 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Mem Inst Oswaldo Cruz, Rio de Janeiro, Vol. 98, No. 3, April, 2003, pp. 401-405 Species Distribution and Antifungal Susceptibility Profile of Candida spp. Bloodstream Isolates from Latin American Hospitals Patrício Godoy, Iris Nora Tiraboschi*, Luiz Carlos Severo**, Beatriz Bustamante***, Belinda Calvo****, Leila Paula de Almeida, Daniel Archimedes da Matta, Arnaldo Lopes Colombo/+ Hospital São Paulo, Escola Paulista de Medicina, Universidade Federal
de São Paulo, Rua Napoleão de Barros 740 - 7º andar, 04023-062
São Paulo, SP, Brasil *Hospital de Clínicas "José de
San Martín", Universidad de Buenos Aires, Buenos Aires, Argentina
** Instituto Especializado em Pesquisa e Diagnóstico, Santa Casa de
Porto Alegre, Porto Alegre, RS, Brasil ***Hospital "Cayetano Heredia",
Lima, Perú ****Hospital Universitário de Maracaibo, Universidad
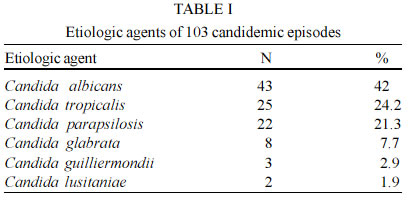
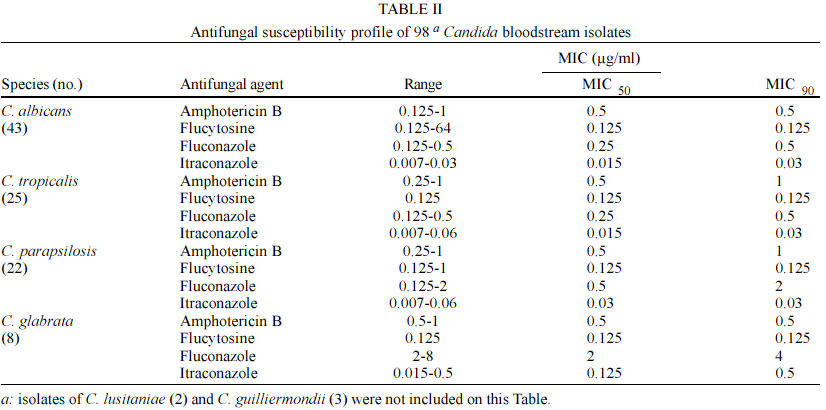
del Zulia (Luz), Maracaibo, Venezuela Received 5 July 2002 Code Number: oc03090 From March 1999 to March 2000, we conducted a prospective multicenter study of candidemia involving five tertiary care hospitals from four countries in Latin America. Yeast isolates were identified by classical methods and the antifungal susceptibility profile was determined according to the National Committee for Clinical Laboratory Standards microbroth assay method. During a 12 month-period we were able to collect a total of 103 bloodstream isolates of Candida spp. C. albicans was the most frequently isolated species accounting for 42% of all isolates. Non-albicans Candida species strains accounted for 58% of all episodes of candidemia and were mostly represented by C. tropicalis (24.2%) and C. parapsilosis (21.3%). It is noteworthy that we were able to identify two cases of C. lusitaniae from different institutions. In our casuistic, non-albicans Candida species isolates related to candidemic episodes were susceptible to fluconazole. Continuously surveillance programs are needed in order to identify possible changes in the species distribution and antifungal susceptibility patterns of yeasts that may occurs after increasing the use of azoles in Latin American hospitals. Key words: candidemia - antifungal susceptibility - Candida spp. A progressive increase in the frequency of candidemia has been observed, particularly among patients receiving antibiotics, immunosuppressive therapy, or parenteral nutrition, as well as among patients exposed to invasive medical procedures such as intravascular catheter, hemodialysis, and abdominal surgery (Lunel et al. 1999). Despite Candida albicans is still considered the most frequently isolated species of candidemic patients, the emergence of non-albicans Candida species is clearly a concern. The resistance of non-C. albicans isolates to currently available antifungal drugs represents a major challenge for future empirical therapeutic and prophylactic strategies (Krcmery & Barnes 2002). Due to the lack of information related to the epidemiology of candidemia existing in our region, we conducted a multicenter study to evaluate the species distribution and antifungal susceptibility patterns of Candida spp. bloodstream isolates in Latin American hospitals. PATIENTS AND METHODS Data collection and clinical specimens - From March 1999 to March 2000, we conducted a prospective multicenter study of candidemia involving five tertiary care hospitals from four countries in Latin America: Hospital Universitário de Maracaibo, Universidad del Zulia (Luz) , Maracaibo, Venezuela, Hospital ¨Cayetano Heredia¨, Lima, Peru, Hospital de Clínicas ¨José de San Martín¨, Universidad de Buenos Aires, Argentina, Instituto Especializado em Pesquisa e Diagnóstico, Santa Casa de Porto Alegre, Brazil and Hospital São Paulo, Escola Paulista de Medicina, Universidade Federal de São Paulo, Brazil. The centers were requested to send the isolated strains to the reference laboratory (Laboratório Especial de Micologia, Division of Infectious Diseases, Unifesp, São Paulo, Brazil) for further identification and antifungal susceptibility testing. In order to be included in this study the patient must have had at least one blood culture positive for Candida spp., drawn from a peripheral vein, and clinical evidence of sepsis. Yeast identification procedures - The purity and viability of yeast original cultures were checked by plating yeast colonies on CHROMagar Candida (CHROMagar Microbiology Paris, France). C. albicans isolates were identified if they exhibited green colonies on CHROMagar Candida and produced chlamydoconidia on corn meal-Tween 80 agar. Non-albicans Candida species isolates were identified on the basis of their micromorphology on corn meal-Tween 80 agar and biochemical tests evaluated by using the commercial system ID 32C, bioMérieux Marcy l'Etoile, France (Warren & Hazen 1995, Baumgartner et al. 1996). In vitro susceptibility testing - Antifungal susceptibility tests were performed by using the broth microdilution assay according to the methodology recommended by the National Committee for Clinical Laboratory Standards (NCCLS), document M-27 A2. The following antifungal drugs, supplied by the manufacturers as pure standard compounds, were tested: amphotericin B, fluconazole, itraconazole and 5-flucytosine. Briefly, the medium used was RPMI-1640, with L-glutamine, without bicarbonate, and buffered at pH 7.0 with 0.165 M MOPS. The yeast inoculum suspension was prepared by using a spectrophotometer to obtain a final yeast concentration containing 0.5 - 2.5 x 103 cells/ml. The assays were incubated at 35°C for 48 h. The minimal inhibitory concentration (MIC) for amphotericin B was considered the lowest tested concentration able to prevent visible growth. MIC for azoles was considered as the lowest tested concentration with a significant reduction (approximately 50%) in growth compared to growth of a positive control (NCCLS 2002). The breakpoints for azoles and 5-flucytosine MICs were those suggested by the NCCLS M27-A2. Due to a lack of consensus about the definition of MIC breakpoint for amphotericin B, arbitrary values were established according to values suggested by a previous study (Nguyen et al. 1998). Isolates with MICs ≤ 8 µg/ml for fluconazole, ≤ 4 µg/ml for 5-flucytosine, ≤ 0.125 µg/ml for itraconazole, and ≤ 1 µg/ml for amphotericin B were considered susceptible. Isolates with MICs between 16 and 32 µg/ml for fluconazole, and 0.25 to 0.5 µg/ml for itraconazole, were considered to have reduced (dose-dependent) susceptibility (DDS). MICs ³ 64 µg/ml for fluconazole, ³ 32 µg/ml for 5-flucytosine, ³ 1 µg/ml for itraconazole, and ³ 2 µg/ml for amphotericin B, were considered resistant (NCCLS M27-A2). RESULTS During a 12 month-period we were able to collect a total of 103 bloodstream isolates of Candida spp. C. albicans was the most frequently isolated species accounting for 42% of all isolates. As show in Table I, non-albicans Candida species strains accounted for 58% of all episodes of candidemia and were mostly represented by C. tropicalis (24.2%) and C. parapsilosis (21.3%). Table II shows MIC50 and MIC90 values exhibited by the four antifungal drugs tested against the most frequently isolated Candida spp. strains. C. albicans, C. tropicalis and C. parapsilosis isolates were all susceptible to fluconazole and amphotericin B. Only one C. albicans isolate was resistant to 5-flucytosine. Non-albicans Candida species isolates had higher azoles MIC values than C. albicans isolates but remained sensitive to low drug concentrations of amphotericin B. C. glabrata isolates had fluconazole MIC50 and MIC90 values of 2 and 4 µg/ml, respectively. The two isolates of C. lusitaniae were susceptible to amphotericin B (MICs of 0.125 and 0.5 µg/ml), itraconazole (MICs of 0.03 and 0.015 µg/ml) and fluconazole (MICs of 0.25 and 0.5 µg/ml). Regarding to 5-flucytosine, one isolate was susceptible (MIC = 0.125 µg/ml) and the other was intermediate (MIC = 8µg/ml). Isolates of C. guilliermondii (3) were all susceptible to amphotericin B (MICs of 0.05 and 1µg/ml), 5-flucytosine (MICs of 0.125 µg/ml) and fluconazole (MICs of 4 and 8 µg/ml). Otherwise, all three isolates had susceptibility dose dependent to itraconazole (MICs of 0.5 µg/ml). DISCUSSION Sandven (2000) reviewed 24 studies addressing episodes of candidemia in United States tertiary care hospitals and observed that the incidence of C. albicans isolates ranged from 38.8% to 79.4% of all episodes. The most prevalent non-albicans Candida species reported by the mentioned studies were C. glabrata, C. tropicalis and C. parapsilosis. Indeed, in most recent studies of candidemia conducted in United States hospitals, C. glabrata accounted for 10% to 21% of all candidemic episodes (Pfaller et al. 1998, 1999, 2000, 2001). Studies from Canada showed a different picture from the United States. In five out of six studies addressing the epidemiology of candidemia, the incidence of C. albicans isolates ranged from 53% to 74% and the non-albicans Candida species were correspondingly less prevalent. The high prevalence of C. albicans in Canada resembles the occurrence of this species in some European countries (Taylor et al. 1994, Karlowsky et al. 1997, Philips et al. 1997, Yamamura et al. 1999). According to data from SENTRY and EORTC surveys, performed between 1997 and 1999, the incidence of C. albicans at European centers ranges from 49% (EORTC) to 59% (SENTRY) of all episodes of candidemia (Viscoli et al. 1999, Pfaller et al. 2001). Voss et al. (1996), after evaluating 626 episodes of candidemia in five Dutch's hospital observed that C. albicans isolates accounted for 60% of all episodes. However, in the same study, the incidence of non-albicans Candida species raised from 20 to 40% between 1987 and 1995. In the present study we observed that C. albicans is the most frequent etiologic agent of candidemia in tertiary care hospitals from four Latin American countries, but non-albicans Candida species responded for almost 60% of all cases. In contrast with most series of candidemia from the United States and Europe, in which C. glabrata has been increasingly reported, this species represented only 7.5% of our candidemic episodes (Voss et al. 1996, Abi-Said et al. 1997). The low incidence of infections by primary azole resistant species of Candida may be related to the limited use of fluconazole in our hospitals due to cost considerations (Colombo et al. 1999). However, considering the lack of information regarding to the consume of antifungal drugs in Latin American Hospitals, this hypothesis should be appropriately evaluated by further investigations. In our casuistic, C. tropicalis was the second most frequently isolated species. The emergence of C. tropicalis as an important etiologic agent of candidemia in north hemisphere countries has been reported by several authors (Nguyen et al. 1996, Pfaller et al. 2000, 2001). Rodero et al. (1999) identified C. tropicalis as the second most common isolate related to candidemic episodes during a multicenter study performed with the participation of 12 medical centers located in Argentina, where 89 cases were evaluated. In accordance with our findings, Colombo et al. (1999) reported that C. parapsilosis and C. tropicalis were the two most common non-albicans Candida species among 145 candidemic episodes documented during a 18 month-period study including 6 different hospitals in Brazil. Costa et al. (2000), after evaluating 86 consecutive episodes of candidemia documented in a single tertiary care hospital from São Paulo, observed that C. parapsilosis and C. tropicalis responded for most of all non-albicans Candida isolates. Finally, Pfaller et al. (2001) reported that in Latin American hospitals participating of SENTRY, C. parapsilosis was the second most common Candida species causing blood stream infections. Most of our Candida bloodstream isolates were susceptible to all antifungal drug tested. However, we had one strain of C. albicans and other of C. lusitaniae that were resistant and intermediate, respectively, to 5-FC. Isolates of C. albicans primarily resistant to 5-FC have been identified in different clinical materials by several authors, varying in frequency between 0% and 38% (Iwata 1992, Barchiesi et al. 2000). The relationship between resistance to 5-FC in C. albicans and serological type was investigated by Drouhet et al. (1975), who reported that the percentage of 5FC-resistant strains isolated from patients in Africa was higher than that recovered from patients in Europe. They suggested that the high incidence of resistance among the former strains was related to the predominance of serotype B isolates (Drouhet et al. 1975). We were surprised
by the low MIC values exhibited by our C. glabrata isolates. Several
publications from north hemisphere countries have shown that C. glabrata isolates
usually exhibit high fluconazole MIC values It is noteworthy that we were able to identify two cases of candidemia due to C. lusitaniae (one reported in Brazil and the other in Argentina) and three cases of C. guilliermondii. Both pathogens have been rarely reported in different series of candidemia. Data from the Sentry Program (Pfaller et al. 2001) did not mention any specific data related to the identification of C. lusitaniae and C. guilliermondii candidemic episodes. Luzzati et al. (2000) were able to identify three cases of invasive infection due to C. lusitaniae among 189 candidemic episodes reported in the University Hospital of Verona, during the period of 1992 and 1997. In Latin America, Colombo et al. (1999) reported only three cases of candidemia due C. guilliermondii among 145 episodes reported on six different tertiary care hospitals in Brazil. Some authors advocate that C. lusitaniae isolates may present innate resistance to amphotericin B (Pfaller et al. 1994, Hadfield et al. 1997). However, the amphotericin B MIC results exhibited by both isolates of C. lusitaniae from our series were 0.125 and 0.5 µg/ml respectively. This aspect may be related to the limitations of the methodology we used to recognize isolates truly resistant to amphotericin B. The NCCLS methodology yields a range of MICs that span only three to four twofold serial dilutions, what make difficult a reliable discrimination between susceptible and resistant isolates (Rex et al. 1995). Considering the mentioned limitation of the NCCLS methodology, some authors have suggested to use the Etest with standardized RPMI medium supplemented with 2% glucose as the most sensitive and reliable means for detecting amphotericin B resistance (Wanger et al. 1995, Peyron et al. 2001). Although C. albicans continues to account for approximately one-half of all episodes of candidemia reported worldwide, its frequency may vary widely from institution to institution. We were able to demonstrate that in South America most non-albicans Candida species are represented by C. tropicalis and C. parapsilosis isolates still susceptible to amphotericin B and fluconazole. However, continuously surveillance programs are needed in order to identify possible changes in the species distribution and antifungal susceptibility patterns of yeasts, particularly after increasing the use of azoles in Latin American hospitals. REFERENCES
Copyright 2003 Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc03090t2.jpg] [oc03090t1.jpg] |
| |||||||||

{kind=link}
{kind=link}