 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
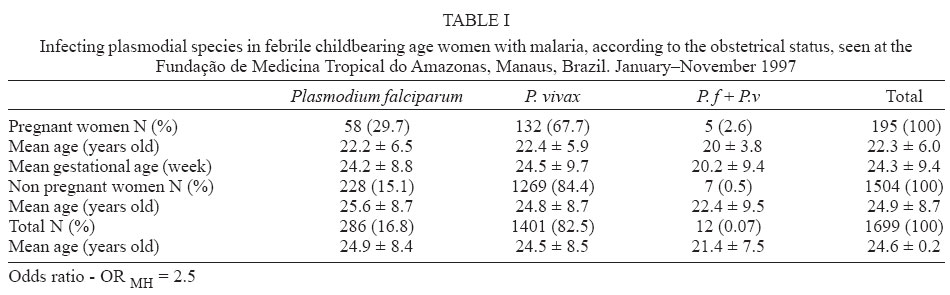
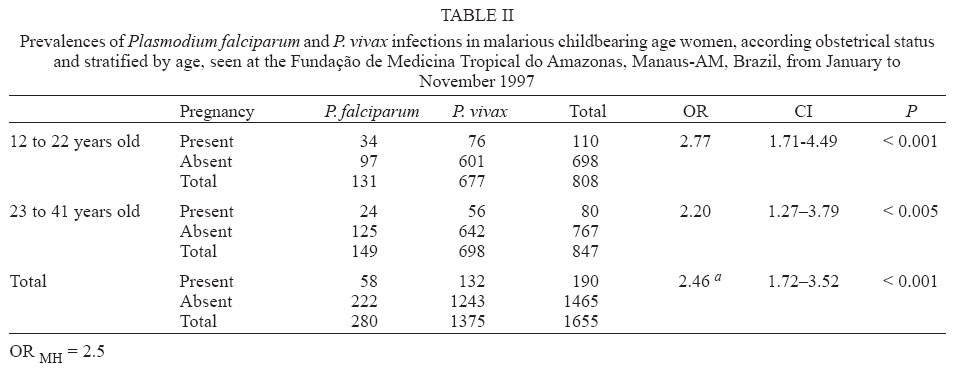
Mem Inst Oswaldo Cruz, Rio de Janeiro, Vol. 99, No. 1, Feb, 2004, pp. 19-21 Malaria during Pregnancy in a Reference Centre from the Brazilian Amazon: Unexpected Increase in the Frequency of Plasmodium falciparum Infections Flor Ernestina Martínez-Espinosa/*/**, Cláudio Tadeu Daniel-Ribeiro/+, Wilson Duarte Alecrim*/** Departamento de Imunologia, WHO Collaborating Centre for Research and Training in Immunology of Parasitic Diseases, Instituto Oswaldo Cruz-Fiocruz, Av. Brasil 4365, 21045-900 Rio de Janeiro, RJ, Brasil *Fundação de Medicina Tropical do Amazonas, Manaus, AM, Brasil **Centro Universitário Nilton Lins, Manaus, AM, Brasil Received 15 September 2003 Code Number: oc04003 ABSTRACT Malaria remains globally the most important parasitic disease of man. Data on its deleterious effects during pregnancy have been extensively documented in hyperendemic, holoendemic, and mesoendemic areas from Africa and Asia where Plasmodium falciparum is responsible for almost all infections. However, knowledge about malaria during pregnancy in areas where transmission is unstable and P. vivax is the most prevalent species, such as the Brazilian Amazon, is scarce. Here, we report a preliminary cross sectional descriptive study, carried out at the Fundação de Medicina Tropical do Amazonas, a reference centre for diagnosis and treatment of tropical diseases in the west-Amazon (Manaus, Brazil). A total of 1699 febrile childbearing age women had positive thick blood smears to Plasmodium species, between January and November 1997: 1401 (82.5%) were positive for P. vivax, 286 (16.8%) for P. falciparum and 12 (0.07%) carried mixed infections. From the malarious patients, 195 were pregnant. The ratio of P. falciparum to P. vivax infections in the group of non-pregnant infected women was 1:5.6 while it was 1:2.3 in that of pregnant infected ones. Similar rates or even proportionally more vivax infections during pregnancy were expected to occur, in function of the contraindication of primaquine with the resulting increased P. vivax relapse rates. Such an observation suggests that the mechanism of resistance/susceptibility to infection and/or malaria pathogenesis in pregnant women may differ according to Plasmodium species and that the extensively described increase in the frequencies of malaria infection during pregnancy may be specifically due to P. falciparum infection. Key words: malaria - pregnancy - Plasmodium falciparum - Plasmodium vivax - unstable transmission - Brazilian Amazon - South America Pregnancy is accompanied by physiological and immunological changes, which modify both resistance to infections and disease pathogenesis. On the other hand, malaria infection may represent a dangerous threat to the course of the pregnancy. The endemic context is a powerful determinant in both senses of the malaria/pregnancy interplay. In unstable transmission areas, where malaria is predominantly epidemic or of low endemicity and undergoes seasonal influence, malaria is almost always symptomatic and affects people of all age with increased rates of severe disease, abortion, foetal death, and premature delivery of infants in pregnant women. The effects of malarial infections in adulthood are much less marked in highly endemic areas, where women, through repeated prior infections, have acquired substantial protective immunity against the disease (McGregor et al. 1983, Brabin 1983, Menendez 1995). It is generally agreed that the prevalence of falciparum malaria in highly endemic areas is higher among pregnant women than in other groups (Brabin 1983, McGregor 1984, Menendez 1995). However, the most important studies considering the relationship between malaria infection and pregnancy have been carried out in African and Asian hyperendemic (Brabin 1983, McGregor 1984, Mutabingwa 1994), holoendemic (Brabin 1983, McGregor 1983, Mutabingwa 1994, Diagne et al. 1997), and mesoendemic (Nosten et al. 1991) regions where Plasmodium falciparum is responsible for the majority of infections. In addition, until now, none of the available studies has specifically concerned the susceptibility of pregnant women to different Plasmodium species. The present study, carried out at the Fundação de Medicina Tropical do Amazonas (FMT-AM), describes observations made in malaria infected pregnant women from South America where infections by P. vivax predominate. PATIENTS AND METHODS The malaria transmission risk of a given area is usually estimated in Brazil by determining the annual number of malaria cases per 1000 inhabitants (annual parasite incidence or API). Areas can be classified accordingly as high (more than 50 cases), medium (between 10 and 50), low (less than 10) or no (zero) risk. Manaus is located in an area of unstable transmission in the west Brazilian Amazon with a PIA of 18.3 in 1997. In that year there were 21,234 malaria cases in the municipality, 83% of them caused by P. vivax. The Fundação Nacional de Saúde (Funasa) reported that from 1989 to 1996 P. vivax was responsible for 81% and P. falciparum for 17.1% of the registered cases of malaria infection from rural and urban regions, with a ratio of P. falciparum to P. vivax infection ranging from 1:3.1 (in 1993) to 1:12.0 (in 1991). A descriptive cross-sectional study of malaria during pregnancy was carried out from March to November 1997 at the FMT-AM. Although malaria diagnosis and treatment can be obtained in other small health centres, FMT-AM is the reference centre for diagnosis and treatment of malaria and other tropical diseases in the state. In this period, 10,483 cases of malaria, nearly 50% of the total registered cases of the county, were diagnosed and treated there. Malaria was defined by the presence of Plasmodium parasites in the peripheral thick blood smear of febrile patients. All pregnant women attending to the Hospital spontaneously for the malaria episode were asked to enrol in the study, at the moment of diagnosis, and were followed-up daily during acute infection and at least once monthly from treatment until delivery. The Funasa determines treatment with chloroquine (25 mg/kg, but no more than 1 g of total dose) to vivax malaria and quinine- first choice- (30 mg/kg/day for 7 days for 3 days associated to another drug such as clindamicine) or mefloquine- second choice, after the first trimester of pregnancy -(15 mg/kg, but no more than 1 g of total dose) to falciparum infections. RESULTS During the nine months of follow-up, 1699 women between 12 and 41 years of age were diagnosed with malaria infection; 195 (11.7%) of them were pregnant. The mean age was 24.9 ± 8.7 years old among non-pregnant women and 22.3 ± 6.0 among the pregnant ones (p < 0.005) that presented a mean gestational age of 24.3 ± 9.4 weeks at the moment of diagnosis. No statistically significant difference was observed in the gestational age, when the infecting species was considered (Table I). There were 1269 (84.4%) cases of P. vivax, and 228 (15.1%) of P. falciparum infection among non-pregnant women. In the pregnant women group, the percentages found were considerably different, being 132 (67.7%) for P. vivax and 58 (29.7%) for P. falciparum; the mixed infections corresponding to 7 (0.5%) and 5 (2.6%) respectively (Table I). The symptoms at the time of assessment did not differ between patients with different infecting species. The earliest and most frequent clinical manifestations were fever, headache, and rigors in all patients. Although a significant association was observed between age and pregnancy [OR = 1.51; CI = (1.10 < OR < 4.49)]; there was no statistically significant difference on age between P. vivax and P. falciparum-infected women [OR = 0.91; CI = (0.69 < OR < 1.18)]; P > 0.1. Taking age into account, the risk of presenting P. falciparum infection, if pregnant, in malaria-infected women was 2.5 higher than if not pregnant (Table II). DISCUSSION P. vivax is the most important malaria species associated to infection in the Amazon region. This contrasts with the situation in regions of Africa or Asia where previous studies on malaria during pregnancy have been performed, and where nearly all-significant malarial cases are due to P. falciparum. Although we do not have sufficient information on malaria during pregnancy in South Ameri-ca, severe disease is probably not as frequent when compared to African and Asian endemic regions, because P. vivax rarely leads to life-threatening complications or mortality. In addition, the present Brazilian government policy on malaria control includes early diagnosis and treatment of cases. In previous studies it has been reported that pregnant women have increased risk of falciparum malaria and severe disease. The main factors associated to an increased susceptibility to malaria infections during pregnancy relate to diminished cellular immunity (Weinberg 1984, Wegmann et al. 1993, Smith 1996) and the presence of the placenta, a privileged site for parasite multiplication (Bray & Sinden 1979, McGregor et al. 1983, Moshi et al. 1995, Leopardi et al. 1996, Fried & Duffy 1996, Rogerson & Beeson 1999). It is also possible, as claimed by Lindsay et al. (2000) that pregnant women are more attractive to mosquitoes. It is, however, not yet known if the increased susceptibility to malaria is inclusive of all Plasmodium species or specifically to P. falciparum, since most of these studies have been conducted in areas where this species is the most prevalent. The data presented here indicate that, although P. vivax infection is more frequent than the P. falciparum one, both in the general population and among pregnant women of the studied region, the odds for having P. falciparum infection seems to be higher in pregnant than in non-pregnant women. This suggests, as we have hypothesized earlier (Martínez-Espinosa 1998, Martínez-Espinosa et al. 2000), that pregnant women are more susceptible to P. falciparum. This could result from a reduced ability of pregnant women to control P. falciparum parasitaemia, the presence of specific receptors for P. falciparum infected red blood cells (chondroitin sulphate A-CSA)- which is abundant on the surface of trophoblastic villi in the placenta (Fried & Duffy 1996, Rogerson & Beeson 1999) and could favour the preferential development of the parasite once in the host and even from the facilitation of P. falciparum infection (as a result of the postulated increased attractiveness of P. falciparum infected mosquitoes, Martínez-Espinosa et al. 2000). Although our data do not exclude the possibility that pregnant woman have an increased resistance to other non-falciparum species, a prospective follow up study of around 6400 women in childbearing age in an Amazonian endemic region, conducted and presently under analysis by our group, seems to rule out this possibility. REFERENCES
Copyright 2004 Instituto Oswaldo Cruz - Fiocruz. Free, full-text also available from http://www.memorias.ioc.fiocruz.br The following images related to this document are available:Photo images[oc04003t2.jpg] [oc04003t1.jpg] |
| |||||||||

{kind=link}
{kind=link}