 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Mem Inst Oswaldo Cruz, Rio de Janeiro, Vol. 98, No. 2, March, 2003, pp. 209-212 SHORT COMMUNICATION
Anti-human Immunodeficiency Virus-1 Antibody Titers in Injection Drug Users Compared to Sexually Infected Individuals Vera Bongertz/+/++, Elaine Priscilla Ouverney, Sylvia LM Teixeira, Carlos Silva-de-Jesus, Mariana A Hacker*, Mariza G Morgado/++, Francisco I Bastos*, The Brazilian Network for HIV Isolation and Characterization++
Laboratório de Aids e
Imunologia Molecular, Departamento de Imunologia, Instituto Oswaldo Cruz-Fiocruz
*Centro de Informações em Ciência e Tecnologia-Fiocruz, Av.
Brasil 4365, 21045-900 Rio de Janeiro, RJ, Brasil Received
5 June 2002 Code Number: oc03056
Sera from infected injection drug users (IDU) have shown to have antibodies against synthetic human immunodeficiency virus-1 (HIV-1) envelope peptides more frequently. In this study, reactivity of 48 IDU plasma were compared to 60 plasmas obtained from sexually infected individuals (S). The overall reactivity of plasma from IDU compared to S was higher, and the reactivity titers were much higher for IDU plasma than S. IDU plasma also showed a broader antibody response. The higher reactivity titers were observed mainly for the gp41 immunodominant epitope and V3 peptides corresponding to the consensus sequences of HIV-1 subtypes/variants prevalent in Brazil (B, F, C) indicating the specificity in the higher immune response of IDU.
Key words: human immunodeficiency virus-1 - antibodies - injection drug users
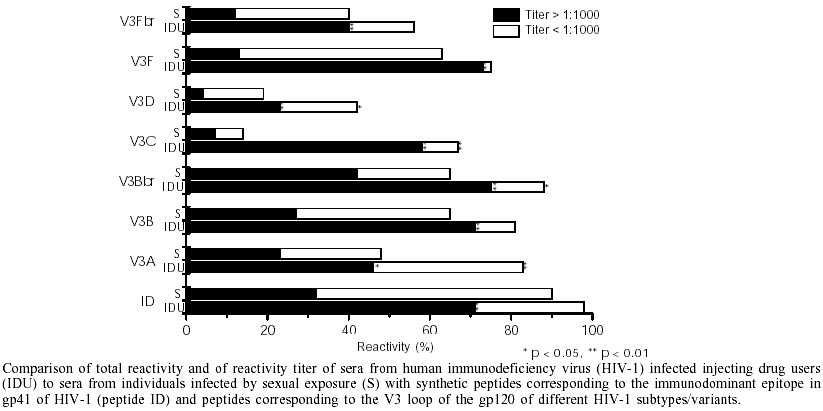
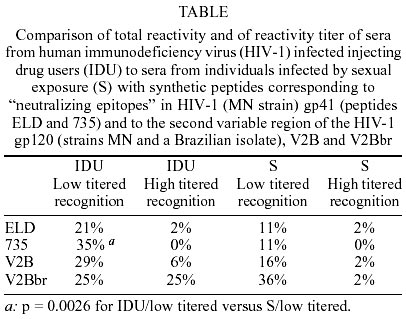
There are indications that injection drug users (IDU) progress slower towards disease after human immunodeficiency virus (HIV) infection than individuals infected by sexual HIV-1 transmission. At least compared to HIV infected homosexual men, IDU present a slower disease progression, independent of age, sex, time of serocon-version or even antiretroviral therapy (Pehrson et al. 1997).The high number of deaths resulting from non-AIDS-related causes, such as overdose/suicide before progression to AIDS (Selwyn et al. 1989, van Haastrecht et al. 1996, Hendricks et al. 1998), may be the cause for this higher mortality of HIV-infected IDUs without AIDS (Prins et al. 1997, Hendricks et al. 1998). It has been speculated that a continuously activated immune response in IDU as opposed to sexually infected individuals may induce a faster immune response (Wetli et al. 1974, Pehrson et al. 1997). Also, "selection" of HIV-1 which can occur in sexually(s) or vertically infected individuals may be different in parenteral HIV-1 infection, where selection will be restricted to the susceptibility of blood mononuclear cells to the different HIV-1 variants injected directly into the blood and not dependent on selection due to passage through different host tissues (Lukashov & Goudsmit 1997). Another factor that may have to be considered when comparing disease progression in different HIV-1 exposure categories is the lower prevalence or even absence of symptomatology in acutely infected IDU, which, apparently, is a prognostic sign for a slower disease progression (Gaines et al. 1988, Sinicco et al. 1993, Pehrson et al. 1997). Earlier studies carried out by our group showed a higher frequency of peptide recognition by IDU sera in comparison to sera from individuals belonging to other exposure categories (Bongertz et al. 1999). Multiple logistic regression analyses confirmed the high importance of route of HIV-1 transmission in frequency of peptide recognition, even controlling for potential confounders. In an attempt to study the humoral immune response of IDU in more detail, samples from 48 IDU who were or had been IDU within the last year were selected from a parallel project analyzing HIV infection risk and viral hepatites in drug users (DU) (Alberti et al. 2001, Bastos et al. 2001). Fourteen HIV-1 negative DU blood samples collected at the same time were used as negative controls. Six individuals who had had a "false positive" diagnostic assay (low positivity in one of three diagnostic ELISA assays) were included as a "false positive" control group. To compare plasma from DU to those from individuals infected by sexual exposure, plasma from 60 sexually infected individuals (group S) (resident in Rio de Janeiro, in different stages of disease progression, see Bongertz et al. 1999) collected for a study aimed at analysis of the specificity of the humoral immune response in HIV-1 infection, were used. All patients signed an "informed consent" form, as approved by the Fiocruz Research Ethics Committee. Sociodemographic characteristics (age, sex) were not significantly different for the HIV-1 seropositive and HIV-1 seronegative groups (unpaired Student t test). Ten percent of the IDU and 14% of the S group individuals were undergoing highly active antiretroviral treatment at sample collection. However, all of the HIV-1 infected IDU reportedly had secondary infections or co-infections, mainly sexually transmitted diseases (STD) (gonorrhea, syphilis, genital herpes), and/or co-infections such as pneumonia, candidiasis, tuberculosis, or tested positive for hepatitis (HBV and/or HCV) (Alberti et al. 2001). In the HIV-1 seronegative drug user control group, STD was reported at a lower frequency to that reported by the HIV-1 seropositive group (p < 0.001). Other co-infections were reported at similar frequencies by both groups, but a greater proportion of HIV-1 seronegatives had no report of any of the infections reported by the HIV seropositive IDU (p < 0.001), indicating a healthier state of the negative controls. In agreement with this conclusion, mean percentiles of CD4+ lymphocytes in peripheral blood of the negative controls was higher (p < 0.0001) than that detected in blood of HIV-1 seropositive individuals (Teixeira et al. 2001a). No significant statistical differences were observed comparing the "false positive" with the control IDU group (sex, age, infections, # CD4). The seropositive IDU group was similar to the S group in regard to number of individuals, age and antiretroviral therapy (5/48 IDU and 8/60 S individuals were undergoing HAART), but differed slightly in sex (37% females in the S group versus 19% in IDU) and, importantly, in "health", in that 84% of the S group were asymptomatic at sample collection, while the great majority of the IDU group reported having different co-infections, and in that the CD4 lymphocyte percentiles were much higher in the S group (both in comparison of mean CD4%, p = 0.0291, and in number of individuals with more than 25% CD4, p = 0.0196). Mean viral loads of 4.1 logarithms of the viral copy counts in peripheral blood were determined for the IDU group. No determinations of viral load were carried out for the S plasma. ELISAs were carried out as described before (Bongertz et al. 1999) with custom made synthetic peptides (Chiron Mimotopes, San Diego, CA) using in addition to the peptides described the peptide "ELD" (= ELDKWA). Variations of this methodology were essayed (Jansson et al. 1994, Barin et al. 1996, Brown et al. 1997), but, as the relationship between IDU and S plasma reactivities remained constant, only results from one technique are shown. The peptide corresponding to the immunodominant epitope in HIV-1 gp41 (ID) was used as internal control, and peptides corresponding to consensus V3 loops of the HIV-1 gp120 belonging to different genotypes and variants circulating in Rio de Janeiro (Morgado et al. 2002) were used, as well as peptides corresponding to the HIV-1 gp120 V2 region, the gp41 "Kennedy epitope" (Cease et al. 1987) here called "peptide 735" and the above mentioned ELD peptide (Liao et al. 2000). Serial dilutions of the plasma by factors two, three, five or ten were carried out, to determine the highest dilution of the plasma still reactive with the peptides used (1:100 - 1:100,000). The results obtained are summarized in the Figure and in the Table. Reactivity was more frequent, and, interestingly, reactivity titers were much higher for IDU than for S plasma, most significantly for the V3B, V3Bbr, V3C and V3F peptides, corresponding to consensus amino-acid sequences of HIV-1 variants and subtypes prevalent in Brazil. Reactivity with the other peptides tested, although mostly higher in frequency for IDU plasma, was seldom detected in high titers (Table). Titers of antibody reactivity at dilutions above 1:1000 were detected against individual V3 peptides for only 6 of 60 sera from the S group (10%), compared to 38/46 (82.6%) of the IDU sera. Indeed, titers above 1:10,000 were observed for the majority (65%) of the IDU plasma, mostly against the V3B [10/43], V3Bbr [17/43] and V3F [10/43] peptides, with lower frequencies against the V3 Fbr [5/43] and V3C [6/43] peptides, while no such titers were observed for the V3D and V3E peptides. Therefore, the higher reactivity titer displayed by sera from infected IDU could be more indicative of specificity against prevalent HIV-1 isolates. As the IDU and S groups differed significantly in gender distribution and in relative CD4 lymphocyte concentration in peripheral blood, the data were analyzed accordingly. Although the number of samples in each group analyzed was too low to permit exhaustive multivariate statistical comparisons, when Fisher's exact test was used in a 2 x 2 contingency table, significantly higher titers were observed by sera from male individuals belonging to the IDU group compared to sera from males from the S group against the ID, 735, and the V3 peptides (ranging from p < 0.05 to p < 0.0001). When the individuals were grouped according to concentration of CD4 lymphocytes in peripheral blood, as an indicator of health of the individuals, a similar result was obtained. The 33% of IDU samples with more than 25% of lymphocytes identified as CD4 cells, compared to the corresponding group of the S samples (60%), showed significantly higher recognition titers against the ID, 735 and V3 peptides (p < 0.05). These results indicate that neither gender nor CD4 concentration are as important as the HIV-1 exposure group with respect to the higher reactivity with the synthetic peptides used in this study, similar as shown by multivariate analysis for the frequency of peptide recognition in a former study (Bongertz et al. 1999). Analysis of the influence of the HIV-1 viral load within the IDU group showed no correlation with seroreactivity, when individuals with undetectable (n = 8), low (below 30,000 HIV-1 RNA copies/ml peripheral blood, n = 25) or high viral loads (above 30.000 HIV-1 RNA copies/ml peripheral blood, n = 13) were compared. As only one of the individuals with low viral load and two individuals with high viral load were undergoing antiretroviral therapy, no analysis of the effect of viral load on seroreactivity can be shown for this study. Genetic typing of the samples was carried according to Delwart et al. (1993): 76.6% of the IDU samples were infected with HIV-1 subtype B, and 23.4% with subtype F (Teixeira et al. 2001b), a distribution similar to that determined for the S group (91% subtype B and 9% subtype F). As shown before, reactivity with peptides corresponding to consensus sequences of the different HIV-1 M group subtypes did not result in serotype results associated to the respective genotype, as the two HIV-1 subtypes observed in this study were not distinguishable using these peptides. Also, no difference in HMA genotype and serotype association could be observed for the two groups of plasma studied. However, plasma from individuals infected with F subtype HIV-1 (adding UDI and S group results) showed a significantly higher cross-reactivity with the different subtype V3 peptides (Chi-Square test, p < 0.001), and significantly higher association with the corresponding HMA subtype (Chi-Square test p = 0.004, odds ratio 1.102-1.951) The higher cross-reactivity with epitopes able to induce neutralizing antibodies in vivo in the IDU group, highly significant when reactivity with six different V3 peptides (or five genotypes) was compared, was presented by 30% of the IDU group versus 10% of the S group (p < 0.0001). As a broader humoral immune response has been associated to a better prognosis of HIV infection (Sheppard et al. 1993, Pilgrim et al. 1997) together with the higher titers of antibodies (Moore & Burton 1999), as reported here for IDU plasma, the results presented may indicate that there is a more complete humoral immune response in IDU compared to sexually infected individuals. REFERENCES
Copyright 2003 Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc03056f1.jpg] [oc03056t1.jpg] |
| |||||||||

{kind=link}
{kind=link}