 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Mem Inst Oswaldo Cruz, Vol. 99, Suppl. 1, August, 2004, pp. 51-57 Schistosomal Hepatopathy Zilton A Andrade Laboratório de Patologia Experimental, Centro de Pesquisas Gonçalo Moniz-Fiocruz, Rua Valdemar Falcão 121, 40295-001 Salvador, BA, Brasil Fax: +55-71-356.4292. E-mail: zilton@cpqgm.fiocruz.br Received 28 May
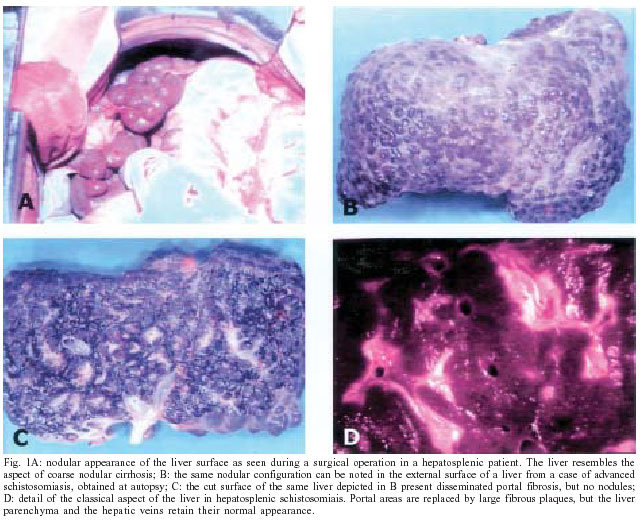
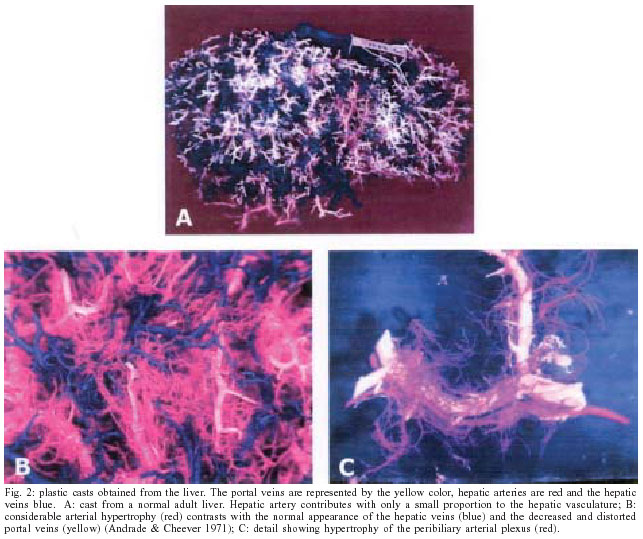
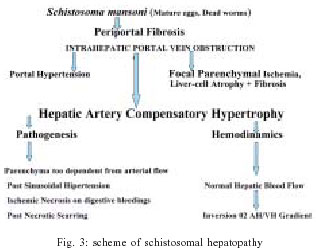
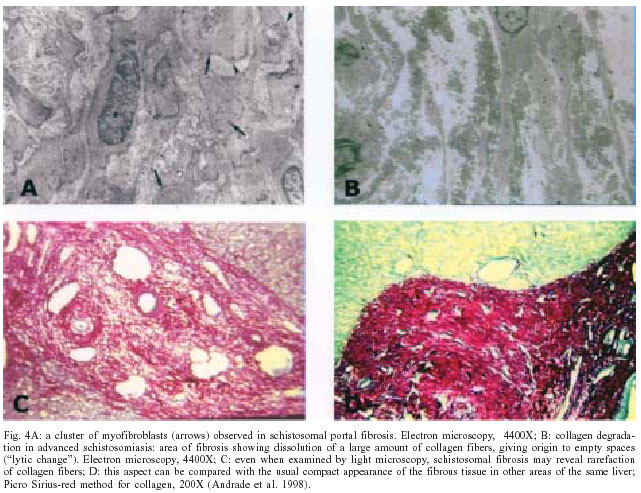
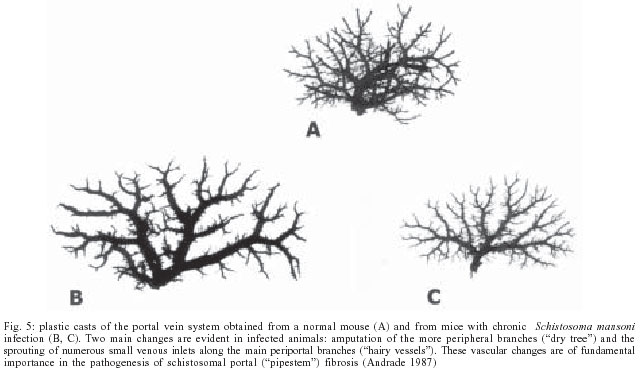
2004 Code Number: oc04086 Gross anatomical features and a complex set of vascular changes characterize schistosomal hepatopathy as a peculiar form of chronic liver disease, clinically known as "hepatosplenic schistosomiasis". It differs from hepatic cirrhosis, although clinical and pathological aspects may sometimes induce confusion between these two conditions. Intrahepatic portal vein obstruction and compensatory arterial hypertrophy render the hepatic parenchyma vulnerable to ischemic insult. This may lead to focal necrosis, which may give place to focal post-necrotic scars. These events are of paramount importance for the clinico-pathological evolution of schistosomal hepatopathy. Although portal fibrosis due to schistosomiasis sometimes reveals numerous myofibroblasts, it does not mean that such fibrosis belongs to a peculiar type. Damage to the muscular walls of the portal vein may be followed by dissociation of smooth muscle cells and their transition toward myofibroblasts, which appear only as transient cells in schistosomal portal fibrosis. Studies made with plastic vascular casts, especially those with the murine model of "pipestem" fibrosis have helped to reveal the mechanisms involved in systematized portal fibrosis formation. However, the factors involved in the pathogenesis of hepatosplenic disease remain poorly understood. A process of chronic hepatitis is a common accompaniment of portal fibrosis in schistosomiasis. Most of the times it is caused by concomitant viral infection. However, no especial interaction seems to exist between schistosomal hepatopathy and viral hepatitis. Key words: schistosomiasis - Schistosoma mansoni - hepatic fibrosis - vascular changes Advanced schistosomiasis produces in man one of the most characteristic gross picture presentation of hepatic pathology. On the cut surface of the liver this lesion appears as whitish fibrous plaques replacing portal spaces on a background of normal looking hepatic parenchyma (Fig. 1C, D). Exactly one century ago, Symmers (1904) classically described this picture after performing autopsies in Egypt. It represents the anatomical counterpart of the clinical condition known as hepatosplenic schistosomiasis. A cursory gross and microscopic examination of the lesion will reveal important clues about its pathogenesis. It can then be noted that the lesion resulted from the deposition of numerous schistosome eggs along the periportal tissues, which provoked chronic granulomatous inflammation with consequent fibrous expansion of the portal spaces and intrahepatic portal vein obstruction. The parenchyma usually maintains its normal architecture, in a good correlation with the preservation of the normal hepatic function, as usually exhibited by the patients. The presence of numerous eggs points to the pathogenetic importance of worm load. Thus, schistosomal hepatopathy seems a good example of a straightforward condition, with a simple, characteristic, and understandable pathology. Although these main lines mentioned above are correct, they say little about the complexities that this unique type of chronic hepatopathy discloses when more closely and properly investigated. A closer view of its physiopathology will reveal several points of interests that are usually overlooked, but that are important for the understanding of the disease in patients and so are worth discussing here. Schistosomal hepatopathy represents a special type of a chronic liver disease. Its pathology contains unique features, one of the most important refers to its vascular changes, which differs from those found in cirrhosis, and are key factors for the understanding of the fundamental pathogenesis and the clinical potential for evolution presented by hepatosplenic schistosomiasis. RELATIONSHIP TO HEPATIC CIRRHOSIS In his seminal description of the gross lesion of advanced schistosomiasis in man, Symmers (1904) used the term "cirrhosis". From time to time this term has emerged in the literature, and even in some textbooks there are references to "schistosomal cirrhosis". But, can schistosomiasis causes hepatic cirrhosis? It is usually admitted that the clinical presentation of hepatosplenic schistosomiasis markedly differs from that of cirrhosis. Although the signs and symptoms of portal hypertension and hypersplenism are dominant in schistosomiasis, the counterpart of hepatocellular failure is conspicuously absent. However, some patients with schistosomiasis do evolve to an end-stage of the disease by exhibiting muscular waste, hypoalbuminemia, ascite, and coma. These observations led to the concept of compensate and decompensate schistosomiasis, to differentiate patients with sole manifestations of portal hypertension (splenomegaly, esophageal varices) from those who, in addition, presented signs of hepatocellular failure. Admitting the existence of these two clinical types, a logical conclusion is that hepatosplenic schistosomiasis can evolve toward a true cirrhosis, at least from a clinical point of view. Although this conclusion could be correct, it has not been supported by a clear morphological correlation. A brief analysis of the literature may help to explain why the relationship of advanced schistosomiasis with hepatic cirrhosis has sometimes given place to confusion. Until recently the terms "cirrhosis" and "fibrosis" were considered as synonymous, so data from the earlier literature can be discarded on their conceptual significance. On the other hand, some early investigators used to consider the presence of schistosome eggs in histological sections, especially when in great numbers, as an indicator of the etiology of cirrhosis. Probably that was the reason why Jaffé (1941) has stated that schistosomiasis can be the cause of any morphologic type of cirrhosis. But, one of the most important reason why someone still continue to believe that schistosomiasis can result in cirrhosis, has been the failure to recognize the focal nature of the "cirrhotic" changes (nodular hepatocellular regeneration and fibrous septa and bands) sometimes observed in gross specimens and in histological sections from cases of hepatosplenic schistosomiasis. This can lead to confusion particularly when examination is restricted to the external surface of the liver, such as occurs during surgery (Fig. 1A), or even during autopsy (Fig. 1B). Bogliolo (1957) clearly recognized the main pathological differences between schistosomal hepatic periportal fibrosis and cirrhosis. His main argument was that no widespread parenchymal subversion occurred only in the former. Focal areas of post-necrotic scarring occur frequently in advanced schistosomiasis. They result from focal ischemic necrosis in a liver parenchyma too much dependent on arterial blood supply, as we shall see below. Others have suggested hemodynamic changes as a mean to differentiate the two conditions. While schistosomiasis courses with normal or near-normal sinusoidal pressure, that is indicated when the hepatic vein is wedged occluded, the so-called pre-sinusoidal type of portal hypertension, cirrhosis presents itself with elevated sinusoidal pressure, therefore a post-sinusoidal type, (Coutinho 1968, Cerri et al. 1984). Soon it was observed that such differentiation did not apply to advanced cases of schistosomiasis, in which sinusoidal pressures were seen to vary from pre-sinusoidal type levels up to the highest figures ever found in cirrhosis (Alves et al. 1977). The understanding of these features needs a discussion on vascular changes. VASCULAR CHANGES One of the most characteristic features of schistosomal hepatopathy is related to its vascular alterations. Studies with the techniques of plastic injection and corrosion in strong acid have yielded casts where the three vascular systems (portal vein, hepatic vein, and hepatic artery) were represented at the same time and with different colors. These casts have revealed that the portal vein system is severely reduced and distorted; the hepatic veins are within normal limits and the hepatic artery exhibits marked hyperplasia and hypertrophy (Fig. 2). This hypertrophy is probably a compensatory phenomenon in face of the progressive and extensive obliteration and amputation of portal vein branches from the lesions induced by the schistosome eggs. These changes are so decisive that hepatosplenic schistosomiasis can be considered as an example of a vascular disease of the liver. The relationship of the portal obstructive lesions to the manifestations of portal hypertension is obvious. The plastic casts revealed marked decrease of the portal vascular bed, with disappearance of the smallest branches and severe distortions of medium and large branches. Sudden diminution of caliber, formation of short-circuit by-passes, tortuosities, multiple focal dilatation, besides the formation of a cuffing of small branching vessels around the main portal vein branches represented the main alterations affecting the portal vein system. But, still the most impressive change was hepatic artery hypertrophy (Andrade & Cheever 1971). The arterial vessels predominate above all the others vessels seen in plastic-corrosion preparations following the simultaneous demonstration of the three vascular systems of the liver. A dense concentration of fine branching arterial vessels appears in the proximity of the larger portal vein branches, probably representing the hypertrophied peri-biliary plexus (Fig. 2C). This had no direct connection with the venous cuffing originated from portal vessels, which is also an impressive change. Experimentally, a considerable hypertrophy of the hepatic arterial tree was produced in rats after a two-step total portal vein ligation (Almeida-Melo et al. 1983). The rats with prolonged total portal vein ligation preserved a normal hepatic structure and even methods of enzymatic histochemistry, applied to hepatocytes, gave results that did not differ from those of normal intact rats. Thus, the liver can maintain its normal structure in the absence of portal blood. However, some important consequences may result thereafter, one of them being the increase of collagen fibers in Disse spaces, with capillarization of the hepatic sinusoids. Other, the increased sensitivity of the parenchyma to drops in arterial pressure and defective perfusion, which is known to occur during massive gastro-intestinal bleeding following rupture of esophageal varices (Andrade 1965). As a matter of fact intrahepatic portal vein obstruction coupled with compensatory arterial hypertrophy turn the liver parenchyma too dependent on arterial perfusion. When the patients present gastro-intestinal bleeding (rupture of esophageal varices) and sudden drop in arterial pressure, parenchymal perfusion may become critical to the point where focal ischemic necrosis is produced. Hepatosplenic patients with a history of significant bleeding episodes a few days before dying, usually show focal areas of parenchymal necrosis, of variable extension, at necropsy, especially in sub-capsular areas of the liver. It is presumed that such areas would undergo post necrotic scarring, in case the patients survive, with nodular regeneration of the parenchyma delimited by fibrous bands and septa. Such focal "cirrhotic" areas are frequently seen in autopsy or biopsy specimens taken from patients with advanced schistosomisis (Andrade 1989). There are other important consequences from arterial hypertrophy. Hemodynamic studies have revealed that general hepatic blood flow in hepatosplenic schistosomiasis is conserved within normal limits, which can only happen if arterial flow is compensating for the poor portal perfusion (Ribeiro Jorge 1967). Also, the hepatic vein/hepatic artery oxygen gradient is reduced as compared to that in normal subject and in cirrhosis. Our own studies demonstrated that sinusoidal hypertension in schistosomiasis, as measured by the occluded wedged hepatic vein pressure, is dependent on arterial hypertrophy (Alves et al. 1977). During surgery for splenectomy, patients with the catheter inside the hepatic vein presented marked reduction of the elevated hepatic vein pressure when the main trunk of the hepatic artery was digitally compressed. This same procedure made in a patient without artery hypertrophy did not interfere with the sinusoidal pressure. The influence of compensatory arterial hypertrophy in advanced schistosomiais is abstracted in Fig. 3. IS SCHISTOSOMAL PORTAL FIBROSIS PECULIAR? Portal fibrosis is systematized, which means that it involves the whole liver, extending from the smallest to the largest portal space. Its consistence is variable. Sometimes it resembles a spongy tissue, such the great amount of small, dilated and congested blood vessels present. Some may consider it a special type of vasculo-connective tissue. Other times it appears so dense as to suggest a keloid scar. Grimaud and Borejovick (1977, 1986) supported that possibility when they found myofibroblasts in great numbers in human schistosomal fibrosis examined by electron microscopy. They suggested that the presence of myofibroblasts not only disclosed the keloid nature of the portal scar, but turned portal fibrosis into a contractile tissue (Fig. 4A). The role a peculiar contractile tissue like this could play on the mechanisms of portal hypertension appeared obvious. However, our own data showed that myofibroblasts in schistosomal portal fibrosis were focally accumulated around damaged portal veins, since they originated from dissociation of the muscular coat of portal vein walls, followed by dispersion of smooth muscle cells and their further differentiation into myofibroblasts (Andrade et al. 1998). It was also observed that these myofibroblasts behaved as transient cells, some becoming fibroblasts and others disappearing, probably undergoing apoptosis. Signs of focal collagen breakdown and resorption are frequently noted in portal fibrosis examined by electron microscopy (Fig. 4B). Lysis, breakdown and disappearance of collagen fibers can be also observed by routine histology (Fig. 4 C, D). These changes are a good illustration of the concept that the extracellular matrix is under a dynamic state of equilibrium between forces of synthesis and breakdown. When fibrogenesis is stimulated by the presence of an inflammatory stimulus (mature schistosome eggs) excess collagen accumulates and fibrosis increases. On the contrary, cure of schistosomiais may lead to fibrosis resorption, which is apparently associated with a complex vascular adjustment and the clinical cure of hepatosplenic disease (Andrade 1994). Several clinical and pathological studies have shown that schistosomal hepatopathy is a reversible condition. This is another particular difference between schistosomal fibrosis and hepatic cirrhosis (Richter 2003). By the nature and distribution of its cellular and extracellular components, by its reversibility potential, portal fibrosis in schistosomiasis is not peculiar, but similar to any other fibrous cicatricial tissue in the organism. PATHOGENESIS Everyone would agree that the worm load is an essential factor for the development of schistosomal hepatopathy. The evidences come from several sources, with data from pathology to parasitology, epidemiology and so on. On the other hand, no case of schistosomal hepatopathy has been observed to develop from a mild and prolonged infection. On the other hand, the presence of high worm load does not mean that a patient will develop the advanced lesions of schistosomal hepatopathy. The influence of several factors, such as host age and gender, genetic background, nutrition, immunological status, and environmental factors have been discussed, but evidences for their specific roles in pathogenesis are incomplete (Prata 1991). There is no explanation for what is commonly observed in endemic areas: the large majority of those infected present mild forms of the infection, while only a few develop severe manifestations. Furthermore, it is not known why infected people who emigrate from an endemic area rarely develop pipestem fibrosis (Coura 1975). If transmission is abolished from an endemic area, severe manifestations of schistosomiasis, including hepatosplenic disease, tend to subside, which points to the influence of re-infection in pathogenesis. Re-infection in a murine model of pipestem fibrosis resulted in an increase in the percentage of the lesion, but there were no statistically significant differences between re-infected and single-infected animals as far as worm load (number of eggs/gram of liver tissue) was considered (Coelho et al. 1996, Santos et al. 2000). When other differences were searched between the groups with and without pipestem fibrosis, it was found that both presented a Th2 pattern. In addition, no significant differences appeared when the in vitro levels of Schistosoma mansoni-induced lymphocyte proliferation or the serum-level of anti-S. mansoni antibodies (IgE, IgG1, IgG2a, IgG2b, IgG3) were compared (Flannery 2003). In spite of the incomplete knowledge about the factors that may influence the development of schistosomal hepatopathy, data obtained from human (Andrade & Cheever 1971) and experimental (Andrade 1987, Flannery 2003) materials have demonstrated the mechanisms of periportal fibrosis production. These studies suggested that massive embolization of eggs to the portal system results in obliteration of fine vessels at the periphery of the vascular bed. The increased intrahepatic venous pressure induces the opening of periportal collaterals. These collaterals may be progressively involved by the continous arrival of more schistosome eggs, resulting in inflammation, fibrosis and vascular obliteration along all the periportal spaces (Fig. 5). THE SIGNIFICANCE OF CHRONIC HEPATITIS Besides the presence of periovular granulomas, the fibrotic portal spaces frequently show diffuse mononuclear leukocyte infiltration, sometimes with differentiation of lymphoid follicles and signs of interface activity ("piece-meal necrosis"). The etiology of this chronic hepatitis is usually difficult to be established. Schistosomiasis itself can cause a certain degree of chronic hepatitis, probably of a reactive nature. The presence of this hepatitis in experimental animals can be easily observed. Sometimes it assumes prominent features and may disappear following curative treatment of schistosomiasis (Andrade & Cheever 1995). On the other hand, patients with hepatosplenic schistosomiasis are 7 to 10 times more susceptible to co-infection with hepatitis B virus than healthy blood donors from the same geographic area or even patients with mild schistosome infection. Patients presenting the hepatosplenic form of schistosomiasis associated with hepatitis B usually show persistent viremia and exhibit chronic active hepatitis on liver biopsy, sometimes with the clinical picture of so-called decompensated schistosomiais, evolving to cirrhosis. Similar findings were also observed with viral hepatitis C (see review in Andrade et al. 2001). However, some studies denied any special relationship between schistosomiasis and infections with hepatotropic viruses. The subject has been thoroughly reviewed in an article that significantly bears the title: "Hepatitis B and schistosomiasis: interaction or no interaction ? (Chen et al. 1993). We used an experimental model susceptible to both schistosomiasis and viral hepatitis in an attempt to clarify these controversies. The woodchuck (Marmota monax) is unique in this regard, since it is both susceptible to a B-virus-like hepatitis, the woodchuck hepatitis virus (WHV) and to S. mansoni. Nine woodchucks inoculated with the hepatitis virus alone presented several degrees of acute and chronic hepatitis, one of them dying of hepatocarcinoma one year after inoculation. Four woodchucks with concomitant viral and schistosome infections presented a simple additive pattern of lesions, without any evidence of modification or aggravation of either one of the two infections. The viral load was analyzed and was not influenced by the presence of schistosomiasis in woodchucks. Therefore, schistosomiasis and viral hepatitis in woodchucks run parallel courses, with no apparent special features derived from the association of the two conditions (Andrade et al. 2001). There are several studies which indicated that the problem concerning the association of viral hepatitis and schistosomiasis derived from observations made on hospitalized patients, but are not confirmed by studies from endemic areas. Populational studies made in an endemic area of schistosomiasis in the state of Bahia, Brazil, concluded that no correlation between viral hepatitis and schistosomiasis was whatsoever observed, especially when hepatosplenic disease was considered (Tavares-Neto 1997). Another study made on liver biopsy material from 100 patients with hepatosplenic schistosomiasis, all of them investigated for the presence of serum virus-markers, revealed that the carrier state, mild to severe chronic hepatitis, and even cirrhosis and hepatocarcinoma can be found in patients presenting both viral hepatitis and severe schistosomiasis. Also, chronic hepatitis can be found in virus-marker negative hepatosplenic patients. Thus, evolutionary possibilities for hepatitis virus infection in patients with schistosomiasis are the same as for the general population (Rocha 1998).
Copyright 2004 Instituto Oswaldo Cruz - Fiocruz. The following images related to this document are available:Photo images[oc04086f3.jpg] [oc04086f4a-d.jpg] [oc04086f2a-c.jpg] [oc04086f1a-d.jpg] [oc04086f5a-c.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}