission was home (71.7%). Acquisition of infection at school was reported
only in children, occurring in 7 (21.2%) of the 33 cases with available data.
Nine of the 13 women who had a known contact acquired the infection from their
children. B19 infection was serologically confirmed in 27 (58.7%) of the contacts
of the 46 patients that reported exposure to an exanthematic disease.
DISCUSSION
Although some studies (Freitas et
al. 1988, 1990, 1993, Miranda et al. 1989, Nascimento et al. 1990, Cubel et
al. 1992, Mielle et al. 1995) have been published in recent years, including
preliminary results of the first year of this study (Oliveira et al. 1996),
clinical and epidemiological aspects of parvovirus B19 are still not widely
documented in Brazil. By systematically gathering data on acute rash diseases
over the years we disclosed a seasonal pattern of the infection in a mid-sized
urban area. During the study period, three distinct peaks of parvovirus infection
were detected, suggesting that the disease appears to cycle in approximately
4-5 years. To our knowledge, this is the first time that the cyclical pattern
of parvovirus B19 infection has been described in our country. Our finding is
similar to those reported in the literature. Rates of infection increase every
3-4 years (Serjeant et al. 1993), although long-term cyclical variation, with
peak activity of infection occurring every 4-7 years, is also described (Rodis
1999).
Different from other rash diseases
for which specific control measures have been applied, parvovirus B19 incidence
fluctuates without interference. Outbreaks of parvovirus B19 infection in temperate
climates are more common in late winter and spring months, though cases may
be recorded in any month (Cohen 1995). In our study, 92.4% of the cases were
recorded during this season, similar to the report by Cubel et al. (1997) for
other regions of Brazil. However, different findings were reported in the Amazon
region by Miranda et al. (1989), who described higher incidence of the disease
during the first half of the year, a season of heavy rainfall and high humidity
in the North of our country.
The high proportion of schoolchildren
(56.2%) among cases of B19 infections with rash is consistent with that reported
in the literature (Brown 1997, Rodis 1999). Most of the B19 cases in adults
(81.3%) occurred in females and 9 of the 13 women who had a known contact acquired
the infection from their children. In a B19 outbreak, no significant differences
in attack rates in males and females were observed by Woolf et al. (1989), although
other authors have reported higher rates in females (Ager et al. 1966, Lauer
et al. 1976). In a controlled clinical-epidemiological study, Woolf et al. (1989)
found that women with B19 infection usually develop an acute arthropathy with
rash, often accompanied by flu-like symptoms, whereas men present fewer symptoms,
being a flu-like illness often the sole manifestation. Therefore, it is likely
that the clear predominance of adult women in our study could be related to
the exuberance of clinical manifestations of B19 infection in females and to
the study design, which did not allow us to detect subclinical infections caused
by the virus.
In general, clinical aspects presented
by our patients were in agreement with those reported by other authors. Frequently,
the disease was characterized by variable combinations of rash, flu-like symptoms
and arthropathy. As described in the literature (Reid et al. 1985), less than
10% of the children had arthralgias or joint swelling, these complaints being
substantially higher in adults (62.5%), particularly female adults. The arthropathy
was symmetrical, affecting more often small joints of hands, feet, knees, wrists.
Although usually brief and self-limiting, in 20% of affected women arthropathy
may persist or recur for more than two months (Woolf et al. 1989, Brown 1997).
In our study, prolonged joint complaints were seen only in 1 (3.8%) of the 26
adult females studied.
The classical slapped-cheek and lace-like
rash have been reported more frequently in children, although they have also
been described in adults (Woolf et al. 1989). In our study population, this
typical rash pattern was found only in children and, among them, in only 30.1%
of the cases. However, for all the other cases that formed our study group the
frequency of these rash patterns was very small. This was the only meaningful
contrast between B19 cases and the other rash diseases, which were rather heterogeneous.
Another finding of this study was the frequency of fever in adults (75%), significantly
greater than in children (37%). It is unclear to what extent this difference
was real or resulted from ascertainment.
The lack of the typical rash pattern
in a large proportion of parvovirus B19 and the similarity of clinical manifestations
to other rash diseases, specially to rubella, highlight the difficulty of diagnosing
B19 infection on clinical grounds alone. Moreover, parvovirus B19 infection
shares the seasonal pattern with rubella and measles, i.e., late winter and
spring, which makes clinical diagnosis even more difficult. In Brazil, because
of the reduction in measles and rubella incidence rates after the introduction
of national mass vaccination campaigns, parvovirus B19 infection has increased
its relative importance in the surveillance of rash diseases (Cubel et al. 1997,
Ministério da Saúde 1999, Oliveira et al. 2001a). However, without
the aid of laboratory methods, the public health relevance is likely to be unnoticed.
Symptomatic parvovirus B19 infections are likely to be misdiagnosed as one of
the more widely known rash diseases. Our data indicate that the diagnosis of
B19 infection should be considered more often, particularly in pregnant women,
immunocompro-mised patients and individuals with underlying hemolytic disorders,
as the infection may lead to serious adverse outcomes.
The findings from this study have
relevant implications for the epidemiological surveillance of rash diseases.
The outbreak of parvovirus B19 in 1999 was missed by routine surveillance, which
was conceived mainly for measles control. As measles and rubella cases become
rarer, the relative importance of parvovirus B19 and other exanthematic diseases
will grow and may eventually have to be targeted by epidemiological surveillance.
Caution should be exercised in the
interpretation of findings from an uncontrolled study of a non-probabilistic
sample of cases gathered from health care settings and, thus, lacking statistical
representativeness. Selective forces acting upon individuals, who ended up in
this case series are only partly known. Our study group provided clinical and
demographic descriptive data on the subset of parvovirus B19 infections, who
presented a maculopapular cutaneous rash, and felt (or was thought to be) ill
enough to seek medical care, and managed to get it in the public health care
network. They are likely to represent the most severe cases in the clinical
spectrum of the disease. Therefore, the age, sex distribution and the frequency
of symptoms may not apply to all those infected. Still, the distribution of
cases over time, may be considered a rough representation of the occurrence
of the infection in that population, which was substantially covered by the
health care units where study participants were recruited.
ACKNOWLEDGEMENTS
To Dr Marilda M Siqueira and Dr Rita
M Nogueira from Fundação Oswaldo Cruz, Rio de Janeiro, Brazil
for, respectively, measles/rubella tests and dengue test; to the general practitioners
from the Department of Infectious Diseases/Hospital Universitário Antonio
Pedro, the Policlínica Comunitária Santa Rosa and from the Centro
de Saúde Carlos Antonio da Silva, Niterói, Rio de Janeiro, Brazil,
for clinical support. To Dr Bernard J Cohen from the Enteric, Respiratory and
Neurological Virus Laboratory, Central Public Health Laboratory, London, UK,
for revising the manuscript critically.
REFERENCES
- Ager EA, Chin TDY, Poland JD 1996.
Epidemic erythema infectiosum. N Engl J Med 275: 1326-1331.
- Anderson MJ, Jones SE, Fisher-Hoch
SO, Lewis E, Hall SM, Bartlett CR, Cohen BJ, Mortimer PP, Pereira MS 1983.
Human parvovirus, the cause of erythema infectiosum (fifth disease)? Lancet
1: 1378.
- Brown KE 1997. Human parvovirus
B19 epidemiology and clinical manifestations. In LJ Anderson, NS Young (eds),
Human Parvovirus B19, Monographs in Virology, Basel Karget, vol. 20,
p. 42-60.
- Brown T, Anand A, Ritchie LD,
Clewley JP, Reid TMS 1984. Intrauterine parvovirus infection associated with
hydrops fetalis. Lancet ii: 1033-1034.
- Cohen BJ 1995. Parvovirus B19:
an expanding spectrum of disease. BMJ 311: 1549-1552.
[ Medline
]
- Cossart YEA, Field AM, Cabt B,
Widdows D 1975. Parvovirus-like particles in human sera. Lancet i:
72-73.
- Cubel RCN, Alferes ACR, Cohen
BJ, Nascimento JP 1994. Application to immunoglobulin M capture hemadherence
assays of hemagglutination of monkey erythrocytes by native and recombinant
human parvovirus B19 antigens. J Clin Microbiol 32: 1997-1999.
[ Medline
]
- Cubel RCN, Siqueira MM, Santos
EO, Pires MF, Cruz CMF, Nascimento JP 1997. Human parvovirus B19 infections
among exanthematic diseases notified as measles. Rev Soc Bras Med Trop
30: 15-20. [ Lilacs
] [ SciELO
]
- Cubel RCN, Valadão MC,
Pereira WV, Magalhães MC, Nascimento JP 1992. Aplastic crisis due to
human parvovirus B19 infection in hereditary hemolytic anaemia. Rev Inst
Med Trop São Paulo 34: 479-482. [ Medline
] [ Lilacs
]
- Dean AG, Dean JA, Coulombier D,
Brendel KA, Smith DC, Burton AH, Dicker RC, Sullivan K, Fagan RF, Arner TG
1994. Epi Info Version 6, Centers for Diseases Control and Prevention,
Atlanta, GA.
- Freitas RB, Gusmão SRB,
Durigon EL, Linhares AC 1999. Survey of parvovirus B19 infection in a cohort
of pregnant women in Belém, Brazil. Braz J Infect Dis 3:
6-14. [ Lilacs
]
- Freitas RB, Linhares AC, Miranda
MFR, Gabbay IV 1988. Novo agente de doença exantemática na Amazônia:
o parvovirus "B19". Bol Epidemiol (Brazil, Ministério
da Saúde, Fundação Sesp) 20: 1-4.
- Freitas RB, Miranda MFR, Shirley
J, Tudor R, Desselberger U, Linhares AC 1993. Parvovirus B19 antibodies in
sera of patients with unexplained exanthemata from Belém, Pará,
Brazil. Mem Inst Oswaldo Cruz 88: 497-499. [ Medline
] [ Lilacs
]
- Freitas RB, Wong D, Boswell F,
Miranda MF, Linhares AC, Shirley J, Desselberger 1990. Prevalence of human
parvovirus B19 and rubellavirus infections in urban and remote rural areas
in Northern Brazil. J Med Virol 32: 203-208.
- Hummel KB, Erdman DD, Heath J,
Bellini WJ 1992. Baculo-virus expression of the nucreoprotein gene of measles
virus and utility of the recombinant protein in diagnosis enzyme immunoassays.
J Clin Microbiol 30: 2874-2880.
- Kuno G, Gomez I, Gubler DJ 1987.
Detecting artificial anti-dengue IgM immune complexes using an enzyme linked
immunosorbent assay. Am J Trop Med Hyg36: 153-159.
- Kurtzman GJ, Cohen BJ, Field AM,
Oseas R, Blaese RM, Young NS 1989. Immune response to B19 parvovirus and an
antibody defect in persistent viral infection. J Clin Invest 84:
1114-1123. [ Medline
]
- Lauer BA, Maccormack JN, Wilfert
C 1976. Erythema infectiosum: an elementary school outbreak. Am J Dis Child
130: 252-254. [ Medline
]
- Mielle A, Nogueira MB, Lisboa
C, Yamashita CA, Costa SD, Lotufo JPB, Vieira SE, Durigon E, Stewvien K, Ejzenberg
B, Baldacci ER, Okay Y 1995. Infecção por parvovírus:
apresentação atípica em três crianças. Pediatria
(São Paulo) 17: 197-201.
- Ministério da Saúde,
Brasil 1999. Fundação Nacional de Saúde. Plano de Erradicação
do Sarampo e Controle da Rubéola e Síndrome da Rubéola
Congênita, Brasília.
- Miranda MFR, Linhares AC, Shirley
JA 1989. Fifth disease in children living in Belém, Brazil. Rev
Inst Med Trop São Paulo 31: 359-362. [ Medline
] [ Lilacs
]
- Nascimento JP, Buckley MM, Brown
KE, Cohen BJ 1990. The prevalence of antibody to human parvovirus B19 in Rio
de Janeiro, Brazil. Rev Inst Med Trop São Paulo 32: 41-45.
[ Medline
] [ Lilacs
]
- Nascimento JP, Mistchenko A, Cohen
BJ 1998. Laboratory diagnosis of acute human parvovirus infection by specific
IgM detection. Rev Inst Med Trop São Paulo 40: 265-266.
[ Medline
] [ Lilacs
] [ SciELO
]
- Nogueira RMR, Miagostovich MP,
Cavalcanti SMB, Marzo-chi KBF, Schatzmayr HG 1992. Levels of IgM antibodies
against dengue virus in Rio de Janeiro, Brazil. Res Virol 143:
423-427. [ Medline
]
- Oliveira SA, Brandão AB,
Fernandes DG, Bettini LR, Carvalho AB, Pereira ACM, Azevedo KM, Nascimento
JP 1996. Human parvovirus B19 infection: clinical and epidemiological study
of 24 cases. Rev Inst Med Trop São Paulo 38: 323-327.
[ Medline
] [ Lilacs
]
- Oliveira SA, Pereira ACM, Rocha
ALC, Pereira SB, Faillace TF, Nascimento JP 2001a. Papel da parvovirose humana
na vigilância epidemiológica da rubéola e outras viroses
exantemáticas. Rev Soc Bras Med Trop 34 (Sup1. 1): 440-441.
- Oliveira SA, Siqueira MM, Camacho
LAB, Nogueira RM, Spinetti CCJ, Cubel-Garcia RCN, Knowles W, Brown DWG 2001b.
The aetiology of maculopapular rash diseases in Niterói, State of Rio
de Janeiro, Brazil: implications for measles surveillance. Epidemiol Infect
127: 509-516. [ Medline
]
- Pattison JR, Jones SE, Hodgson
J, Davis LR, White JM, Stroud CE, Murtaza L 1981. Parvovirus infections and
hypoplastic crisis in sickle-cell anaemia. Lancet i: 664-665.
- Reid DM, Reid TMS, Brown T, Rennie
JAN, Eastmond CJ 1985. Human parvovirus-associated arthritis: a clinical and
laboratory description. Lancet i: 422-425.
- Rodis JF 1999. Parvovirus infection.
Clin Obstet Gynecol 42: 107-120. [ Medline
]
- Serjeant GR, Serjeant BE, Thomas
PE, Anderson MJ, Patou G, Pattison JR 1993. Human parvovirus infection in
homozygous sickle cell disease. Lancet 341: 1237-1240.
- Ward KN, Gray JJ, Efstathiou S
1989. Brief report: primary human herpesvirus-6 infection in a patient following
liver transplantation from a seropositive donor. J Med Virol 28:
69-72. [ Medline
]
- Woolf AD, Campion GV, Chishick
A, Wise S, Cohen BJ, Klouda PT, Caul O, Dieppe PA 1989. Clinical manifestations
of human parvovirus B19 in adults. Arch Intern Med 149: 1153-1156.
[ Medline
]
Copyright 2002 Instituto Oswaldo
Cruz - Fiocruz
The following images related to this document are available:
Photo images
[oc02219t2.jpg]
[oc02219f1.jpg]
[oc02219t1.jpg]
|

{kind=link}
{kind=link}
{kind=link}