 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Mem Inst Oswaldo Cruz, Rio de Janeiro, Vol. 98, No. 5, July, 2003, pp. 599-603 Hepatitis B and C in the Hemodialysis Unit of Tocantins, Brazil: Serological and Molecular Profiles Karla P Souza, Jônio A Luz, Sheila A Teles*, Megmar AS Carneiro, Luciana A Oliveira, Adriane S Gomes, Márcia A Dias, Selma A Gomes**, Clara FT Yoshida**, Regina MB Martins/+ Instituto de Patologia Tropical
e Saúde Pública *Faculdade de Enfermagem, Universidade Federal
de Goiás, Caixa Postal 131, 74605-050 Goiânia, GO, Brasil **Departamento
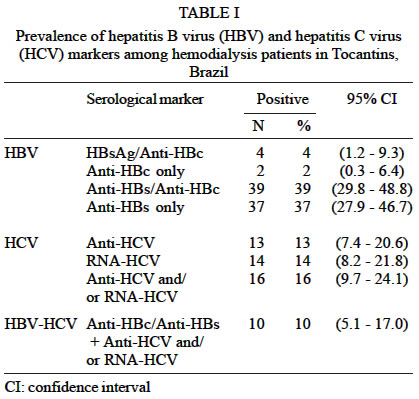
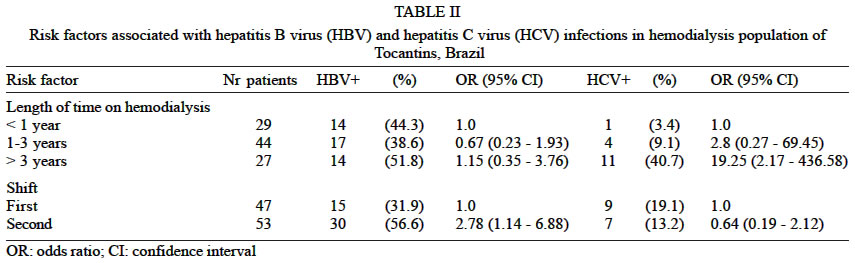
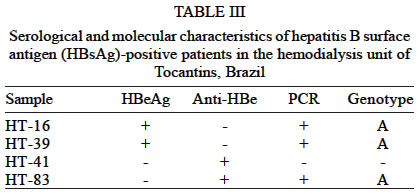
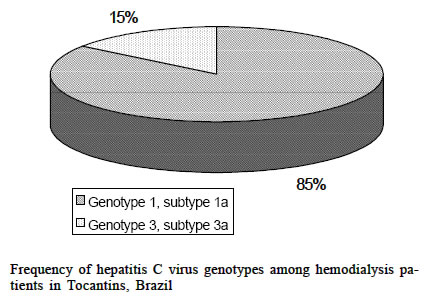
de Virologia, Instituto Oswaldo Cruz-Fiocruz, Rio de Janeiro, RJ, Brasil This work received financial support from CNPq. Received 14 January 2003 Code Number: oc03127 A survey was conducted in the hemodialysis population of the state of Tocantins, Brazil, aiming to assess the prevalence of hepatitis B virus (HBV) and hepatitis C virus (HCV) infections, to analyze associated risk factors, and also to investigate these viruses genotypes distribution. During January and March 2001, all patients (n = 100) were interviewed at the unique dialysis unit in Tocantins. Blood samples were collected and serum samples were screened for HBV serological markers. Hepatitis B surface antigen positive samples were tested for HBV DNA. All samples were also tested for anti-HCV antibodies and HCV RNA. An overall prevalence of 45% was found for HBV infection (4% were HBsAg/anti-HBc positive, 2% were anti-HBc only and 39% had anti-HBc/anti-HBs markers). Concerning HCV infection, anti-HCV and HCV RNA were detected in 13% and 14% of the subjects, respectively. Three patients were HCV RNA positive and anti-HCV negative, resulting in an overall HCV prevalence of 16%. Univariate analysis of risk factors showed that only shift and length of time on hemodialysis were associated with HBV and HCV positivity, respectively. Among the four HBsAg-positive samples, HBV DNA was detected in three of them, which were identified as genotype A by restriction fragment length polymorphism (RFLP) analysis. All 14 HCV RNA-positive samples were genotyped by INNO-LiPA. Genotypes 1a and 3a were found in 85% and 15%, respectively. The present data show low HBsAg and HCV prevalence rates. The risk factors associated with HBV and HCV positivity suggest that nosocomial transmission may influence in spreading these viruses in the dialysis unit studied. Key words: hepatitis B virus - hepatitis C virus - hemodialysis - prevalence - risk factors - genotypes - Tocantins - Brazil Hepatitis B virus (HBV) and hepatitis C virus (HCV) are important causes of liver diseases, including cirrhosis and hepatocellular carcinoma. The number of HBV chronic carriers is approximately 350 million worldwide. Regarding HCV, about 170 million people have been infected with this agent (Poovorawan et al. 2002). HBV is an enveloped, double-stranded DNA virus that presents a constrained evolution due to the overlapping nature of its genes, with a rate of nucleotide substitutions in order of 5 x 10-5/site/year. HBV isolates have been classified into eight genotypes (A to H), considering a divergence of more than 8% in the entire virus genomic sequence (Okamoto et al. 1988, Norder et al. 1994, Stuyver et al. 2000, Arauz-Ruiz et al. 2002). HCV is a positive-sense, single-stranded RNA virus that presents a high mutation rate (10-3 substitutions/site/year). HCV isolates have been classified in at least six different genotypes (1 to 6), each comprising multiple subtypes (designated a, b, c, etc.) (Simmonds et al. 1994, Zein 2000). Since both viruses are efficiently transmitted by parenteral route, patients undergoing hemodialysis are at high risk of acquiring these bloodborne hepatitis agents (Cañero-Velasco et al. 1998, Covic et al. 1999, Vladutiu et al. 2000). In addition, infected patients have an increased tendency to develop chronic hepatitis and also to be a potential reservoir for its transmission (Goldbloom & Reed 1980, Harnett et al. 1988). Before infection control practices and hepatitis B vaccination, high prevalence rates of HBV markers were found in hemodialysis patients globally (Szumeness et al. 1974, Löfdgren et al. 1982). In developed countries where these measures have been implemented, HBV infection declined significantly, reaching hepatitis B surface antigen (HBsAg) rates lower than 1%, as observed in the US (Alter et al. 1986, Tokars et al. 2002). In Brazil, investigations have shown prevalence rates ranging from 4.4% to 15.1% (Cenderoglo Neto et al. 1995, Busek et al. 2002, Teles et al. 2002). Regarding HCV infection in hemodialysis patients, studies showed rates ranging from 3.4%, in the Netherlands (Schneeberger et al. 2000), to more than 70%, in Eastern Europe (Vladutiu et al. 2000). In our country, HCV prevalence rates of 20.3%, 23.8%, 33.4% and 39% were recently found in Santa Catarina (Moraes 2001), Bahia (Santana et al. 2001), Minas Gerais (Busek et al. 2002), and Goiás (Carneiro et al. 2001), respectively. The state of Tocantins was created in 1988. It is located in the North of Brazil, a region of low economic conditions. Up to now there is no data concerning HBV and HCV infections in patients undergoing hemodialysis in this region. Therefore, the present study aims to assess the prevalences of hepatitis B and C in hemodialysis population of Tocantins, to analyze risk factors associated to these infections, and also to investigate the HBV and HCV genotypes distribution in this population. MATERIALS AND METHODS Patients - Our study was carried out in the hemodialysis unit of Araguaína city, which represents the unique unit in the state of Tocantins (1,131,005 inhabitants). During January and March 2001, all chronic hemodialysis patients (N = 100) were interviewed for risk factors to HBV and HCV infections and for hepatitis B vaccination. The studied population ranged in age from 13 to 82 years old (average 47.6 years). Sixty-two (62%) were males and 38 (38%) were females. A standardized form was used to collect data on age, sex, history of hepatitis/jaundice, length of time on hemodialysis treatment, number of previous transfusions, acupuncture, tattooing, intravenous drug use, multiple partners, sexually transmitted diseases, and household contact with hepatitis/jaundice. Permission for carrying out the study was granted by the institution involved and informed consent was obtained from all participants. The study was approved by the Ethical Committee of the Federal University of Goiás. Serological tests - Blood samples were collected from all patients and sera were stored at -20ºC. Serum samples were screened by enzyme-linked immunosorbent assays (ELISA) for the presence of the following hepatitis B viral markers: HBsAg, hepatitis B surface antibody (anti-HBs) and hepatitis B core antibody (anti-HBc) (Hepanostika Uni-form Organon Teknika B.V., Boxtel, Holland). HBsAg-positive samples were submitted to hepatitis B e antigen (HBeAg) and hepatitis B e antibody (anti-HBe) detection (Hepanostika Uni-form Organon Teknica). All samples were also tested for hepatitis C antibody (anti-HCV) by ELISA (HBK 520 HEMOBIO HCV, Embrabio). Positive samples were retested for confirmation, using line immunoassay (INNO-LIA HCV Ab III, Innogenetics). Detection and genotyping of HBV DNA - DNA was extracted from 250 µl of serum samples, as described elsewhere (Niel et al. 1994). PCR was carried out in a final volume of 50 µl in 35 cycles under the following conditions: 95ºC for 30 s, 52ºC for 1 min, 72ºC for 1 min, final elongation at 72ºC for 7 min. Four primers pairs were used to amplify HBV fragments which, taken together, encompassed 81% of the genome: PS1-PS2 and X1-X2 (Niel et al. 1994), C1-PS2 and PS4-S2 (Gomes et al. 1996). The PCR products were subjected to RFLP analysis, as previously described by De Castro et al. (2000). Detection and genotyping of HCV RNA - All samples were submitted to RNA extraction, reverse transcription, and a nested PCR with primers complementary to the conserved area of the 5' non-coding region of HCV, essentially as described by Ginabreda et al. (1997). Positive samples were genotyped by line probe assay (INNO-LiPA HCV, Innogenetics NV, Ghent, Belgium). Statistical analysis - Prevalence and 95% confidence intervals (95% CI) were calculated. Risk factors, estimated by odds ratio, were detected by univariate analysis. Statistical significance was assessed at the 0.05 probability level in all analyses. Statistical evaluations were performed using Epiinfo 6.0, a program developed by Centers for Disease Control and Prevention (Atlanta, GA). RESULTS Of the 100 hemodialysis patients, 4 (4%) were HBsAg/anti-HBc positive, 2 (2%) were anti-HBc only and 39 (39%) had anti-HBs/anti-HBc markers, resulting in a HBV prevalence infection of 45%. Anti-HBs isolated (vaccinated) was present in 37 (37%) patients. Concerning HCV infection among this population, anti-HCV and HCV RNA were detected in 13 (13%) and 14 (14%) subjects, respectively. Three patients were HCV RNA positive and anti-HCV negative, resulting in an overall HCV prevalence of 16%. HBV and HCV infection markers were detected in 10 (10%) patients (Table I). Among all risk factors studied, only shift and length of time on hemodialysis were significantly associated with HBV and HCV positivity, respectively. Subjects undergoing hemodialysis during the second shift had a 2.78-fold (95% CI: 1.14 - 6.88) greater risk of HBV positivity, compared to those that had dialyzed during the first shift. Regarding HCV infection, patients under treatment for more than three years had 19.25-fold (95% CI: 2.17 - 436.58) greater risk of seropositiviy, compared to subjects who had undergone less than one year (Table II). Table III shows the serological and molecular characteristics of the four HBsAg-positive hemodialysis patients. Two samples were HBeAg and the two others anti-HBeAg reactive. HBV DNA was detected in three samples: two HBeAg and one anti-HBe-positive serum sample. All were identified as genotype A by RFLP. All 14 HCV RNA-positive samples were genotyped by INNO-LiPA. Genotype 1 (subtype 1a) was predominant (85%). Genotype 3 (subtype 3a) was detected in two patients (15%) (Figure). DISCUSSION The present study represents the first investigation of HBV and HCV prevalences in hemodialysis patients in the state of Tocantins, Brazil. Almost half of the patients studied here had already suffered a HBV infection, and 4% were HBsAg carriers. This HBsAg prevalence was higher than those found in developed countries as Spain (2.2%) (López-Alcorocho et al. 2001), Switzerland (1.6%) (Ambühl et al. 2000), and the US (0.9%) (Tokars et al. 2002). However, this rate was lower than those observed in other studies conduced before the implementation of improved methods for prevention and control of infection in Brazilian hemodialysis units (Cenderoglo Neto et al. 1995, Vanderborght et al. 1995). In fact, recently Teles et al. (2002) reported a decline of the HBsAg prevalence from 12%, in 1995, to 5.8%, in 1999, among hemodialysis patients from Goiânia city. High anti-HCV prevalence rates have been found in hemodialysis patients worldwide, but more frequently in developing countries. Recent data from Indonesia, Syria, and Jordan revealed rates of 63.4%, 48.9% and 34.6%, respectively (Othman & Monem 2001, Bdour 2002, Chanpong et al. 2002). In Brazil, anti-HCV prevalence ranges from 20.3% to 64.7% (Vanderborght et al. 1995, Carneiro et al. 2001, Santana et al. 2001, Busek et al. 2002). Thus, the prevalence of 13% found in hemodialysis patients in Tocantins could be placed in a low position. Three subjects were HCV RNA positive and anti-HCV negative. Retesting confirmed this result. This laboratorial profile has been observed in some hemodialysis patients (Scheneeberger et al. 2000, Carneiro et al. 2001, Busek et al. 2002, Hinrichsen et al. 2002), and seems to be related to their prolonged anti-HCV negative window phase (Scheneeberger et al. 2000) or impaired immune response (Goldbloom & Reed 1980). Ten patients (10%) were positive for HBV and HCV markers. These viruses are transmitted by parenteral mode. Thus, this co-infection has not been a rare event, and rates ranging from 5% to 62.7% have been observed in other hemodialysis populations (Cañero-Velasco et al. 1998, Covic et al. 1999, Vladutiu et al. 2000, Otham & Monem 2001). In the present study, subjects undergoing hemodialysis during the second shift had a 2.78-fold (95% CI: 1.14 - 6.88) greater risk of HBV positivity compared to those that had dialyzed during the first shift. This was also demonstrated elsewhere (Covic et al. 1999). Although hemodialysis machine disinfection procedures are similar between shifts, the complete cleaning and disinfection procedure of all surfaces is usually made at the end of the day. Since HBV is able to survive in the environment (Bond et al. 1981), hemodialysis staff may unexpectedly transfer virus from contaminated surfaces to patients by hands or through the use of contaminated equipment and supplies (Pugliese & Favero 1996). Many investigations have demonstrated that duration of hemodialysis treatment is strictly correlated with hepatitis C positivity, suggesting HCV nosocomial transmission (Schneeberger et al. 2000, Hinrichsen et al. 2002). In fact, our patients under treatment for more than three years had 19.25-fold (95% CI: 2.17- 436.58) greater risk of HCV infection, compared to subjects who had undergone less than one year. Although blood transfusion has been pointed out as an important risk factor for viral hepatitis within hemodialysis population (Covic et al. 1999, Chanpong et al. 2002, Hinrichsen et al. 2002), in the present investigation this factor was not associated with HBV and HCV infections. Therefore, probably the screening of blood products for HBsAg, anti-HBc and anti-HCV in Brazilian blood banks, and the use of erythropoietin for anemia treatment should have contributed to reduce this risk among our hemodialysis patients. HBV genotypes A, D and F have been found in Brazilian hemodialysis population (De Castro et al. 2000, Carrilho 2001, Teles et al. 2002), reflecting the HBV genotypes circulating in our country (Moraes et al. 1996). In the present study, only HBV genotype A strains were detected in the hemodialysis patients. Two HCV genotypes were identified in the hemodialysis patients in Tocantins: subtypes 1a and 3a. Nevertheless, the first was highly predominant. Recently, Busek et al. (2002) have also found a high frequency of this genotype in hemodialysis patients in Minas Gerais. In conclusion, although HBsAg and HCV rates in hemodialysis patients of Tocantins are smaller than those found in other Brazilian units, they are still high. The findings that hemodialysis in the second shift and duration of treatment were associated with HBV and HCV sero-positivy, respectively, suggest nosocomial transmission. Also, the results of HBV and HCV genotypes corroborate this hypothesis, reinforcing the need for stricter adherence to infection control measures in dialysis units. ACKNOWLEDGEMENTS To the patients and staff of the hemodialysis unit of Araguaína city, Tocantins. To Cristiane SCC Galvão and Marco Antônio C Galvão for their collaboration in this study. REFERENCES
Copyright 2003 Instituto Oswaldo Cruz - Fiocruz. Free, full-text also available from http://www.memorias.ioc.fiocruz.br The following images related to this document are available:Photo images[oc03127t3.jpg] [oc03127t1.jpg] [oc03127t2.jpg] [oc03127f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}