 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Mem Inst Oswaldo Cruz, Rio de Janeiro, Vol. 99, No. 3, May, 2004, pp. 319-324 Survey of Antimicrobial Susceptibility Patterns of the Bacteria of the Bacteroides fragilis Group Isolated from the Intestinal Tract of Children Viviane Nakano++, Mario Julio Avila-Campos+ Laboratório
de Anaeróbios, Departamento de Microbiologia, Instituto de Ciências
Biomédicas II, Universidade de São Paulo, Avenida Professor
Lineu Prestes 1374 - 2º andar, 05508-900 São Paulo, SP, Brasil Financial support: Fundação de Amparo à Pesquisa do Estado de São Paulo, grant 99/06475-1 Received 23 October
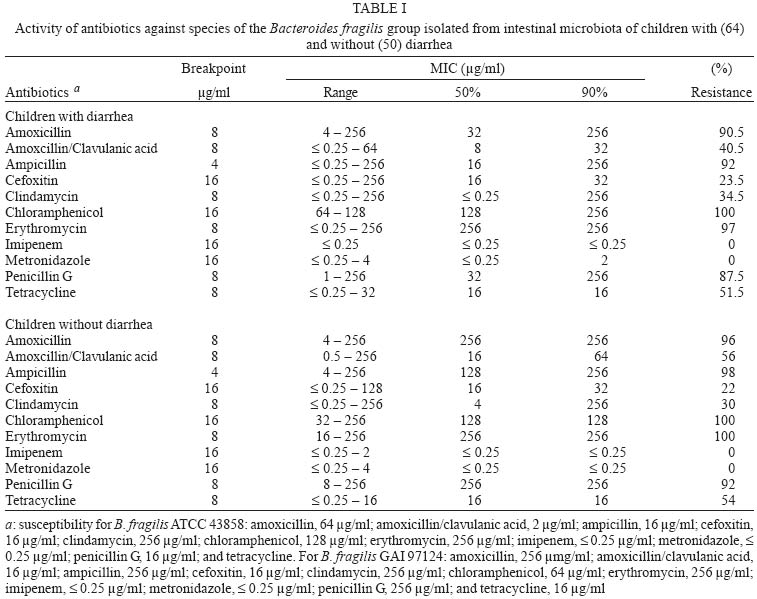
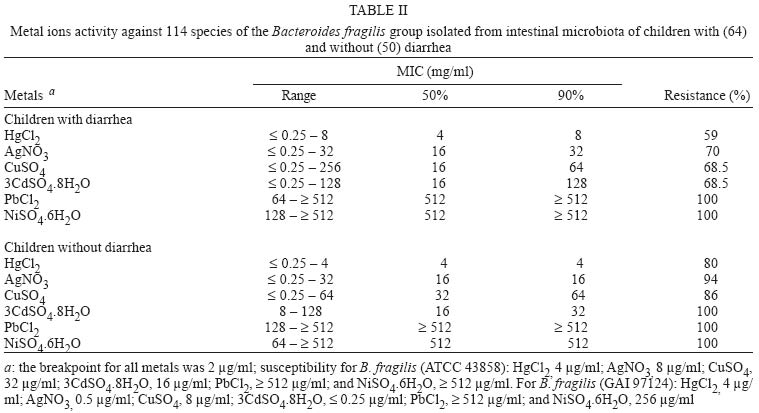
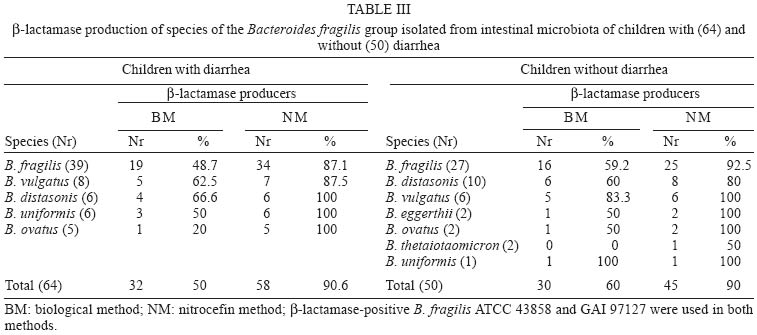
2003 Code Number: oc04057 The bacteria of the Bacteroides fragilis group are considered important clinical pathogens and they are the most common anaerobes isolated from human endogenous infections. In this study, the susceptibility patterns to antibiotics and metals of 114 species of the B. fragilis group isolated from children with and without diarrhea were determined. Susceptibility was assayed by using an agar dilution method with Wilkins-Chalgren agar. All B. fragilis strains were resistant to lead and nickel, but susceptible to metronidazole and imipenem. b-lactamase production was detected by using biological and nitrocefin methods, respectively, in 50% and 90.6% of the isolates of children with diarrhea and in 60% and 90% of the isolates of children without diarrhea. Our results show an increase of antibiotics and metals resistance in this microbial group, and a periodic evaluation of the antimicrobial susceptibility is needed. In Brazil, the contamination for antibiotics or metal ions is often observed, and it is suggested an increase the antimicrobial resistance surveillance of this microbial group, mainly those isolated from children's diarrhea. Key words: Bacteroides fragilis species - antimicrobial susceptibility - b-lactamase enzyme Bacteroides fragilis is considered an important clinical pathogen and it is the most common anaerobe isolated from human clinical specimens producing endogenous infections (Duerden 1994). Species of the B. fragilis group have shown an increase of the resistance to most of the antimicrobial agents traditionally used for treating anaerobic infections. Antibiotics and metal ions have been used in the treatment of these infections but it has been a complicated process because of the bacterial resistance to these drugs, particularly in B. fragilis species (Salyers 1984). It is well known that antimicrobial drugs can produce alterations on host's indigenous microbiota selecting resistant organisms, which can appear as opportunistic pathogens (Bezirtzoglou 1997). B. fragilis group bacteria have been studied because of their pathogenic potential and because of their unusual multiple resistances to several antibiotics (Bartlett et al. 1983) and heavy metals (Salyers 1984, Avila-Campos et al. 1991), which can be either transferred to intra- and inter-species or to other intestinal bacteria, including gram-negative facultative anaerobic ones, e.g. Escherichia coli (Tally et al. 1979). In facultative organisms, the heavy metal resistance is plasmid-mediated and it has been extensively studied. In these organisms, the resistance markers to metals such as mercury and arsenic are usual on plasmids carrying multiple antibiotic resistance genes (Nakahara et al. 1977). Moreover, these genetic markers have been observed among species of the human indigenous amphibiotic microbiota as well as in clinical isolates (Welch et al. 1979). Several studies have demonstrated that transferable plasmids in Bacteroides spp. play an important role in the dissemination of resistance to antibiotics, but their resistance to heavy metals is rarely reported in the literature (Riley & Mee 1982, Rudrik et al. 1985). The emergence and the increase of resistance to some antimicrobial agents, including tetracycline, clindamycin, cefoxitin, and metallic ions, reflect the capacity of the B. fragilis group in developing resistance via different mechanisms. In developing countries, self-prescription and the use of over-the-counter antimicrobials is very common (Kunin 1993), which may lead to the emergence of a bacterial resistance in the indigenous intestinal anaerobic microbiota (Wexler et al. 2001). Thus, it is necessary to carry out a continuing assessment to the activity of antimicrobial agents against these bacteria and search for new efficacious antibiotics. The National Committee for Clinical Laboratory Standards (NCCLS) has recommended to be performed a periodic evaluation of the susceptibility patterns of anaerobes producing infections, particularly species of the B. fragilis group, in order to provide more information to physicians about the treatment of infectious processes. In this study, the antimicrobial susceptibility patterns of the bacteria of the B. fragilis group isolated from children's intestinal microbiota was determined. MATERIALS AND METHODS Bacteria - Bacteria were obtained from diarrhea stool samples collected from two child hospitals in São Paulo (Hospital Menino Jesus and Instituto da Criança do Hospital das Clínicas) and from healthy children from two state day care centers (Maria do Belém and Vila Carmosina, SP), from April to December 2000. None of the children received antibiotic therapy before the sample collection. A total of 114 species of the B. fragilis group was tested: 64 strains isolated from 15 children with diarrhea, and 50 strains from 24 children without diarrhea, both groups ranged from 2 months to 6 years old. Bacteria were plated onto B. fragilis-bile-esculin agar and identified by established methodology (Holdeman et al. 1977). All the isolates were stored in 10% skim-milk at _80oC at the Anaerobe Laboratory, Department of Microbiology until the susceptibility tests could be done. The Ethic Commission of the hospitals and of the Institute of Biomedical Sciences of the University of São Paulo approved this study. Antibiotics and metal ions susceptibility testing - The antibiotics used were the following: amoxicillin, ampicillin, clindamycin, erythromycin, and tetracycline (Luper Ind. Farm. Ltd., São Paulo, SP, Brazil); amoxicillin/clavulanic acid (Smithkline Beecham Brazil Ltd., SP); cefoxitin and imipenem (Merck, Sharp & Dohme, SP); penicillin G (Prodoti Lab. Farm. Ltd., SP), and metronidazole (Aventis Farm. Ltd., SP). The metals used were the following: mercuric chloride (HgCl2), silver nitrate (AgNO3), copper sulfate (CuSO4) and nickel sulfate (NiSO46H2O) (Labsynth Prod. Lab. Ltd., SP); cadmium sulfate (3CdSO4.8H2O) and lead chloride (PbCl2) (Vetec Química Fina Ltd., SP). Antimicrobial susceptibility tests were performed by using an agar dilution method according to NCCLS (1997) using the Wilkins-Chalgren agar. Plates containing two-fold serial dilutions of antimicrobial agents ranging from 0.25 to 512 µg/ml were used, and the final inoculum delivered by a Steers replicator was 1.5 x 105 cfu/spot. Plates without antibiotics or metals were used as controls. All the plates were incubated in anaerobiosis (90% N2/10% CO2), at 37°C, for 48 h. The minimal inhibitory concentration (MIC) was defined as being the lowest concentration of each antimicrobial agent able to inhibit the macroscopic bacterial growth or any distinct change from the growth control. Reference strains B. fragilis ATCC 43858 and GAI 97124 were included in each experiment to assess the reliability of the method. Moreover, all the tests were done in duplicate. Determination of b-lactamase activity - Penicillin-resistant strains were tested to verify the b-lactamase production by using biological (Paula et al. 2003) and nitrocefin methods. The biological method was as it follows: 20 µl of a bacterial growth was inoculated, in duplicate, onto BHI agar containing 32 µg/ml of penicillin. After incubation (anaerobiosis, 37ºC, 48 h), the growth was exposed to chloroform vapors during 20 min. Then, 3 ml of BHI (0.7% agar) inoculated with Actinomyces viscosus ATCC 910144 susceptible to penicillin (£ 0.25 µg/ml) was pour-plated. Plates were incubated in anaerobic conditions, at 37ºC, for 72 h, and the presence of a growth halo over killed bacteria was considered as producing b-lactamase. The hydrolysis of the chromogenic cephalosporin, nitrocefin (Oxoid Ltd., SP) was used as well. Briefly, a drop of nitrocefin was deposited on a microscope slide and a colony was dissolved on it. Then, the mixture was incubated at room temperature for 30 min. The b-lactamase activity was expressed as it follows: negative, no color alterations, and positive, red colored. In both methods a penicillin-resistant and a b-lactamase-positive B. fragilis ATCC 43858 and GAI 97124 were used. RESULTS Analyzed isolates - From the 114 analyzed species of the B. fragilis group (64 strains from diarrhea and 50 from normal stools), B. fragilis ranked first, being recovered in 60% and in 54%, respectively. Among species isolated from children with diarrhea B. vulgatus was recovered in 12.5%, followed by B. uniformis and B. distasonis (9.3%) and B. ovatus (3.1%). Among species isolated from children without diarrhea B. distasonis was recovered in 20%, B. vulgatus (12%), B. eggerthii, B. ovatus, and B. thetaio-taomicron (4%), and B. uniformis (2%). Antimicrobial susceptibilities - MIC values as well as the resistance rates to antibiotics and metal ions of species of the B. fragilis group isolated from children with and without diarrhea are expressed in Tables I and II, respectively. Isolates were uniformly susceptible to imipenem and metronidazole. Species isolated from children with and without diarrhea showed the following resistance rates, respectively: amoxicillin, 90.5% and 96%; ampicillin, 92% and 98%; cefoxitin, 23.5% and 22%; clindamycin, 34.5% and 30%; erythromycin, 97% and 100%; penicillin G, 87.5% and 92%; and tetracycline, 51.5% and 54%. The association amoxicillin/clavulanic acid showed a middle activity with resistance rates of 40.5% and 56%, respectively, in species of the B. fragilis group isolated from children with and without diarrhea. In all tested metal ions, the resistance rates for isolates of the B. fragilis group in both groups ranged from 59% to 100% (Table II). Mercuric chloride showed a better activity than other ions, showing MIC90 < 8 µg/ml and MIC90 < 4 µg/ml, respectively, for isolates from children with and without diarrhea. The isolates from both children groups showed, respectively, resistance rates of 59% and 80% to mercuric chloride (HgCl2); 70% and 94% to silver nitrate (AgNO3); 68.5% and 86% to copper sulfate (CuSO4); 68.5% and 100% to cadmium sulfate (3CdSO4.8H2O). A high resistance rate of 100% was observed to lead chloride (PbCl2) and to nickel sulfate (NiSO4.6H2O). Detection of b-lactamase - Most of b-lactamase producing isolates from both children's groups could be detected by using both biological and nitrocefin methods (Table III). The b-lactamase activity through biological methods was confirmed in 32 (50%) of the 64 tested isolates tested from children with diarrhea and in 30 (60%) of the 50 isolates from healthy children. Moreover, this enzyme was detected for nitrocefin in 58 (90.6%) of the 64 isolates from children with diarrhea and in 45 (90%) of the 50 isolates from healthy children. It was observed differences in the detection of the b-lactamase production when both methods were used. Nitrocefin method was more sensible to detect the b-lactamase activity. However, all the b-lactamase-positive strains of the B. fragilis group were considered high producers in spite of their phenotype resistance. DISCUSSION Species of the B. fragilis group are the anaerobic bacteria most commonly associated with a wide variety of endogenous clinical infections, especially B. fragilis species. These organisms represent 75% of post-operative intra-abdominal infections and approximately 100% in cases of appendicitis (Aldridge et al. 2001). In this study, the survey of antibiotics and metals susceptibility as well as the resistance profile of species of the B. fragilis isolated from children intestinal microbiota was performed. Clindamycin resistance among clinical isolates of Bacteroides has increased in several countries. However, in Europe and in the US, the clindamycin (Aldridge et al. 2001, Wexler et al. 2001) resistance is below 22% compared with 35% in Brazil, Japan, and Spain (Almeida & Uzeda, 1987, Baquero & Reig, 1992, Bandoh et al. 1993). Similar resistance rate is mentioned to cephalosporin in Canada and France (Bourgault et al. 1992, Dubreuil et al. 1992). In this study, B. fragilis strains isolated from children without diarrhea showed a similar resistance to several antimicrobials with that ones isolated from diarrhea (Table I). All the strains from both groups were 100% resistant to lead and nickel. The high resistance observed to antibiotics and metals in Bacteroides species can be explained because the self-medication is common in countries such as Brazil, where policies about medication are not strict. Moreover, all tested organisms were susceptible to imipenem and metronidazole, according to literature (Mol et al. 1991, Aldridge et al. 2001, Wexler et al. 2001). On the other hand, antimicrobial resistance has been associated with plasmids, except for metronidazole (Breuil et al. 1989) and imipenem (Bandoh et al. 1992), and conjugative transposon such as Tn 4555 have been recently described to be associated with cefoxitin resistance, encoding the cfxA gene (Tribble et al. 1999). During the last 20 years, species of the B. fragilis group have shown an increase of the resistance to most of the antimicrobial agents traditionally used for treating anaerobic infections (Sanders & Aldridge 1992). Clindamycin and cefoxitin resistance have been reported since 1980 and recently, although rare, resistances to imipenem and metronidazole have also been described (Bourgault et al. 1992, O'Donogue et al. 1992). In this study, the resistance rates to clindamycin were 34.5% and 30% for strains from children with and without diarrhea, respectively. Clindamycin resistance frequently has been shown to be conferred by a macrolide-lincosamide-streptogramin B resistance (MLS). Therefore, the clinical use of clindamycin or erythromycin may increase the frequency of clindamycin-resistant strains among Bacteroides species (Macrina & Smith 1993). Interestingly, resistance rates of 23.5% and 22% to cefoxitin for strains isolated from children with and without diarrhea, respectively, were observed. This should be attributed to the wide and indiscriminate use of macrolides, lincosamides and b-lactams in Brazil (Carvalho et al. 1997). Resistance rates ranging from 16 to 22% to cefoxitin have also been documented in other studies (Dubreil et al. 1984, Garcia-Rodriguez & Garcia-Sánchez 1990). In other Brazilian study, Almeida and Uzeda (1987) reported high resistance levels to clindamycin (37%) and cefoxitin (21%) among B. fragilis group strains isolated from the human intestinal microbiota. Moreover, Avelar et al. (2001) found high levels of resistance of the B. fragilis group isolated from children and adults to clindamycin (72.7% and 58.3%), and to cefoxitin (8.3% and 13.5%), respectively. Moreover, tetracycline resistance rates were 51.5% and 54% for bacteria isolated from children with and without diarrhea, respectively, according to Sanders and Aldridge (1992) and Carvalho et al. (1997). By using biological and nitrocefin methods, the b-lactamase production was respectively observed in 32 (50%) and 58 (90.6%) isolates from children with diarrhea, and in 30 (60%) and 45 (90%) isolates from healthy children. Moreover, all the b-lactamase-positive isolates observed by using a biological method also were positive to nitrocefin method. These results suggest that the last method is more sensible than the biological one to detect the b-lactamase activity. However, it is important to note that biological method was tested only with penicillin-resistant isolates. On the other hand, the nitrocefin method is recommended to detect the cephalosporinase and the penicillinase activity. Cáceres et al. (2000) and Aldridge et al. (2001) verified the b-lactamase production in 97.5% and in 77% of the B. fragilis tested, respectively. Most of the enzymes are chromosomally mediated cephalosporinases with activities against many narrow-and-broad-spectrum penicillins and cephalosporins (Bush 1988, Rasmussen et al. 1997). It is mentioned that the bacteria with antimicrobial resistance mechanisms are able to grow and to multiply in gradual higher concentrations of antibiotics and heavy metals. Moreover, it is also suggested that both genetic and physiological bacterial factors could selectively suppress the susceptibility to the antibiotic killing action (Tuomanen et al. 1986). Since a bacterial population consists of different subpopulation of cells there is much to be elucidated on these phenomena among bacteria of the B. fragilis group (Avila-Campos et al. 1991). In their usual habitats, these indigenous microorganisms are constantly exposed to various antimicrobial agents, including heavy metals. The literature on biochemical-physiological mechanisms of susceptibility and on the resistance of microorganisms to some chemical agents, such as heavy metals, is not convincing, but it is suggested that the phenomena could be either chromosome- or plasmid-mediated (Rudrick et al. 1985). Gram-negative bacteria such as Escherichia coli, Salmonella typhimurium, and Pseudomonas sp. carrying transferable plasmids have showed resistance to mercuric ions (Summers & Silver 1978). Moreover, studies have shown that Bacteroides spp. harboring plasmid show resistance to several antimicrobial drugs, but not to heavy metals (Tinnel & Macrina 1976). According to Riley and Mee (1982), it is possible that the heavy metals resistance in this microbial group would be intrinsic, rather than plasmid borne. In this study, a multiple resistance to antibiotics and/or metals was observed in all species of the B. fragilis group isolated from children with and without diarrhea. A resistance rate of 100% was observed to lead and nickel in both analyzed children groups, and to cadmium only in strains isolated from children without diarrhea. These data can be the results of a continue contamination with these metallic ions by agriculture or ground way of humans and animals, mainly in some Brazilian countries such as São Paulo City. On the other hand, the presence of plasmid in these tested strains was associated to antibiotic-resistance but not to metals (data not shown). This result suggests that the metal-resistance in B. fragilis is chromosomally mediated in accordance with Riley and Mee (1982). Resistance rates of HgCl2, AgNO3 and CuSO4 were from 68.5 to 94%, probably partly due to the wide use of these metallic ions in medical centers. Therefore, a political program of using metals and antibiotics is urgent in order to save those therapeutic treatments. Finally, considering the endogenous origin of these bacteria and the conjugal transfer properties among intestinal bacteria, these results are worrisome, and they reaffirm the need to increase the antibiotics and metals resistance surveillance of this microbial group in Brazil. ACKNOWLEDGEMENTS To Mrs Zulmira Alves de Souza for her technical support. REFERENCES
Copyright 2004 Instituto Oswaldo Cruz - Fiocruz. The following images related to this document are available:Photo images[oc04057t2.jpg] [oc04057t3.jpg] [oc04057t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}