 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Mem Inst Oswaldo Cruz, Rio de Janeiro, Vol. 97(8), December 2002, pp. 1165-1168 Detection of Giardia duodenalis Antigen in Human Fecal Eluates by Enzyme-linked Immunosorbent Assay Using Polyclonal Antibodies Sofía Duque-Beltrán*, Rubén Santiago Nicholls-Orejuela/*/+, Adriana Arévalo-Jamaica, Rafael Guerrero-Lozano**/***, Sonia Montenegro****/*****, Mark A James*****
Laboratorio de Parasitología,
Instituto Nacional de Salud, Avenida Calle 26 No.51-60 CAN, Bogotá, D.C.,
Colombia *Facultad de Medicina, Universidad Nacional de Colombia, Bogotá,
D.C., Colombia **Gastroenterología Pediátrica, Universidad El
Bosque, Bogotá, D.C., Colombia ***Hospital Infantil Universitario "Lorencita
Villegas de Santos", Servicio de Gastroenterología, Bogotá,
D.C., Colombia ****Ochsner Medical Foundation, New Orleans, LA, USA *****Department
of Tropical Medicine, Tulane University Health Sciences Center, New Orleans,
LA, USA Received 1 April 2002 Code Number: oc02253
The present study developed and standardized an enzime-linked immunosorbent assay (ELISA) to detect Giardia antigen in feces using rabbit polyclonal antibodies. Giardia cysts were purified from human fecal samples by sucrose and percoll gradients. Gerbils (Meriones unguiculatus) were infected to obtain trophozoites. Rabbits were inoculated with either cyst or trophozoite antigens of 14 Colombian Giardia isolates to develop antibodies against the respective stages. The IgG anti-Giardia were purified by sequential caprylic acid and ammonium sulfate precipitation. A portion of these polyclonal antibodies was linked to alkaline phosphatase (conjugate). One hundred and ninety six samples of human feces, from different patients, were tested by parasitologic diagnosis: 69 were positive for Giardia cysts, 56 had no Giardia parasites, and 71 revealed parasites other than Giardia. The optimal concentration of polyclonal antibodies for antigen capture was 40 µg/ml and the optimal conjugate dilution was 1:100. The absorbance cut-off value was 0.24. The parameters of the ELISA test for Giardia antigen detection were: sensitivity, 100% (95% CI: 93.4-100%); specificity, 95% (95% CI: 88.6-97.6%); positive predictive value, 91% (95% CI: 81.4-95.9%); and negative predictive value, 100% (95% CI: 96.1-100%). This ELISA will improve the diagnosis of Giardia infections in Colombia and will be useful in following patients after treatment.
Key words: Giardia - antigen - enzyme-linked immunosorbent assay (ELISA) - feces - Colombia Giardia duodenalis has a worldwide distribution and the prevalence of infection varies widely depending on the sensitivity of the diagnostic method (Flanagan 1992), the geographical area (Flanagan 1992), and the population studied (Miotti et al. 1986). In Colombia, the prevalence of giardiasis, according to two national studies on intestinal parasitism, was reported to be 11.9% in 1969 (Galán et al. 1969) and 13.8% in 1980 (Corredor et al. 2000). More recently, the prevalence has increased to 28% in children aged 1 to 4 years (Botero & Restrepo 1998) and to 21.2% in a nationwide study carried out in 1996 on children aged 12 to 59 months (Castro de Navarro & Nicholls 1998). Diagnosis of Giardia infections has traditionally been carried out using microscopic identification of cysts or trophozoites in either single or multiple fecal specimens, duodenal aspirates, duodenal smears or small intestine biopsies (Wolfe et al. 1990). The sensitivity of parasite identification has been reported to increase up to 85% when multiple fecal samples obtained on three different days were examined (Goka et al. 1990). As opposed to duodenal aspirates and biopsy samples, which require invasive and rather costly procedures, fecal samples can be readily obtained, thus being the best sample available for parasite identification. However, for biological reasons such as the intermittent pattern of cyst or trophozoite excretion, sensitivities greater than 90% are rarely obtained. This problem can potentially be overcome if Giardia antigen detection assays are developed. Previous immunoassays for detection of Giardia antigen in fecal sample eluates have included counterimmunoelectrophoresis (CIE) (Craft & Nelson 1982), enzyme-linked immunosor-bent assay (ELISA) (Ungar et al. 1984, Green et al. 1985, Nash et al. 1987, Knisley et al. 1989, Dutt et al. 1991, McLaughlin et al. 1993, Torres et al. 1997, Fedorko et al. 2000) and dot-ELISA (Vinayak et al. 1991). The sensitivity of these methods has varied from 88 to 98% with CIE, and from 68 to 100% for the ELISA; their specificity has ranged from 90 to 97% for CIE, 81-100% for ELISA, and 100% for dot-ELISA. Several Giardia antigen detection kits are now commercially available (Rosoff et al. 1989, Addiss et al. 1991, García & Shimizu 1997, Aldeen et al. 1998, Rocha et al. 1999, Fedorko et al. 2000), their sensitivity varying from 85 to 98% and their specificity ranging between 90 and 100%. However, it is well known that the sensitivity and specificity of diagnostic methods based upon Giardia antigen detection can be affected by the genetic variability of Giardia isolates present in a given geographic area (Faubert & Belosevic 1990). The purpose of the present study was to develop and evaluate an enzyme immunoassay for Giardia antigen detection in eluates of human fecal samples, using specific polyclonal antibodies raised against endemic parasite isolates of Colombia. MATERIALS AND METHODS
Parasitological diagnosis - Fecal specimens, collected from 196 different patients, were submitted to direct wet mount and formol-ether concentration methods in order to identify Giardia trophozoites or cysts (Truant et al. 1981).
Production of polyclonal anti-Giardia cyst and trophozoite antibodies Preparation of Giardia cyst and/or trophozoite inocula - Giardia cysts were purified from human fecal samples. Trophozoites were obtained from experimentally infected gerbils with 14 different Giardia human isolates following the procedure described by Belosevic et al. (1983). Their concentration was independently adjusted to 1x106 per 1 ml saline (Green et al. 1985). Freeze (-196oC) and thaw (4°C) cycles were carried out. These solutions were submitted to ultrasound sonication (Harlow & Lane 1988). Immunization scheme - Rabbits were used to produce polyclonal antibodies against Giardia parasites. All procedures were carried out according to international guidelines (CIOMS 1985). Rabbits were inoculated via intradermal injection with Giardia cyst and trophozoite antigen, independently (Harlow & Lane 1988) on days 1, 15, 30, 60 and 120. Rabbits which were inoculated intradermally with cyst antigen were also immunized intravenously on day 30 (Harlow & Lane 1988). Purification of polyclonal anti-Giardia cyst and trophozoite antibodies - Rabbit polyclonal anti-Giardia cyst and trophozoite antibodies were purified from hyperimmune rabbit sera by sequential caprylic acid and ammonium sulfate precipitation (Arévalo 1999).
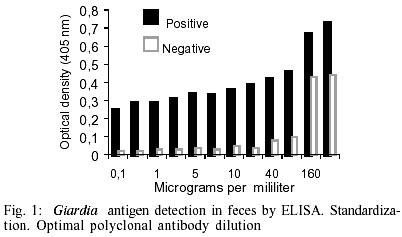
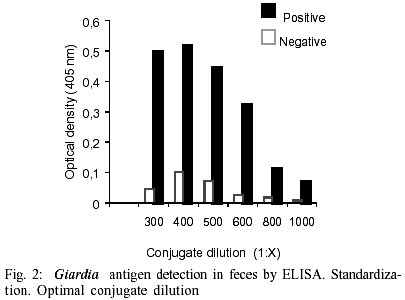
Detection of Giardia antigen in human fecal samples using an antigen-capture ELISA Test standardization - Purified rabbit polyclonal anti-Giardia antibodies were mixed in a 1:2 proportion of anti-cyst to anti-trophozoite antibodies, and the mixture then diluted in 0.05 M carbonate-bicarbonate coating buffer, pH 9.6, to final concentrations of 0.1, 0.5, 1, 2.5, 5, 10, 20, 40, 80, 160 and 320 µg/ml. Coproantigen samples were prepared by dissolving 1 g of each sample in 10 ml of PBS, pH 7.4 (Green et al. 1985). A positive human coproantigen fecal sample (eluate of a fecal sample which was diagnosed as positive for Giardia upon microscopical examination) and a negative coproantigen sample (sample negative for Giardia upon microscopical examination) were selected. An enzyme-linked anti-Giardia conjugate was diluted to 1:300, 1:400, 1:500, 1:600, 1:800 and 1:1000 in PBS containing 0.05% Tween 20 (PBS-T). The conjugate had been prepared previously with anti-cyst and anti-trophozoite antibodies, each adjusted to 2.4 mg/ml and mixed in a 1:2 proportion, respectively. Four milligrams of alkaline phosphatase were added in the presence of 1% glutaraldehyde (EM grade) and 1 M glycine. The enzyme conjugate was stored at -20oC until used (Arévalo 1999). Finally, capture and detecting antibody concentrations were titrated in a checkerboard format using an ELISA procedure described by McLaren et al. (1981). The optimal concentration of polyclonal anti-Giardia antibody necessary to capture Giardia antigen contained in human fecal eluates, defined as the minimum concentration which distinguished between positive and negative reference samples, was 40 µg/ml (Fig. 1) and the optimal dilution of the anti-Giardia enzyme conjugate, defined as that which allowed the best differentiation between positive and negative samples, was 1:400 (Fig. 2). The following procedural steps were considered optimal upon test standardization: Dynatech Immulon I® micro-ELISA polystyrene plates were coated with polyclonal anti-Giardia antibody (100 µl/well) diluted to a concentration of 40 µg/ml in 0.05 M carbonate-bicarbonate buffer, pH 9.6. The plates were incubated in a humidified chamber at room temperature (18ºC) for 3 h. After incubation, plates were then washed three times with PBS-T, 5 min each. Fecal eluates were each added in triplicate, 100 µl per well: eluates were diluted to a final concentration of 1:10 in gelatin which had been previously dissolved in a 1:1 proportion with PBS-T. The fecal antigen samples were allowed to incubate for 2 h as described above. The plates were then washed for three times with PBS-T, 5 min each. The alkaline phosphatase-linked anti-Giardia antibody conjugate was diluted in PBS-T at a final concentration of 1:400, and 100 µl placed in each well. The plates were allowed to incubate in a humidified chamber at 4°C overnight. After incubation, all plates were washed as above in PBS-T. The reactions were developed by adding 100 µl p-nitrophenyl phosphate (1 mg/ml) in 0.1 M diethano-lamine buffer, pH 9.8, to each well. After 30 min, color development was stopped by adding a 25 µl volume of 3N NaOH to each well. The absorbance value was determined by reading the optical density at a 405 nm wavelength using a MultiSkan MS® colorimeter.
Evaluation of the ELISA test for antigen detection Validation: statistical analysis - Validation of the ELISA for Giardia antigen detection was carried out by establishing the cut-off value (Kurstak 1985) and the test parameters (Griner et al. 1981). The cut-off value, defined as the absorbance value from which a negative sample can be clearly distinguished from a positive sample, was determined by adding twice the standard deviation to the mean absorbance value of the negative samples. This provides 95% reliability (Kurstak 1985). Sensitivity, specificity, positive and negative predictive values (PPV and NPV, respectively) and their 95% confidence intervals (95% CI) were determined using a 2 x 2 contingency table (Griner et al. 1981). RESULTS
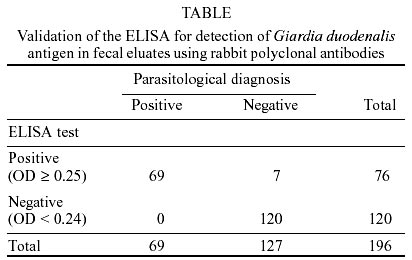
The results of the parasitological examination were: 69 samples were positive for Giardia cysts or trophozoites and 127 were negative. In 71 samples parasites other than Giardia were found upon microscopic examination. The ELISA test showed 76 samples positive for Giardia antigen and 120 negative (Table). The cut-off value for positive reactions was established at 0.240, and the parameters of the ELISA for Giardia antigen detection were: sensitivity, 100% (95% CI: 93.4-100%); specificity, 95% (95% CI: 88.6-97.6%); positive predictive value, 91% (95% CI: 81.4-95.9%); and negative predictive value, 100% (95% CI: 96.1-100%) (Table). The production of anti-cyst and anti trophozoite anti-Giardia polyclonal antibodies in independent fashion increased the reactivity of antibodies after each successive immunization as evidenced by an increasing intensity of the antigen-antibody precipitin bands as immunizations progressed. DISCUSSION
The immunodiagnostic test developed and described herein for detection of Colombian Giardia isolates antigen in fecal eluates shows differences with similar assays developed previously. Enzyme immunoassays use either the direct (Green et al. 1985, Knisley et al. 1989, Dutt et al. 1991, Torres et al. 1997) or indirect methods. The test described herein is based on the direct method with the advantage of using polyclonal anti-Giardia antibodies as capture reagent, and the same antibodies linked to an enzyme as conjugate for detecting the reaction. These features allow greater specificity in the antigen-antibody reaction and also simplify the test procedure. It is possible that optimization of the assay changes with each lot of antibody production. However, the standard conditions for the ELISA test can be maintained by titrating each new polyclonal antibody lot, which can be achieved by determining the optimal antibody concentration which allows the correct discrimination between a positive and a negative sample. The ELISA for Giardia antigen detection is easy to perform, inexpensive, and allows simultaneous processing of multiple samples. The cost of giardiasis parasitological diagnosis by means of examination of multiple fecal samples is similar to that of the ELISA antigen detection assay. However, the ELISA assay developed in the current study will improve the diagnosis of Giardia infections because the sensitivity increases from 85% to 100%. In addition, it should improve Giardia diagnosis by eliminating false negative results caused by lack of training and experience of the laboratory personnel responsible for microscopic examination, untimely processing of samples, and intermittent excretion of Giardia cysts and trophozoites in feces. This is the first Giardia antigen ELISA test developed in Colombia using polyclonal antibodies raised against endemic, homologous isolates of G. duodenalis, isolated from Colombian patients with parasitologically confirmed giardiasis. G. duodenalis isolates from other geographic regions do not necessarily share the same antigenic determinants. Because of antigenic variations or polymorphisms, antibodies raised against a particular isolate of Giardia may not necessarily cross-react with antigens of heterologous Giardia isolates from different geographic origin (Nash 1992). The analytical sensitivity of the assay was not established; however, a previous study showed little correlation between the numbers of cysts or trophozoites observed in fecal samples and the optical density values obtained by the ELISA test for detecting Giardia antigens in fecal eluates, possibly because the assay detects free antigen in feces rather than whole organisms (Green et al. 1985). The ELISA for antigen detection in human fecal eluates will improve diagnosis of Giardia infection. When applied under field conditions the test will be useful in determining the prevalence of Giardia infection and in making a timely diagnosis of infected individuals, particularly children who suffer from recurrent diarrhea, chronic abdominal pain, malabsorption and stunting as a consequence of infection. Currently, studies concerning the relationship between ELISA results, severity of disease and gastrointestinal symptoms as well as the application of the test in clinical follow-up, are being planned. Future studies should target the extent and degree of heterologous cross-reactivity of the polyclonal antibodies used in the test with Giardia isolates from different geographical origins, because of the antigenic variability which might exist among them.
ACKNOWLEDGEMENTS
To Instituto Nacional de Salud, Universidad El Bosque, Hospital Infantil Universitario "Lorencita Villegas de Santos", Ochsner Medical Foundation and Tulane University Health Sciences Center. REFERENCES
Copyright 2002 Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc02253f1.jpg] [oc02253f2.jpg] [oc02253t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}