 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Mem Inst Oswaldo Cruz, Rio de Janeiro, Vol. 98, No. 6, Sept, 2003, pp. 831-837 Human Immunodeficiency Virus Type 1: Drug Resistance in Treated and Untreated Brazilian Children SRR Simonetti+, HG Schatzmayr, JP Simonetti Núcleo de Retrovirus, Departamento
de Virologia, Instituto Oswaldo Cruz-Fiocruz, Av. Brasil 4365, 21045-900
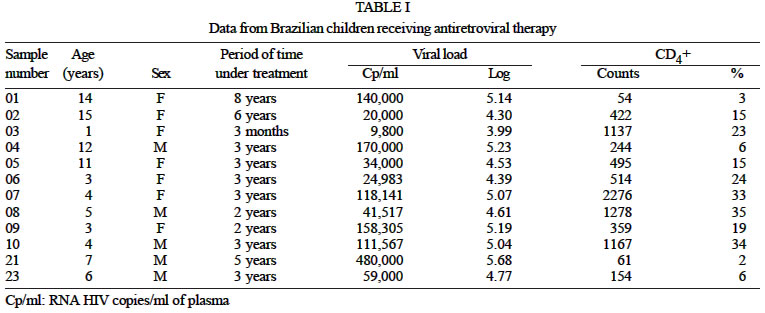
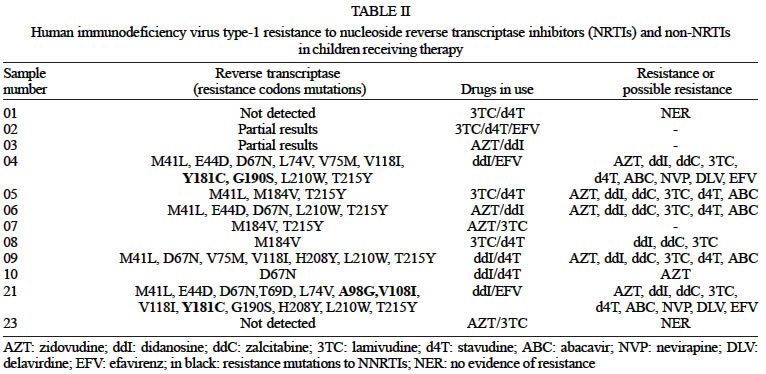
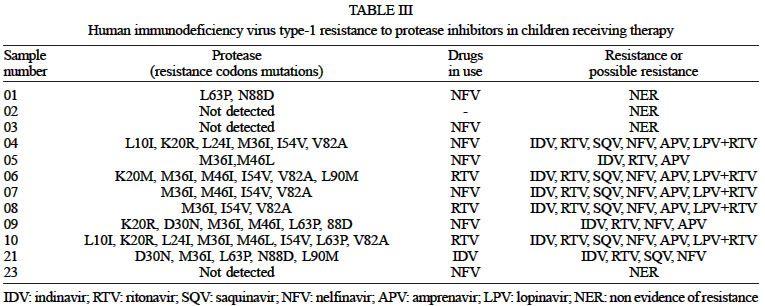
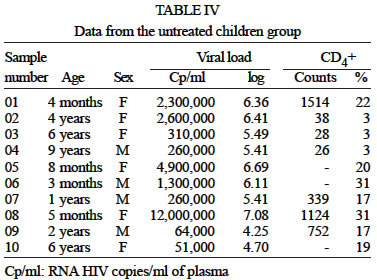
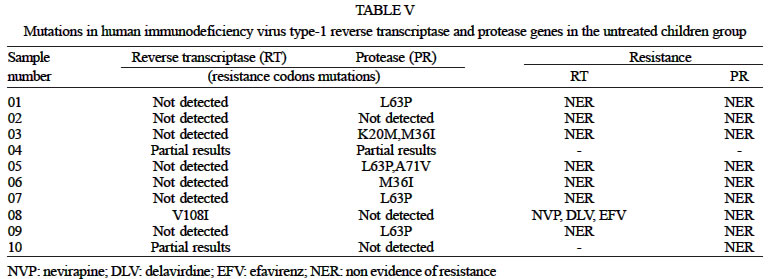
Rio de Janeiro, RJ, Brasil This work received financial support from the Ministério da Saúde, Brazil. Received 24 January 2003 Code Number: oc03167 Twenty-two vertically human immunodeficiency virus type 1 (HIV-1) infected Brazilian children were studied for antiretroviral drug resistance. They were separated into 2 groups according to the administration of antiretroviral therapy into those who presented disease symptoms or without symptoms and no therapy. Viral genome sequencing reactions were loaded on an automated DNA sampler (TruGene, Visible Genetics) and compared to a database of wild type HIV-1. In the former group 8 of 12 children presented isolates with mutations conferring resistance to protease inhibitors (PIs), 7 presented isolates resistant to nucleoside reverse transcriptase inhibitors (NRTIs) and 2 presented isolates resistant to non-nucleoside reverse transcriptase inhibitors (NNRTIs). Ten children were included in the antiretroviral naïve group. Eight were susceptible to NRTIs and all of them were susceptible to PIs; one presented the V108I mutation, which confers low-level resistance to NNRTIs. The data report HIV mutant isolates both in treated and untreated infants. However, the frequency and the level of drug resistance were more frequent in the group receiving antiretroviral therapy, corroborating the concept of selective pressure acting on the emergence of resistant viral strains. The children who presented alterations at polymorphism sites should be monitored for the development of additional mutations occurring at relevant resistance codons. Key words: human immunodeficiency virus type 1 (HIV-1) - genotyping - drug resistance - Brazilian children Human immunodeficiency virus type 1 (HIV-1) drug resistance arises from mutations in the viral genome, specifically in the regions that encode the molecular targets of therapy (Mitsuya et al. 1990) in such a way that the protease (PR) and reverse transcriptase (RT) enzymes function is no longer inhibited by the drug, leaving the virus to replicate freely. Therapy options for the management of HIV-1 disease include nucleoside analogue reverse transcriptase inhibitors (NRTIs), non-nucleoside reverse transcriptase inhibitors (NNRTIs) and protease inhibitors (PIs). Drug resistance mutations to all of these inhibitors have been identified even in previously non-treated patients (Nájera et al. 1995, Brenner et al. 2002). The so-called highly active antiretroviral therapy (HAART) consists of antiretroviral drug combinations including 2 NRTIs and/or NNRTIs and 1 or more PIs. NRTIs currently approved are zidovudine (AZT), didanosine (ddI), zalcitabine (ddC), lamivudine (3TC), stavudine (d4T), and abacavir (ABC). All of these compounds act in a similar way, as chain terminators of the RT reaction after phosphorylation by intracellular kinases (Furman et al. 1986). NNRTIs in use are delavirdine (DLV), efavirenz (EFV) and nevirapine (NVP). They inhibit HIV-1 replication allosterically by displacing the catalytic aspartate residues relative to the polymerase-binding site (Tantillo et al. 1994). PIs are amprenavir (APV), indinavir (IDV), nelfinavir (NFV), ritonavir (RTV), saquinavir (SQV), and lopinavir/ritonavir. They do not require intracellular activation and strongly bind to the protease active site competing with the natural substrate and producing inactive non-infectious virions by preventing the cleavage of the viral polyproteins Gag and Gag-Pol precursors into structural proteins and viral enzymes (Kohl et al. 1998). Drug resistance has been found to be proportional to the number of mutations occurring by gene coding for RT (Richman et al. 1991). The clinical significance of the mutations that appear first (primary) versus those that appear later (secondary) remains debatable, particularly for NRTIs and NNRTIs. These mutations tend to arise in a specific order, at least in the case of AZT or RTV therapy. For higher levels of resistance to many antiretroviral drugs, 2 or more mutations are needed; mutation at codon T69S, followed by an insertion of 2 or more amino acids, is associated with resistance to multiple NRTIs. This in-sertion mutation is often accompanied by mutations at sites M41L, A62V, D67N, K70R, L210W, T215Y/F, K219Q/E (Winters et al. 1998). The multi-NRTI resistance related to the 151-complex is observed at codons A62V, V75I, F77L, F116Y, and Q151M (Schmit et al. 1998). Multi-NNRTI resistance is caused by accumulation of mutations at codons L100I, V106A, Y181C/I, G190S/A, M230L or by mutations occurring specifically at codons K103N or Y188L that can, each by itself substantially reduce the clinical utility of all currently approved drugs (Schmit et al. 1996). The distinction between primary and secondary mutations was kept for HIV-1 PIs because those that are listed as primary do have greater effects on drug susceptibility than those that are listed as secondary. PI resistance usually develops gradually from the ac-cumulation of multiple drug resistance mutations. Most substrate cleft mutations cause a 2 to 5-fold reduction in susceptibility in vitro to one or more PIs. Additional mutations in the enzyme flap and in other parts of the molecule are usually required for resistance to emerge in vivo. This requirement for multiple mutations to overcome the activity of PI has been referred to as a "genetic barrier" to drug resistance (Kempf et al. 2001). The L63P protease mutation is common in viruses that have never exposed to PIs (Kozal et al. 1996) and may be more prevalent in viruses from patients in whom a protease inhibitor-containing regimen has failed. Multi-PI resistance arises from accumulation of 4 or more of primary mutations M46I/L, V82A/F/T/S, I84V, L90M and secondary mutations L10F/I/R/V, I54V/M/L (Condra et al. 1995). Assays for drug resistance testing in HIV-1 infection are available detecting mutations that confer phenotypic resistance, either by genotyping all relevant codons or by hybridization-based detection of selected codons (Larder et al. 1991, Kozal et al. 1993). Interpretation of results can be done according to different guidelines, all of them based on appropriate criteria (Durant et al. 1999). HIV genotypic resistance determinations are of increasing diagnostic value in a number of clinical settings, including monitoring of drug resistance prior to therapy initiation or at the time of therapy failure (Hirsch et al. 2000). Information on patterns of resistance to and cross-resistance between antiretroviral agents may be important for decisions on how to combine drugs to achieve an optimum antiviral effect. Antiretroviral resistance studies are of special interest in HIV-infected infants as in addition to the drug pressure acting in the selection of viral mutants they may present vertically transmitted multidrug-resistant (MDR) isolates (Johnson et al. 2001). In this paper we report the results found in two groups of HIV-infected infants, treated and untreated with antiretroviral therapy, studied for the presence in RT and protease genes of antiretroviral resistance mutations. MATERIALS AND METHODS Subjects - Twenty-two vertically HIV-1 infected children aging from 4 months to 15 years old were included in this study. These children who are receiving follow-up care at the Department of Infectious Diseases, Instituto Fernandes Figueira (Fiocruz, Rio de Janeiro) were separated into 2 groups according to the administration of antiretroviral therapy or no therapy. In the first group were included those who presented disease symptoms, according to the US Centers for Disease Control and Prevention (CDC) 1994 classification. The antiretroviral-naïve group included those without symptoms. Entry criteria established HIV-1 viral load higher than 1 000 copies/ml of plasma. All of the patients were submitted to an informed consent obtained from their parents or guardians. The Ethics Committee of our Institute approved the study protocol. Methods - Plasma viral load was determined as described elsewhere using either the HIV-1 RNA PCR Assay (Amplicor Monitor Assay, Roche Molecular Systems, New Jersey, US) or the HIV-1 Nucleic Acid Sequence-Based Amplification (NASBA-QT, Advanced BioScience Laboratories, North Caroline, US). Nucleic acid extraction (Boom et al. 1990) - Briefly, HIV-1 RNA was extracted from plasma samples using lysis buffer (5 mol/ml guanidine thiocyanate, 0.1 M Tris-HCl, 0.2 M EDTA, 2.6 g/100 ml Triton X-100, pH 8.0) and it was bound to silicon dioxide particles, which were washed several times (120 g guanidine thiocyanate/100 ml 0.1 M Tris-HCl pH 6.4). The nucleic acid was eluted from the solid phase (10 mM Tris-HCl, 1 mM EDTA pH 8.0) and the extracted RNA was stored at -70ºC. cDNA synthesis and polymerase chain reaction (PCR) - The viral RNA was retrotranscribed into cDNA and subsequently amplified by a single-tube rt-PCR with an HIV-1 assay genotyping kit (TruGene, Visible Genetics Inc., Toronto, Canada). PCR cycles were as follows: 1 cycle 90ºC 2 min, 50ºC 60 min, 94ºC 2 min, 20 cycles 94ºC 30 s, 57ºC 30 s, 94ºC 2 min, 17 cycles 94ºC 30 s, 60ºC 30 s, 68ºC 2 min 30 s, 1 cycle 68ºC 7 min. A 1.3 kb amplicon covering the whole protease gene (codons 1-99) and the major part of the reverse transcriptase gene (codons 39-244) was amplified. Sequencing - Sequencing reactions were generated from the amplified cDNA by CLIPTM sequencing (Open-GeneTM, Visible Genetics Inc.) under thermal cycling (94ºC 5 min, 30 cycles 94ºC 20 s, 56ºC 20 s, 70ºC 1 min 30 s, 1 cycle 70ºC 5 min). It allows both directions of the cDNA to be sequenced simultaneously in the same tube using 2 different dye-labeled primers for each of the 4 sequencing reactions. Each sequencing reaction was loaded on an automated DNA sampler and run on 6% acrylamide gel electrophoresis (MicroGene Clipper, Visible Genetics Inc.). The assays were base called with GeneObjects (Visible Genetics Inc.), aligned and assembled together with GeneLibrarian (Visible Genetics Inc.). The sequences were compared to a database of wild type HIV-1 sequences to find out which mutations were present in the HIV-1 RNA. Classification of the mutations associated or not associated with decreased drug sensitivity was established according to the consensus statement on antiretroviral drug resistance testing (Hirsch et al. 2000). RESULTS The group receiving antiretroviral therapy included 12 HIV-infected children; 7 were female aging from 1 to 15 years old and 5 were male aging from 4 to 12 years old. The viral load ranged from 9800 to 480, 000 RNA copies/ml of plasma (3.99 to 5.68 log) (mean 112,442 copies; 5.05 log). CD4(+) T cells ranged from 54 to 2 276 cells/ml of blood. Epidemiological and laboratorial data and the period of time each child has been under antiretroviral treatment are shown in Table I. RT gene mutations were detected in 8 and were not detected in 2 of the 12 samples. The analysis of important resistance codons was not possible in the remaining 2 since only one amplicon strand 3' or 5' showed satisfactory results for all amplification and analysis procedures and the results could only be partially interpreted. RT gene mutation distribution in the group receiving therapy was as follows: T215Y: 6 children; M41L: 5 children; L210W: 4 children; E44D, M184V: 3 children; L74V, V75M, V118I, Y181C, G190S, H208Y: 2 children; T69D, A98G, V108I, V181C: 1 child. RT gene mutations detected in these patients are known to confer resistance or possible resistance to NRTIs and NNRTIs. Seven of the 12 patients presented resistance to NRTIs; among them 2 were also resistant to NNRTIs. The results are shown in Table II. Some of the elder children have been under treatment for a significant number of years. However, we could not find a correlation between the period of time and the number and variety of resistance mutations detected. PR gene mutations were detected in 9 of the 12 children receiving therapy and were not detected in 3. PR gene mutation distribution was as follows: M36I: 8 children; I54V: 5 children; L63P: 4 children; K20R, M36I, N88D: 3 children; L10I, L24I, D30N, M46L, L90M: 2 children; K20M: 1 child. Among these mutations those occurring at codons L10I, K20R, K20M, M36I and L63P were polymorphisms. Primary mutations were seen at codons D30N, M46I and V82A and secondary mutations at codons L24I, M46L, I54V and N88D. The L90M is considered to be a primary mutation to saquinavir and nelfinavir and a secondary mutation to indinavir, ritonavir, amprenavir and lopinavir/ritonavir. These mutations conferred resistance or possible resistance to PIs in 8 of the 12 patients. In the remaining 4 we found no evidence of resistance. The results are shown in Table III. In the second group 10 children without therapy were included. Six were female aging from 4 months to 6 years old. Four were male at ages of 3 months, 1 year old, 2 years old and 9 years old. The viral load ranged from 51,000 to 12,000,000 RNA copies/ml of plasma (4.70 to 7.08 log) (mean 2,404,500 copies; 6.38 log). CD4(+) T cells ranged from 26 to 1 514 cells/ml of blood (3 to 31%). Epidemiological and laboratorial data are shown in Table IV. A significant mean age difference was observed between both groups (7 years in the treated versus 2.9 years in the untreated children). It was very hard to include elder untreated children in this study, since the antiretroviral treatment to be offered to the HIV-infected children who are receiving follow-up care at the Instituto Fernandes Figueira, starts as soon after they have developed disease symptoms. Mutations in the protease gene occurring at codons K20M, M36I, L63P and A71V were reported in 6 children. These mutations are known to contribute to drug resistance, but are not by themselves associated to it as long as they occur as natural polymorphisms. For the RT gene a single resistance mutation (V108I) was reported in only one child conferring low-level resistance to NVP, DLV and EFV. There was no evidence of resistance to NRTIs in 8 samples and for the remaining 2 the results were only partially interpreted. These data are presented in Table V. DISCUSSION In the group receiving antiretroviral therapy, RT gene mutations were reported occurring at codons M41L, E44D, D67N, T69D, L74V, V75M, A98G, V108I, V118I, V181C, Y181C, M184V, G190S, H208Y, L210W, T215Y. Mutations at positions 41, 67, 70, 210, 215 and 219, named nucleotide excision mutations (NEMs), are associated with clinical resistance to not only AZT, but also to each of the other NRTIs, with the probable exception of 3TC (Wainberg & White 2001), conferring resistance throughout the pyrophosphorolysis and primer unblocking mechanism. The NEMs were reported in 7 of the 12 children, occurring at 1 or many resistance codons, and 1 child presented a single mutation (D67N) conferring probable resistance to AZT. The T215Y was the most frequent mutation observed in this group. It causes intermediate (10-20 fold) AZT resistance. Five children presented the M41L mutation, which causes possible resistance to AZT and d4T; its association to the T215Y mutation causes possible resistance or resistance to ABC (Hirsch et al. 2000). They also presented the D67N-mediated AZT possible resistance. Additional mutations occurring at relevant resistance codons such as L210W, observed in 4 children, resulted in multi-resistance to all of the NRTIs. The M184V mutation was reported in 3 children. It causes a resistance level higher than 100-fold to 3TC and emerges rapidly in patients receiving 3TC monotherapy (Wainberg et al. 1995). It is also selected during therapy with ABC (Miller et al. 2000) and less commonly with ddC and ddI (Winters et al. 1997) causing about 2-fold resistance to each of these 3 drugs. Two of the 3 children received a drug therapy that included 3TC and d4T. For the other child receiving AZT and 3TC some relevant resistance codons were missing from evaluation, thus hampering the final result interpretation. However, she also presented the T215Y-mediated AZT resistance, which is reversed by the M184V mutation (Tisdale et al. 1993). The T69D was detected in 1 child. It causes resistance to ddC (Fitzgibbon et al. 1992) and contributes to the NRTIs resistance when occurring together with NEMs (Winters et al. 2001). The L74V, reported in 2 children, occurs commonly during ddI and ABC monotherapy (Miller et al. 2000) and confers 2 to 5-fold resistance to ddI and ddC (Winters et al. 1997) and 2 to 3-fold resistance to ABC (Tisdale et al. 1997). Both children receiving ddI therapy were ddI, ddC and ABC resistant. The V75M mutation that appears to contribute to d4T resistance (Bloor et al. 1998) was reported in 1 child receiving d4T therapy. NNRTIs resistance mutations were reported in 2 of the 12 children. Both were receiving EFV therapy. The Y181C and G190S mutations were reported in 1 child and the other one presented additional resistance mutations at sites A98G and V108I. The Y181C mutation causes a more than 30-fold resistance to NVP and DLV and 2 to 3-fold resistance to EFV (Petropoulos et al. 2000). The G190S mutation causes high-level resistance to both NVP and EFV (Huang et al. 2000). A98G and V108I cause low-level resistance to each of the NNRTIs (Hirsch et al. 2000). PIs resistance mutations were not seen in 3 of the 12 children. In the remaining 9 they occurred at codons L10I, K20M, K20R, L24I, D30, M36I, M46I, M46L, I54V, L63P, V82A, N88D, L90M. Amino acid variants at positions 10, 20, 36 and 63, observed in this study, and those at codons 71, 77 and 93 occur at polymorphic sites making frequent contributions to drug resistance when present together with other protease mutations (Nijhuis et al. 1999). PIs primary mutations were reported at codons D30N, M46I, and V82A. The L90M mutation either contributes to or directly confers resistance to each of the 6 approved PIs, acting as secondary mutation to IDV, RTV, LPV and APV and primary mutation to SQV and NFV (Dronda et al. 2001). The D30N mutation, reported in 2 children, occurs solely in patients receiving NFV and does not confer in vitro cross resistance to the other PIs (Zolopa et al. 1999). Cross-resistance to IDV, RTV and SQV has been observed among isolates presenting this mutation together with other at positions 88 and 90 (Parkin et al. 2001). This pattern was partially observed in both children: 1 child receiving NFV and also presenting the N88D mutation showed resistance to all of the PIs except for SQV. The other one showing the 2 additional resistance mutations and resistance to IDV, RTV, SQV, and NFV was receiving treatment with IDV. The M46I mutation was reported in 3 children. Mutations at position 46 contribute resistance to each of the PIs except possibly SQV and have been commonly reported during therapy with IDV, RTV, APV, and NFV (Condra et al. 2000a). Two of the 3 children presented resistance to all of the PIs including SQV and they were receiving RTV or NFV. The third child receiving treatment with NFV did not show resistance to SQV and LPV associated to RTV. The V82A mutation was the most frequently primary mutation observed in this group of children. It was detected in 5 of the 9 samples showing PIs resistance mutations. The V82A occurs predominantly in HIV-1 isolates from patients receiving treatment with IDV or RTV (Condra et al. 1996, Molla et al. 1996). By themselves, mutations at position 82 confer reduced susceptibility in vitro to IDV, RTV, and LPV but not to NFV, SQV, or APV (Kempf et al. 2001). However, when present with other PI mutations, V82A contributes to clinical resistance to each of the PIs. The 5 children presenting this mutation showed resistance or possible resistance to all of the PIs. Three were receiving RTV treatment and 2 were receiving NFV. The L90M mutation, reported in 2 children, has been reported in isolates from patients receiving SQV, NFV, IDV, and RTV. This mutation either contributes to or directly confers resistance to each of the PIs playing important role in causing cross-resistance to each of them (Dronda et al. 2001). One child receiving treatment with RTV showed possible resistance to LPV associated to RTV and resistance to the remaining PIs. For the other child receiving treatment with IDV it was reported possible resistance to IDV and RTV and resistance to SQV and NFV. PIs secondary mutations were reported at codons L24I, M46L, I54V, and N88D. The I54V reported in 5 children contributes resistance to each of the 6 approved PIs and has been commonly reported during therapy with IDV, RTV, APV, SQV, and LPV (Condra et al. 2000b). Three of these children were receiving RTV. The N88D was reported in 3 children; it commonly occurs in patients receiving NFV and occasionally in patients receiving IDV. By itself, it causes low-level resistance to NFV and IDV. However, in the presence of D30N or M46I it causes high-level NFV resistance (Petropoulos et al. 2000) as reported in 1 child. The M46L was reported in 2 children; it contributes resistance to each of the PIs except possibly SQV and has been commonly reported during therapy with IDV, RTV, APV, and NFV (Condra et al. 2000b). One child was receiving RTV and was resistant or partially resistant to all of the PIs; the other one with possible resistance to IDV, RTV, and APV was receiving NFV. The L24I mutation reported in 2 children has been reported only in HIV-1 isolates from patients receiving IDV (Condra et al. 2000a) and has not been shown to confer cross-resistance to other PIs, except possibly LPV (Kempf et al. 2001). Both children were receiving NFV or RTV and presented possible resistance to LPV. However, the L24I mutation could not be correlated to drug resistance since both children presented primary M46I and V82A mutations conferring resistance to LPV. In the group of untreated patients we evaluated 10 HIV-infected children. Eight of them did not have NRTIs resistance mutations and in the remaining 2 the results were only partially interpreted since the analysis of important resistance codons was not possible. The V108I mutation reported for 1 child conferred low-level resistance to NVP, DLV and EFV (Huang et al. 1999). The antiretroviral therapy to be offered to this child should take into account these results. PR gene mutations at positions 10, 20, 36, and 71 occur in about 6% of untreated persons infected with subtype B viruses and the mutation at position 63 is the most polymorphic protease position occurring in 62% of untreated persons (Pieniazek et al. 2000). PIs resistance mutations were detected in 6 of the 10 untreated patients. However, all of them occurred at polymorphism sites (K20M, M36I, L63P, A71V) so they did not confer resistance to PIs. These patients should be considered with regard to the development of additional mutations associated with drug resistance. The data presented in this work reported the presence of viral variants at both groups of children. However, the frequency and the level of drug resistance mutations were more evident in the group receiving antiretroviral therapy, which corroborates the concept of selective pressure acting effectively in the emergence of resistant viral strains. Few data have been published on HIV-1 genotyping in vertically infected children. Therefore, the value of genotypic assays in guiding treatment has not been established as yet. However, they should be done in drug failure cases while the pediatric patient is still receiving antiretroviral therapy. ACKNOWLEDGEMENTS To Visible Genetics Inc., Toronto, Canada. REFERENCES
Copyright 2003 Instituto Oswaldo Cruz - Fiocruz. Free, full-text also available from http://www.memorias.ioc.fiocruz.br The following images related to this document are available:Photo images[oc03167t1.jpg] [oc03167t3.jpg] [oc03167t5.jpg] [oc03167t4.jpg] [oc03167t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}