 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Mem Inst Oswaldo Cruz, Rio de Janeiro, Vol. 99, No. 4, June, 2004, pp. 425-431 Oral Candida Flora from Brazilian Human Immunodeficiency Virus-infected Patients in the Highly Active Antiretroviral Therapy Era NR Melo/+, H Taguchi**, J Jorge, RJ Pedro*, OP Almeida, K Fukushima**, K Nishimura**, M Miyaji** Departamento de
Patologia Oral, Faculdade de Odontologia de Piracicaba, Piracicaba, SP,
Brasil *Departamento de Moléstias Infecciosas, Faculdade de Ciências
Médicas, Unicamp, Campinas, SP, Brasil **Research Center for Pathogenic
Fungi and Microbial Toxicoses, Chiba University, Chiba, Japan Financial support: Japan International Cooperation Agency, Japan National Institute of Infectious Diseases, and Fundação de Amparo à Pesquisa do Estado de São Paulo (grant 97/07020-2) Received 19 November
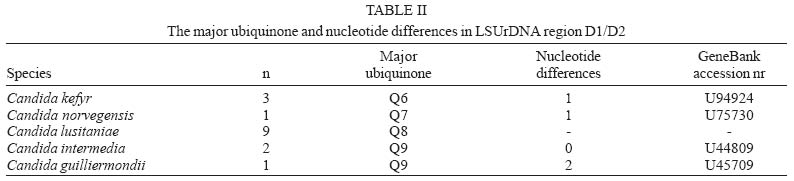
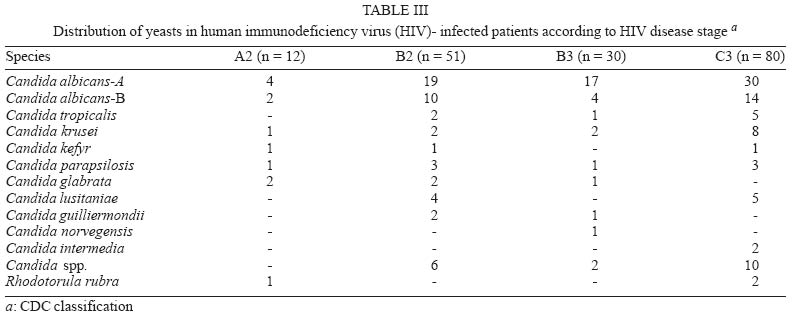
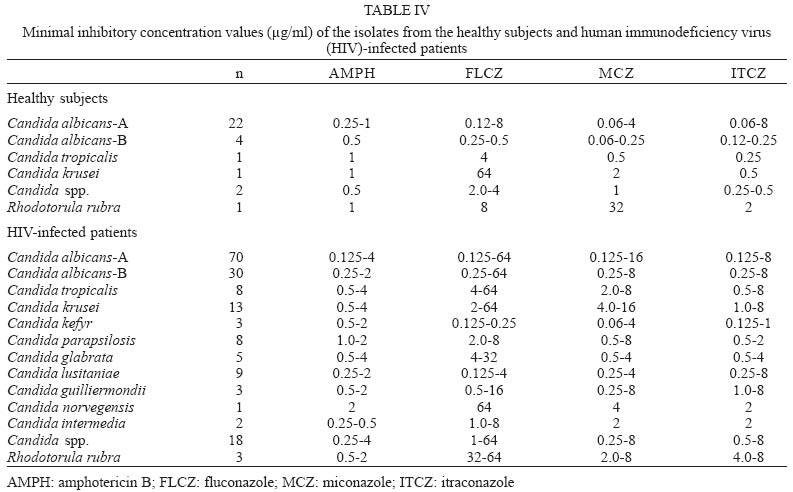
2003 Code Number: oc04075 One of the main opportunistic fungal infections amongst immunocompromised individuals is oral candidosis, which has been found in up to 90% of human immunodeficiency virus (HIV)-infected patients. This study employed yeasts isolated from the saliva and oral cavities of 114 HIV-infected patients living in Campinas, São Paulo. Of the isolates, 57.8% were identified as Candida albicans and 42.1% as non-C. albicans. The latter isolates were subsequently identified as C. krusei (7.5%), C. lusitaniae (5.2%), C. tropicalis (4.6%), C. parapsilosis (4.6%), C. glabrata (2.8%), C. kefyr (1.7%), C. guilliermondii (1.7%), C. intermedia (1.1%), C. norvegensis (0.5%), and Rhodotorula rubra (1.7%). Susceptibility of the isolates to amphotericin B, fluconazole, miconazole, and itraconazole was also determined by a microdilution method adopted by the National Committee for Clinical Laboratory Standards. The isolates demonstrated various susceptibilities to the antifungal agents. In particular 29 C. albicans and 13 non-C. albicans isolates showed low susceptibility to FLCZ (> 64 µg/ml). This study revealed huge diversity of Candida species, in particular the increasing emergence of non-C. albicans associated with the oral flora of HIV-infected patients. Key words: Candida - human immunodeficiency virus - antifungal drug - Brazil Since the human immunodeficiency virus (HIV) was described in the 1980s, the number of HIV-infected patients has continued to increase and at present over than 50 million patients have been documented in the world. Furthermore, opportunistic fungal infections in immuno-compromised hosts have become a serious problem in the medical field (Pfaller et al. 1998). In particular oral candidosis occurs in more than 90% of HIV-infected patients (Korting et al. 1999). Usually the main causative agent of oral candidosis in immunocompromised hosts is Candida albicans, which is a member of oral microbe flora (Odds 1984, Stenderup 1990, Fetter et al. 1993). Nevertheless, in recent years several reports have described a change of oral Candida flora in HIV-infected patients (Nguyen et al. 1996, Nho et al. 1997). This change has been particularly associated with the use of antifungal agents such as fluconazole (FLCZ). FLZC has been the primary choice in fungal infection therapy for HIV-infected patients (Ghannoum & Rice 1999). However, an increasing number of patients with clinical resistance to this azole antifungal compound has been observed (Le Guennec et al. 1995). Resistance to antifungal agents has important implications for morbidity, mortality, and health care costs in hospitals as well as in the community. Hence, substantial attention has been focused on improving methods to detect resistance, designing more effective antifungals against resistant organisms and preventing the emergence and spread of resistance in the first place (Nho et al. 1997). The purpose of this study was to evaluate Candida spp. diversity in the oral cavity of HIV-infected patients and to determine the level of resistance of the clinical isolates to antifungal agents. MATERIALS AND METHODS Isolates from HIV-infected patients - One hundred and seventy three isolates were identified from the oral cavities of 114 HIV-infected patients at the School of Medical Sciences, University of Campinas, state of São Paulo, from August 1997 to January 1999. The patients were classified into 4 groups: A2, B2, B3, and C3, according to the criteria defined by the Review System of Classification of the Center for Disease Control and Prevention (CDC 1993). This classification system for HIV infection emphasizes the clinical importance of the CD4+ T-lymphocyte count in the categorization of HIV-related clinical conditions. Categories 1 to 3 correspond to CD4+ T-lymphocyte counts per microliter of blood. Category 1 denotes cell counts greater than or equal to 500 cells/ml; category 2 indicates cell counts of 200-400 cells/ml, and category 3 means cell counts less than 200 cells/ml. Category A includes asymptomatic HIV infection. Category B consists of symptomatic conditions in HIV-infected adolescent or adult such as bacillary angiomatosis, candidosis oropharyngeal, candidosis vulvovaginal; cervical dysplasia, oral hairy leukoplakia, and constitutional symptoms. Category C includes the 23 clinical conditions listed in the AIDS surveillance such as candidosis of bronchi, trachea, lungs or esophagus. The group C3 was the most frequent (41.2%), followed by the B2 (32.4%), B3 (18.4%), and A2 (7.8%) groups. The patients were on highly active antiretroviral therapy (HAART) that included Indinavir (HIV protease inhibitors), Zidovudina (AZT), Lamivudine (3TC) or other antiretroviral drugs namely, Didanosine, Zalcitabine, Stavudine, Ritonavir, and Saquinavir. Furthermore, patients with fungal infections were treated with oral antifungal and local antifungal agents (itraconazole gel, chlorhexidine rinse or itraconazole pastilles) in addition to oral hygiene orientation. There were 74 males and 40 females; the average age was 35.2 ± 8.2 years. They were racially classified as 95 whites, 9 blacks, and 10 mulattos. Isolates from healthy subjects - Thirty-one isolates from 30 healthy individuals were examined in this study as a control. They did not receive any drugs such as antibiotics, antiretroviral or antifungal agents. There were 17 males and 13 females and the average age was 47.7 ± 8.2 years. They were racially classified as 20 whites, 5 blacks, and 5 mulattos. All isolates were cultured and stored according to the standard procedures (Sandven 1990). Identification Conventional methods - The isolates were identified according to the standard technique (Sandven 1990). They were cultured on corn meal agar (Difco, US), supplemented with 1% Tween 80, at 25°C for 7 days for chlamydospore formation. Germ tube formation was carried out in calf serum (Gibco BR, US) at 37°C for 2 to 4 h. Additionally the isolates were cultured at 30°C for 48 h on chromogenic agar (CHROMagar®, France) (Beighton et al. 1995), and tested with the Candida Check kit® (Iatron laboratories, Inc., Japan) and ID32C® profiled (bioMerieux, Marcy l'Etoile, France). Ubiquinone system - Additionally some non-C. albi-cans isolates were identified by using the ubiquinone system and genetic analyses. C. guilliermondii (ubi-quinone 9, Q9) was used as a control. Briefly, ubiquinones were extracted from mycelia grown in Sabouraud dextrose broth. Extraction, purification and determination of ubiquinones by high performance liquid chromatography were performed as previously described (Billon-Grand 1987, Fukushima et al. 1993). Genetic analysis - The D1/D2 region of the large subunit ribosomal DNA (LSUrDNA) of the same set of samples was sequenced. Genomic DNA extraction from yeast and gram-positive bacteria was carried out using GenTLETM (Tanaka Shuzo Co. Ltd, Otsu, Shiga, Japan) according to the manufacturer's instructions. D1/D2 regions were amplified by the method of Kurtzman and Robnett (1997) using a primer set of (NL-1 5'-GCATATCAATAA GCGGAGGAAAAG) and (NL-4 5'-GGTCCGTGTTT CAAGACGG). Amplification was performed for 30 polymerase chain reaction (PCR) cycles with annealing at 52°C, extension at 72°C for 2 min, and denaturation at 94°C for 1 min. The amplified DNA was purified with SUPRECTM-2 according to the manufacturer's instructions (Takara Bio Inc., Otsu, Shiga, Japan). The PCR amplified D1/D2 regions were directly sequenced in both directions using a Thermo Sequenase II Dye terminator cycle sequencing Kit (Amersham Pharmacia Biotech, Buckinghamshire, UK) by an AbI PRISMTM 377 sequencer. To determine the sequences, the two following internal primers were adopted together with the above external primers: (NL-2 5'-CTTGTTCGCTATCGGTCTC) and (NL-3 5'-GAGA CCGATAGCGAACAAG). The nucleotide sequence data were analyzed by the genetic information processing software, GENETYX-MAC 9.0, 1r 5 (Software Development, Tokyo, Japan). Antifungal susceptibility test Antifungal susceptibility tests were performed using the broth microdilution method according to the guidelines recently published by the National Committee for Clinical Laboratory Standards (NCCLS 1997). Medium - RPMI-1640 medium (Nissui Pharmaceutical Co., Japan) was buffered with morpholinepropanesulfonic acid (MOPS; Sigma Chemical Co.) and adjusted to pH 7.0 (Taguchi et al. 1995). Antifungal agents - Amphotericin B (AMPH) (Bristol-Myers Squibb), fluconazole (FLCZ) (Pfizer Pharm. Inc. Japan), miconazole (MCZ) (Mochida Pharm. Inc. Japan), and itraconazole (ITCZ) (Janssen-Kyowa Co., Ltd., Japan) were tested against the isolates. Procedures - These antifungal reagent-grade powders were dissolved in dimethyl sulfoxide solvent (DMSO) to obtain stock solutions of 12.8 mg/ml. A 10-fold serial dilution was performed in RPMI-1640 medium to provide a working solution for each drug giving final concentration ranges of 0.03 to 16 µg/ml for AMPH B, 0.125 to 64 µg/ml for FLCZ, 0.06 to 32 µg/ml for MCZ, and 0.015 to 8 µg/ml ITCZ. Antifungal agents were serially diluted in 96-well microtiter plates (Falcon, Lincoln Park, NJ). The isolates were subcultured onto PDA slants at 30°C for 24 h. Cell suspensions were prepared in RPMI-1640 medium and were adjusted to give a final concentration approximately 2.5 x 10³ cells/ml. The microdilution plates were incubated at 30°C and the MICs were determined visually at 24 and 48 h. The minimal inhibitory concentration (MIC) was defined as the lowest concentration of antifungal agent at which 80% inhibition of growth (MIC80) occurs compared with that of the growth control well. C. albicans ATCC 90028 and ATCC 90029 were used in each micro-dilution set to ensure quality control. Chi-Square test and Fisher's exact test were applied considering significant differences of p < 0.05. Breakpoints for antifungal susceptibility have been established for Candida isolates tested according to NCCLS. RESULTS AND DISCUSSION Oral yeast flora of healthy subjects and HIV-infected patients - Since the AIDS epidemy the oral candidosis has been one of the major markers of HIV disease progression. The prevalence of oropharingeal colonization and infection by C. albicans has been evaluated worldwide (Cassone et al. 1999, Arribas et al. 2000, Diz et al. 2001). Recently several reports have addressed to the impact of HIV protease inhibitor therapy on Candida spp. colonization (Cassone et al. 1999, Mata-Essayag et al. 2001, Barchiesi et al. 2002). Highly active antiretroviral therapy that includes HIV aspartyl protease inhibitors (PIs) causes a decline in the incidence of some opportunistic infections in AIDS, and this decline is currently attributed to the restoration of specific immunity. Besides the expected immunorestoration, patients receiving PI therapy may benefit from a direct anticandidal activity of these drugs (Cassone et al. 1999). In Brazil and South America there are a small number of reports (Mata-Essayag et al. 2001, Sant'ana et al. 2002) focusing on the epidemiology of C. albicans and emergent non-C. albicans species in HIV-infected patients after the introduction of HAART. In the present study 100% of the patients were on HAART. This is the first Brazilian investigation focusing the impact of HIV protease inhibitors on Candida spp. oral colonization. As shown in the Table I, 57.8% of isolates in HIV-infected patients were C. albicans. Diz et al. (2001) found a similar percentage of C. albicans isolates in HIV-infected patients who were treated with HIV protease inhibitors. The data shown by the authors were different from those reported by Hauman et al. (1993). These last authors investigated yeast flora from the oral cavities of HIV-infected patients who had not taken the HIV protease inhibitor drugs. According to their data, C. albicans was still the main isolate. In a multicenter Brazilian study of oral Candida from AIDS patients performed by Sant'Ana et al. (2002), only 37% of the patients enrolled were on HAART. C. albicans was the most prevalent isolate (91%) and only 9% of isolates were non-C. albicans spp. In contrast our data show an increase of the number and species of non-C. albicans isolates. Non-C. albicans occupied 42.1% of the isolates (Table I). They were as follows: 13 of C. krusei, 9 of C. lusitaniae, 8 of C. tropicalis, 8 of C. parapsilosis, 5 of C. glabrata, 3 of C. kefyr, 3 of C. guilliermondii, 2 of C. intermedia, 1 of C. norvegensis, 18 of Candida spp., and 3 of R. rubra. Nguyen et al. (1996), Dondra et al. (1996), and Fidel et al. (1999) also indicated that non-C. albicans spp. play a role as causative agents in oral candidosis. Recently, several reports have also described a change in the oral Candida flora of HIV-infected patients (Cartledge et al. 1999, Arribas et al. 2000, Diz et al. 2001). The use of various medicines such as antiretroviral agents, antibiotics, and antifungal agents has been pointed as a reason for this change. Furthermore, other authors (Franker et al. 1990, Fotos & Hellstein 1992) reported that the oral Candida flora in patients who had not taken HIV protease inhibitors was occupied with C. albicans up to 80%. Non-C. albicans spp. have been associated with severe symptoms in oral candidosis and have had a major impact in clinical presentation (Redding et al. 2000). In addition, Colombo et al. (1999) indicated that candidemia due to non-C. albicans is increasing in Brazilian tertiary hospitals. Therefore our results emphasized the emergence of non-C. albicans species recently reported (Nguyen et al. 1996, Schoofs et al. 1998, Colombo et al. 1999). Interestingly, no C. dubliniensis isolates were found in our study. C. dubliniensis isolates have been rarely reported in South America, which includes Brazil and Argentina (Rodero et al. 1998, Sano et al. 2000, Mariano et al. 2003) with low incidence of 1.5-2% compared with 14% incidence in worldwide reports (Sullivan et al. 1995, Pinjon et al. 2003). Rare Candida spp. such as C. lusitaniae, C. kefyr, C. intermedia, and C. norvegensis found in our study have been currently isolated and associated with immunocompromised patients (Krcmery & Barnes 2002). In healthy subjects, C. albicans represented almost all of the yeasts (26 isolates) (Table I); others were C. tropicalis (1 isolate), C. krusei (1 isolate), Candida spp. (2 isolates), and Rhodotorula rubra (1 isolate). As shown in the Table I, oral yeast flora of the healthy subjects was monotonous and a similar percentage of 15.9% for non-C. albicans was reported by Schoofs et al. (1998). C. albicans serotype-A was the most prevalent phenotype of C. albicans isolates in both groups studied. This result is in accordance with previous reports (Sant'Ana et al. 2002, Mariano et al. 2003). Analysis of ubiquinone systems and nucleotide sequences of D1/D2 regions of LSUrDNA - When the authors attempted to identify the yeasts isolated from the oral cavities of HIV-infected patients by using conventional methods, some isolates were difficult to identify. In the cases of rare Candida spp., such as C. lusitaniae, C. kefyr, C. intermedia, and C. norvegensis, ubiquinone analysis was useful to identify these isolates. The major ubiquinone of each isolate was determined (Table II); C. lusitaniae isolates showed ubiquinone-8 (Q8), C. intermedia Q9, Q6 for C. kefyr, Q9 for C. guilliermondii, and Q7 for C. norvegensis. For confirmation of identification of the three rare species, C. kefyr, C. intermedia, and C. norvegensis, the nucleotide sequences of the D1/D2 regions of LSUrDNA were analyzed. Nucleotide differences between the isolates examined and those deposited in GeneBank by Kurtzman (Kurtzman & Robnett 1997) are summarized in Table II. No major difference was found among C. kefyr, C. intermedia, and C. norvegensis isolates, which showed only one nucleotide substitution; C. guilliermondii showed two substitutions. Identification methods based on ubiquinone presence have been mainly applied in Chemotaxonomy (Billon-Grand 1987, Fukushima et al. 1993). The chemotaxonomic and genetic data obtained in this investigation supported the conventional methods, therefore the eventual application of chemotaxonomic data to identification particularly in rare species possessing a specific ubiquinone can be an useful alternative. Relationship between oral yeast flora and progress of HIV-disease - Table III shows the relationship between the yeast flora and CDC criteria (CDC 1993). The number and diversity of Candida spp. increased in proportion to the progress of HIV disease. Interestingly, rare Candida spp. such as C. lusitaniae, C. norvegensis, and C. inter-media were isolated from the oral cavities of HIV-infected patients. In the relationship between Candida spp. and CDC classification in HIV-infected patients, the isolates from the initial AIDS stage patients contrasted with those from the severe disease stage. In the B2, B3, C3 stages, we succeeded in isolating several Candida species. The non-C. albicans isolates (91.7%, 67/73) were isolated from patients in the advanced stages (B2, B3 and C3 groups). Redding et al. (2000) reported that late-stage HIV-infected patients have high prevalence of Candida spp. with decreased susceptibility to FLCZ, especially non-C. albicans species. Non-C. albicans spp. are therefore more likely to require higher doses of FLCZ in order for the patients to be cured of fungal infections/ disease. The presence of non-C. albicans isolates may be a consequence of immunodeficiency and action of drug therapy (Sweet 1997). Interestingly, C. glabrata was predominant in groups A2 and B2 compared to B3 and C3. On the other hand, 4 C. lusitaniae isolates were found in the B2 group. This fact is of particular importance because C. lusitaniae has the ability to develop resistance to AMPH, as reported by Nguyen et al. (1996). Effect of antifungal agents on the yeasts isolated from the oral cavity - The prevalence of azole resistance among Candida spp. isolates has been variable both over time and geographical location. In the HIV-infected patients, minimal inhibitory concentration (MIC) ranges were wide and some isolates showed low susceptibility against antifungal agents. Table IV summarizes the effect of 4 antifungal agents on the yeast isolates. Amongst HIV-infected patients, 29 C. albicans and 13 non-C. albicans isolates showed low susceptibility to FLCZ (> 64 µg/ml). Many isolates (80 C. albicans and 63 non-C. albicans) showed low susceptibility to ITCZ (> 2 µg/ml). Interestingly, 23 C. albicans isolates showed a simultaneously low susceptibility to FLCZ (> 64 µg/ml) and ITCZ (> 8 µg/ml). In contrast, Colombo et al. (1999) described that nosocomial candidemias in Brazilian tertiary hospitals were predominantly caused by non-C. albicans isolates, in which FLCZ resistant isolates were rare. We compared the MIC range of C. albicans serotypes and found that 30% (21/70) of serotype A had low susceptibility to FLCZ (> 64 µg/ml) and ITCZ (> 8 µg/ml). Only 6.6% (2/30) of serotype B displayed a low susceptibility to FLCZ (> 64 µg/ml) and ITCZ (> 8 µg/ml). Of the C. krusei isolates, 41.6% (5/13) revealed cross-resistance to FLCZ (> 64 µg/ml) and ITCZ (> 8 µg/ml). In the case of C. glabrata, 60% (3/5) of isolates showed a MIC range of > 32 µg/ml for FLCZ and > 4 µg/ml for ITCZ; Nguyen et al. (1996) reported similar results. Thus, in this study, 17.8% (13/73) non-C. albicans isolates in this study showed cross-resistance to the FLCZ (> 64 µg/ml) and ITCZ (> 8 µg/ml), in contrast to the reports by Pfaller et al. (1998), and Colombo et al. (1999) in which non-C. albicans were susceptible to FLCZ. Antifungal susceptibility of non-C. albicans species varies significantly in contrast to C. albicans. Some non-C. albicans species are inherently or secondarily resistant to FLCZ, for example, 75% of C. krusei isolates, 35% of C. glabrata, 10-25% of C. tropicalis and C. lusitaniae (Krcmery & Barnes 2002). Amphotericin B resistance is also seen in a small proportion: 5-20% of C. lusitaniae and C. rugosa, 10-15% of C. krusei and 5-10% of C. guilliermondii. The isolates from healthy subjects showed narrow minimal inhibitory concentration (MIC) ranges. Five C. albicans isolates showed low susceptibility (> 2 µg/ml) to ITCZ but all C. albicans isolates from healthy subjects were susceptible to FLCZ (0.12-8 µg/ml). Certain non-C. albicans species such as C. glabrata and C. krusei are commonly less susceptible to FLCZ than C. albicans and are being isolated with increased frequency in HIV-infected patients (Redding et al. 2000). In our study only one C. krusei isolate from the healthy subjects showed low susceptibility to FLCZ (> 64 µg/ml) emphasizing that this organism is intrinsically resistant to FLCZ (Fukuoka et al. 2003). In conclusion, according to recent reports, an increase in Candida spp. diversity in the oral cavities of HIV-infected patients is evident. The presence of isolates with low susceptibility to antifungal agents in our study represents a serious problem for the selection of effective antifungal therapy. An increase of recurrent non-C. albicans candidemia episodes with antifungal resistance has also been suggested. Therefore, greater attention should be paid to microbiology routine problems encountered to ensure that non-C. albicans spp. are accurately identified. Our study revealed huge Candida spp. diversity and relevant emergence of rare non-C. albicans in isolates from Brazilian HIV-infected patients under HAART. ACKNOWLEDGMENTS To Chiba University, Japan, Dental Faculty of Piracicaba, DST/AIDS Research Group (GPD); Dr Ademar Yamanaka from Gastrocentro, FCM, University of Campinas, Brazil, Dr Stephen N Smith from Aston University, and Samirah Perally, University of Wales Aberystwyth, UK for proof-reading of this paper. REFERENCES
Copyright 2004 Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc04075t4.jpg] [oc04075t3.jpg] [oc04075t2.jpg] [oc04075t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}