 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Mem Inst Oswaldo Cruz, Rio de Janeiro, Vol. 98, No. 6, Sept, 2003, pp. 721-725 Prevalence of Helicobacter pylori Infection in Warao Lineage Communities of Delta Amacuro State, Venezuela Diana Ortiz/+, María Eugenia Cavazza, Orquídea Rodríguez, Isabel Hagel, MaríaCorrenti*, Jacinto Convit Instituto de Biomedicina, Ministerio
de Salud y Desarrollo Social, Universidad Central de Venezuela, Apartado
Postal 4043, Caracas 1010A, Venezuela *Instituto de Oncología y Hematología,
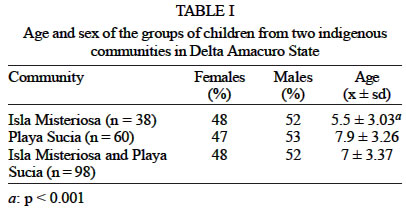
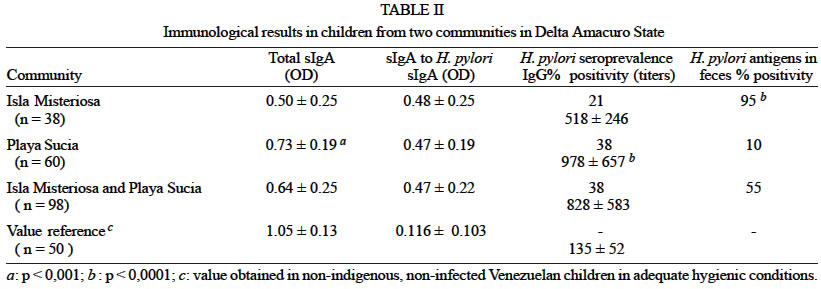
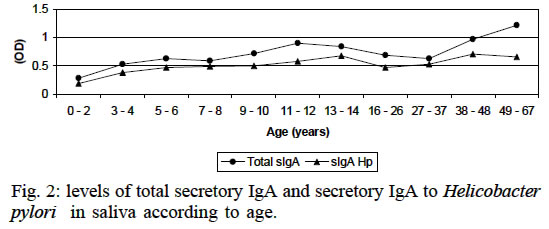
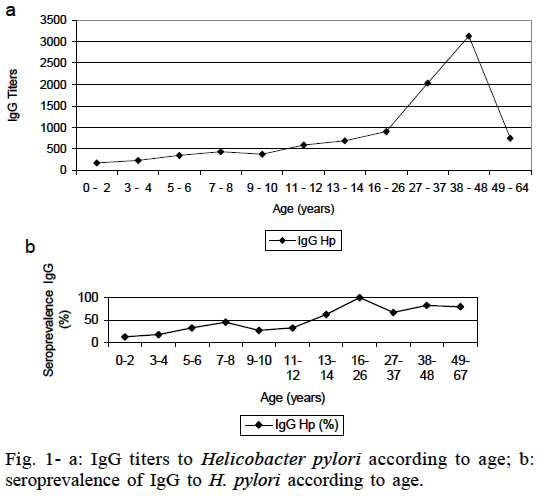
Ministerio de Salud y Desarrollo Social, Caracas, Venezuela This investigation was financed by Conicit Project S1-96001408, and by the Program for Special Attention to Indigenous Populations, coordinated by General Victor Salom the National Guard of Venezuela. Received 5 July 2002 Code Number: oc03148 The purpose of this study was the evaluation of Helicobacter pylori infections in children and adults from two indigenous communities of Delta Amacuro State, Venezuela, that differ in hygienic conditions of the housing. The evaluation was performed in 98 children (mean age 7 ± 3.37 years) and their mothers (33.96 ± 13.77 years) from two communities of Warao lineage. Anti-H. pylori serum IgG and secretory anti-H. pylori IgA antibodies were de-termined, as well as total secretory IgA and H. pylori antigens in feces. Serological prevalence of H. pylori infection was 38% in children and 84% their in mothers. Children from the community that had the most deficient sanitary and hygienic conditions had significantly lower titers of specific IgG antibodies and total secretory IgA (P < 0.0001) and a high percentage of them had H. pylori antigens in their feces (P < 0.0001). The levels of specific IgA were similar in both groups. The results indicate that in these populations there is a high prevalence of H. pylori infection and that poor hygienic conditions can increase the risk of infection and damage to the gastrointestinal tract. Key words: Helicobacter pylori - secretory IgA - seroprevalence - Venezuela Helicobacter pylori colonizes about 50% of the world population; less than 20% of affected individuals develop gastroduodenal diseases. Gastroduodenal diseases associated with H. pylori occur mainly in adults. Nevertheless, the infection is usually acquired during childhood (Wotherspoon et al. 1993) and it is possible that the humoral and mucosal tissue responses at that time can determine the natural course of the infection (Torres et al. 2000). Although studies suggest that the majority of individuals acquire H. pylori in childhood, the mi-crooganism can persist in its gastric habitat for decades. It is acquired from another family member (Brenner et al.1999, Rothenbacher et al.1999). During this time, it can undergo considerable genetic changes that could facilitate adaptation to the gastric ecosystem of a particular host, including changes in environmental features brought about by H. pylori colonization (Falk et al. 2000). H. pylori isolates from un related individuals have totally different genetic fingerprints, so that H. pylori can be considered a "quasi-species" (Covacci et al. 1997). It has been reported at a worldwide level that H. pylori infection prevalence in children varies between 10% and 80% (Vaira et al. 1994, Torres et al. 2000). The lowest prevalence has been found in populations in Northern and Eastern Europe, Japan and other parts of Asia. High prevalence has been well documented in India and Bangladesh and in certain cities of Africa and Latin America (Torres et al. 2000). In a study where prevalence by ethnic category was examined, an increase in immigrant groups from high prevalence regions was reported, as well as in low socio-economic level ethnic risk groups (Ma et al. 1998, Vorobjova et al. 2000). Again increase with age, low socio-economic and educational levels, race, crowded living quarters, migration from high prevalence regions, background of H. pylori-infected family members, poor nutritional state indicators, ingestion of water and vegetables which do not fulfill hygienic conditions, have been reported as risk factors for the increase of H. pylori infection (Graham et al. 1991, Smoat et al. 1994, Torres et al. 2000). Few studies have examined the incidence of H. pylori infection in children, possibly due to the ethical considerations involved in carrying out invasive tests which are not really required in these age groups. On the other hand, studies in indigenous communities are troublesome to carry out because of the difficulties of both physical and cultural accessibility. The main purpose of this study was the evaluation of H. pylori infection in children and adults from two indigenous communities of Delta Amacuro State in Venezuela. MATERIALS AND METHODS Study population - Ninety-eight children, males and females with ages between 1 and 14 years (average 7 ± 3.37 years) and 32 adult women (33.96 ± 13.77 years) from two indigenous communities of Warao lineage, Pedernales municipality, Delta Amacuro State, were evaluated (Table I). This state has a tropical rainy climate and swampy grounds of the tropical hydromorphic type. Its com-munities are dispersed along the banks of the Orinoco River Delta, living mainly from hunting and fishing. The study protocol was approved by the Ethics Committee of the Institute de Biomedicine, Faculty of Medicine of Universidad Central de Venezuela, and by competent authorities of Delta Amacuro State. The characteristics of the studied population were compared with values obtained from non-indigenous, non-infected Venezuelan groups that live under adequate hygienic conditions. Serum determination of IgG to H. pylori - The determination of specific IgG antibodies was done using a commercial immunoenzymatic kit (PYLORISET EIA-G, ORION Diagnostic Laboratories) . The plates were read in a spectrophotometer at 405 nm and the optical density units were extrapolated in a graph on semi-logarithmic paper, using as reference the standards supplied with the kit. The results obtained were expressed in antibody titers (positive titers > 300). Determination of secretory IgA to H. pylori in saliva - Specific secretory anti-H. pylori IgA in saliva was determined using an ELISA technique standardized in our laboratory. For this purpose we collected saliva from each subject directly from the mouth. The samples were kept in vacutainer tubes with ethylenediaminotetracid (EDTA) at -20oC until use. The polystyrene plates (Nunc MaxiSorp) were sensitized with the H. pylori antigen (2.5 µg per well) diluted in coating buffer pH 9.6 during 2 h at 37oC. Non-specific sites were blocked with 0.5% PBST-BSA during 2 h at 37oC, then the saliva samples were incubated during 1 h at 37oC at a 1:10 dilution in 0.5% PBST-BSA. The conjugate was peroxidase-labeled anti-IgA (SIGMA) diluted 1:1000 in 5% PBST-BSA. After incubation at 37oC for 1 h, the reactions were developed with o-phe-nylenediamine (SIGMA) and H2O2, reading at 492 nm absorbance. Values 0.300 units of optical density were considered positive; this cut-off was determined in previous studies (Ortiz et al. 2001). Antigen preparation - A crude antigen prepared from five strains isolated from patients with duodenal ulcer (DU) and H. pylori infection confirmed by the four conventional criteria was used. The H. pylori strains isolated were inoculated in chocolate and blood cultures mediums and the harvesting of the microorganisms was done by adding 2 ml of sterile PBS to the agar plates and harvesting the bacteria. The harvested bacteria were centrifuged at 2 000 rpm to obtain a pellet, which was washed 2 x with PBS. The cells were then submitted to 5 sonication cycles of 30 s each, then the samples were centrifuged at 14 000 rpm in an Eppendorf centrifuge and the protein concentration of the supernatant was determined by the Lowry method (Lowry et al. 1951). SDS-polyacrilamide (10%) gel electrophoresis was carried out with the cell sonicate to visualize the protein bands. For this purpose it was diluted in sample buffer (Tris HCL 0.06M, pH 6.8, 2% SDS, 10% glycerol, 5% 2-mer-captoethanol, 0.001% bromophenol blue). Determination of total secretory IgA in saliva - To determine total secretory IgA in saliva we used the ELISA technique previously described (Ortiz et al. 2001). Determination of H. pylori antigens in feces - For the determination of H. pylori antigens in fecal material we used a commercial qualitative immunoenzymatic diagnostic method (PREMIER PLATINUM HpSA Kit, Meridian Diagnostic, Inc.) and the plate was read at 450 nm absorbance. Samples with absorbance values less than 0.140 were considered negative, those with values between 0.140 and 0.160 were regarded as ambiguous, and those with results equal to or greater than 0.160 were reported as positive. Statistical analysis - The geometric means and standard deviations of the titers of specific IgG antibodies were calculated, as well as the total and specific secretory IgA. The various groups were compared using Student's t test, and the differences among proportions were compared applying the Chi-square (χ2) test. RESULTS Regarding the immunological parameters studied in the children, we found a prevalence of positive tests for humoral H. pylori IgG antibodies of 38% (828 ± 583 titers); the titers were significantly more elevated in the Playa Sucia community than in Isla Misteriosa (p < 0.0001). The mean value of total secretory IgA in saliva was sig-nificantly higher (p < 0.001) in children from the Playa Sucia community than in those of the Isla Misteriosa community. Nevertheless, secretory IgA to H. pylori values in saliva were similar in both groups (0.47 ± 0.22 OD), above the cut off established for children not infected by H. pylori. The evaluation of the presence of H. pylori antigens in feces, showed a positivity of 95% in children from Isla Misteriosa, compared to 10% in the Playa Sucia group (Table II). When studying the group of women, we found 84% of seroprevalence of H. pylori infection, (2288 ± 2005 specific IgG titers). The values of total secretory IgA were also measured (0.82 ± 0.32 OD) and the values of secretory IgA to H. pylori in saliva (0.57 ± 0.21 OD) were significantly higher (p < 0.05) than the value obtained of adults not infected by H. pylori. This values were significantly higher (p < 0.0001) in mothers that in the children. An increase of total and specific secretory IgA to H. pylori (Fig. 2) measured in saliva, as well specific IgG antibodies (Fig. 1a,b), were observed with age progression. Seroprevalence of infection increased with age, and the highest titers were seen at age 40, with a decrease from that age on. The total secretory IgA and specific secretory IgA to H. pylori in relation to age, appeared to stabilize from 35 years on (Fig. 2). DISCUSSION In our country there is a high prevalence of H. pylori infection in adults and children (Piñero et al. 2000, Ortiz et al. 2001). In spite of the fact that there are many reports on the prevalence of infection with this bacterium, very few studies have been carried out in indigenous population. The titers of the children who were evaluated in two Delta Amacuro State communities, were elevated according to the upper normal limit. No differences between the seroprevalence in the two communities were apparent. Seroprevalence is high and similar to that reported for other rural children populations in Venezuela (Piñero et al. 2000, Ortiz et al. 2001), and other countries (Bode et al. 1998, Elitsur et al. 1998, Torres et al. 1998). This is important since it has been reported that high titles are associate with a lesser likelihood of gastric carcinoma compared to low titer (Fujioka et al. 2001). On the other hand, average value of the total secretory IgA levels was significantly lower than that found in groups of children from other rural communities of non-indigenous Venezuelans (Ortiz et al. 2000) and also significantly lower than in healthy children without any gastrointestinal pathology. With regard to mucosal immunity, it is clear that local IgA antibody plays a primary role en protection against foreign organisms (Goto et al. 1999). Therefore, deficiencies in the production of this antibody could be an indicator of damage of mucosal tissues. The environmental hygienic and socio-economic conditions of these children are low and they are permanently exposed to a variety of infections which compromise the gastrointestinal mucosal tissue, it is possible that there may be immunological alterations of the gastrointestinal tract. This effect could generate deficiencies of secretory IgA production or it may inhibit the exposure of Th2 cells to luminal antigens, which favor the positively selected response of IgA antibodies (Ernest et al. 1999). Thus alterations of regulatory mechanisms of the immune response could direct it towards a chronic inflammatory process of the gastric mucosal tissue. In addition, is possible that there may be some ethnic susceptibility effect. No differences were found in the levels of specific secretory IgA to H. pylori between communities. Nevertheless, the values are above the cut-off point established in previous studies (Ortiz et al. 2000), suggesting the development of a local specific immune response through the production of secretory IgA to H. pylori antibodies. It has been reported that during H. pylori infection, levels of local and specific IgA to H. pylori antibodies increase (Wyatt et al. 1988, Taylor & Blaser 1991). When comparing both communities, we found that the mean age of children from the Playa Sucia community was higher, and this could be one of the factors which explains why the levels of total secretory IgA and the titers of IgG to H. pylori were significantly higher than those found in children from the Isla Misteriosa community. In fact, it has been observed that the development of immunological memory and antibody titers progressively increase with age (Graham et al. 1991). We also found a higher percentage of children with fecal H. pylori antigens in the Isla Misteriosa community, which suggests that probably there are more children with recent infection in this population. Regarding the socio-economic and cultural characteristics, the communities studied belong to Warao lineage and they present a high proportion of homes in a state of poverty, considering the inadequate hygienic conditions and the low family incomes, insufficient to cover the amounts needed for feeding the family. Environmental conditions can significantly influence the general state of health of human beings, modulating the immune response (Ortiz et al. 2000) and high rates of H. pylori infection being associated with low socio-economic status, high densities of living and poor hygienic conditions (Mitchell & Mégraud 2002). Even if it is true that both communities belong to the Warao lineage and their geographical characteristics are similar, it should be also considered that Playa Sucia is a community which has been organized through a pilot program sponsored by the Regional Environmental Sanitation Direction of the Ministry of Health and Social Development of Venezuela since 1998. This program has implanted policies which improve living and environmental sanitation conditions. On the contrary, in the Isla Misteriosa community the hygiene and sanitation conditions are very deficient, the dwellings are primitive lake dwellings built on the riverbanks themselves, where there are marshes and swamps. This produces optimal conditions for the development of microorganisms and other infectious agents, generating a permanent infection source for its inhabitants, increasing the infection risk and therefore the damage to the gastrointestinal mucosal tissue. Even though the H. pylori transmission mode is not well established, fecal-oral and oral-oral modes of transmission have been suggested (Grübel et al. 1998) and intrafamilial transmission is important on the acquisition of infections (Miyazaki et al. 2002, Taneike et al. 2001). H. pylori has been cultured from vomitus, saliva, and diarrheal stool (Smith & Parsonnet 1998). This study indicate that these communities present a high prevalence of H. pylori infection and that the hygienic conditions can influence the prevalence of the infection and may increase the risk of damage to the gastrointestinal mucosal tissue, influencing the course of the infection. It is important to continue studies in this type of community where infections are recurrent and the damage to the gastric mucous tissue can become a chronic problem generating a permanent immunological challenge as well. ACKNOWLEDGEMENTS To Dr Marian Ulrich and Dr Mario Sanchez Borges for reviewing the manuscript. To the local authorities of Delta Amacuro State. Mrs Niria Zabaleta and Lourdes Becerra collaborated in the evaluation of the children. To Warao indigenous populations for allowing us to enter and participate in their communities. REFERENCES
Copyright 2003 Instituto Oswaldo Cruz - Fiocruz. Free, full-text also available from http://www.memorias.ioc.fiocruz.br The following images related to this document are available:Photo images[oc03148f1.jpg] [oc03148t2.jpg] [oc03148f2.jpg] [oc03148t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}