 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Mem Inst Oswaldo Cruz, Rio de Janeiro, Vol. 99, No. 3, May, 2004, pp. 281-282 SHORT COMMUNICATION Prevalence of Human Papillomavirus Type 16 Variants in the Federal District, Central Brazil Márcio R Cruz/++, Daniela M Cerqueira, Waldenor B Cruz, Geni NL Camara*, Marcelo M Brígido, Evandro O Silva**, Luciano GS Carvalho***, Cláudia RF Martins/+ Instituto de Biologia,
Universidade de Brasília, ICC Sul, 70919-900 Brasília, DF,
Brasil *Agência de Vigilância Sanitária, Ministério
da Saúde, Brasília, DF, Brasil **Hospital Regional da Ceilândia,
Ceilândia, DF, Brasil ***Hospital de Base do Distrito Federal, Brasília,
DF, Brasil Financial support: Fundação de Apoio à Pesquisa do Distrito Federal and Fundação de Empreendimentos Científicos e Tecnológicos Received 3 November
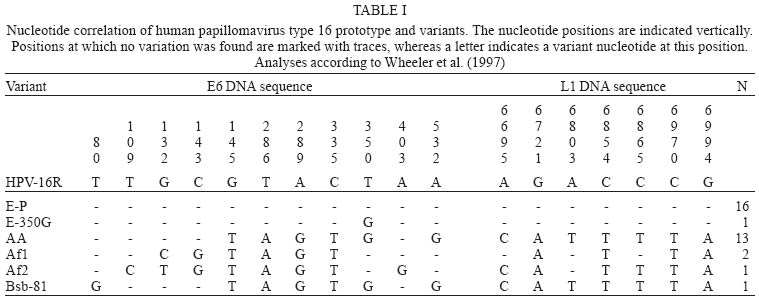
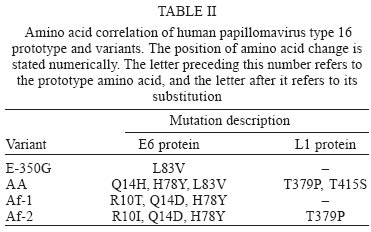
2003 Code Number: oc04050 We report the prevalence of human papillomavirus type 16 (HPV-16) variants in women with cervical lesions from the Federal District, Central Brazil. We analyzed 34 HPV-16 samples, identifying the sequence variations of E6 and L1 genes and correlating variant frequency with disease status. The most prevalent HPV-16 variant was the European (50%), followed by Asian-American (41.2%), African-1 (5.9%), and African-2 (2.9%). European and non-European variants appeared in equal frequencies among the cytological types of lesions atypical squamous or glandular cells of undetermined significance, cytological alterations suggesting HPV infection, cervical intraepithelial neoplasias, squamous cell carcinoma, and adenocarcinoma. Key words: human papillomavirus type 16 - variants - Federal District, Brazil Human papillomaviruses (HPVs) have been consistently associated with invasive cervical carcinoma (ICC) and cervical intraepithelial neoplasias (CINs) (Lehtinen et al. 2001, Matsukura & Sugaset 2001). Worldwide, HPV-16 is considered the most prevalent of the more than 20 different HPV types associated with cervical lesions (Bosch et al. 1995). Within an HPV type, variants are defined by nucleotide substitutions of up to 2% in E6 and L1 genes and by up to 5% in the LCR (Chan et al. 1995). HPV-16 variants can be clustered in 5 groups: African-1, African-2, Asian, Asian-American, and European (Stewart et al. 1996, Yamada et al. 1997). The sequence considered to be the reference, mentioned as the prototype (Seedorf et al. 1985), belongs to the European branch. The purpose of the present study is to describe the prevalence of HPV-16 variants in cervical specimens from the Federal District, Central Brazil, as well as to investigate a possible differential variant associated pathogenicity in this population. Thirty four HPV-16 variants were identified by polymerase chain reaction (PCR) amplification and automated sequencing of the MY09/MY11 (Bernard et al. 1994) L1 region and the entire E6 gene, amplified by primers E6A/E6S (Gibco) (Wheeler et al. 1997). The same primers were used for automatically sequencing the 2 strands of the amplified products using a Megabace System (Amersham Pharmacia). The base positions of all sequences obtained were numbered after basic local alignment search tool (BLAST) analysis (Altschul et al. 1997), and the variant designation followed the classification of Wheeler et al. (1997). The most prevalent HPV-16 variant was the European (17 out of 34, 50%), followed by the Asian-American (14 out of 34, 41.2%), African-1 (2 out of 34, 5.9%), and African-2 (1 out of 34, 2.9%). Only one of the European variants was an E-350G variant. HPV-16 non-European and European variants were detected at similar frequencies among the cytological types of lesions, revealing an uniform distribution (Table I). We identified one nucleotide substitution in an Asian-American variant (Bsb-81) that had not been reported previously by other authors. It occurred at position 80 (thymine to guanine) (Table I), between a TATA signal (from nucleotide 65 to 71) and the beginning of the E6 coding region (from nucleotide 83 to 559). Considering all variants, 12 different point mutations were detected within the E6 segment, spanning nucleotides 31 and 683. Seven different point mutations were detected within the L1 segment, spanning nucleotides 6584 and 7035 (Table I). Altogether, 8 point mutations in 7 nucleotide positions generated amino acid changes in E6 and in L1 proteins (Table II). In Brazil, similar to the prevalence of HPV-16 European variants in the Federal District (50%), Villa et al. (2000) detected European variants in 54% of the patients in São Paulo. However, in our study, the percentage of patients positive for Asian-American variants (41.2%) was higher than that reported by other authors. Villa et al. (2000) detected Asian-American variants in 22% of the patients and Yamada et al. (1997), in an international study, detected Asian-American variants in 19.7% of the patients living in Central and South America. Our results suggest that HPV-16 non-European variants do not represent an additional factor associated with increased occurrence of high grade cervical lesions in the studied population, as European and non-European variants appeared in equal frequencies among the cytological types of lesions. Nindl et al. (1999) also did not find any correlation between variants and severity of the lesion. ACKNOWLEDGEMENTS To John Penney, for reviewing this manuscript. REFERENCES
Copyright 2004 Instituto Oswaldo Cruz - Fiocruz. The following images related to this document are available:Photo images[oc04050t2.jpg] [oc04050t1.jpg] |
| |||||||||

{kind=link}
{kind=link}