 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Mem Inst Oswaldo Cruz, Rio de Janeiro, Vol. 99, No. 8, December, 2004, pp. 895-897 Short Communication Hepatitis C Virus Genotypes in Blood Donors from the Federal District, Central Brazil Regina MS Amorim/++, Claudiner P Oliveira/++, Patrícia S Wyant/++, Daniela M Cerqueira/++, Geni NL Câmara*, Luciano S Flores**, Regina MB Martins***, Cláudia RF Martins/+ Departamento de
Biologia Celular, Instituto de Biologia, Universidade de Brasília,
ICC Sul, 70919-900 Brasília, DF, Brasil *Agência Nacional de
Vigilância Sanitária, Brasília, DF, Brasil **Hemocentro
de Brasília, Brasília, DF, Brasil ***Universidade Federal de
Góias, Goiânia, GO, Brasil Received 24 May
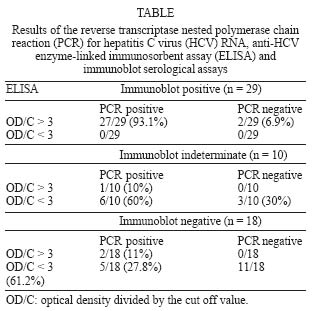
2004 Code number: oc04175 The objective of this study was to characterize hepatitis C virus (HCV) genotypes in blood donors from the Federal District, Central Brazil, and to compare HCV screening by serological assays and reverse transcriptase polymerase chain reaction (RT-PCR). Plasma samples from 57 individuals with reactive or indeterminate results in serological anti-HCV screening assays (ELISA or EIA) were tested for HCV RNA by RT-PCR. The results from a confirmatory LIA serological assay were also evaluated. The 5' non-coding region of the HCV genome was amplified from 41 PCR positive samples (71.9%), which were further characterized by nucleotide sequencing analysis. Of these, 60.9% were of HCV genotype 1 and 39.1% of genotype 3. Key words: hepatitis C virus - genotypes - Federal District, Central Brazil Hepatitis C Virus (HCV) has been classified into six major genotypes and several subtypes, which may produce clinically relevant differences in the response to interferon therapy. Infection with genotype 1 is associated with a poorer response to interferon treatment when compared to infection with other genotypes (Zein 2000). Genotypes 1, 2, and 3 have a worldwide distribution. Genotype 4 is more prevalent in North Africa and in the Middle East, while genotypes 5 and 6 occur more commonly in South Africa and Asia, respectively (Zein 2000). In Brazil, several studies have shown that genotype 1 is the most prevalent one, followed by genotype 3 (Bassit et al. 1994, Krug et al. 1996, Martins et al. 1998). Molecular and serological detections of HCV play an important role in the diagnosis of infection, therapeutic decision-making, and assessment of the virologic response to therapy. In addition, it might reduce the frequency of post-transfusion hepatitis (Smith et al. 1995, Zein 2000, Pawlotsky 2002). The purpose of the present study was to characterize HCV genotypes in volunteer blood donors from the Federal District (Central Brazil) and to compare the results of routine serological assays with those obtained by HCV reverse transcriptase polymerase chain reaction (RT-PCR). Plasma samples from 57 voluntary blood donors were obtained between March 2001 and June 2002 at two blood banks located at the Federal District: the Hemocentro and the Hemoclínica of the Santa Lúcia Hospital. The Committee on Research Ethics from the University of Brasília granted prior approval to this research project. Serum samples were previously screened using routine HCV enzyme immunoassays (ELISA - Ortho Diagnostics Systems or EIA - Abbott Prism HCV). The results of these anti-HCV assays were expressed as the optical densities (OD) of the samples divided by the cut off value (C). Samples with ratio OD/C < 0.9 were considered non-reactive, and those with ratio OD/C > 0.9 and < 1.1 were classified as indeterminate. Samples with ratio OD/C > 1 and < 3 were reactive and those with OD/C > 3 were highly reactive. All 57 samples were retested by a supplementary line immunoblot assay (Lia Tek HCV III, Organon-Teknika). All tests were performed according to the manufacturer's instructions. The 57 samples, all classified as reactive or indeterminate by ELISA, were subjected to RNA extraction using the QIAmp Viral RNA Kit (Qiagen), according to the manufacturer's protocol. Complementary DNA (cDNA) was synthesized from 2 µl of extracted RNA using 200 U of M-MuLV RT (Gibco-BRL) plus 0.2 mM each dNTP (Gibco-BRL), 2 U RNAse inhibitor (Pharmacia Biotech), and 0.5 µg of random primer. The reaction condition was 42°C for 90 min. The cDNA was used as a template in a nested PCR amplification by using two primer sets matching a conserved region in the 5' UTR of the different HCV genotypes (Ginabreda et al. 1997). One microliter of the resulting cDNA was used in outer PCR amplification, in a total volume of 50 µl over 35 cycles, each consisting of 15 s at 94°C, 45 s at 50°C and 1 min at 72°C. A final step (7 min at 72°C) was included after the last cycle. The solution was adjusted to a final concentration of 0.25 mM each dNTP (Gibco-BRL), 1x Taq buffer (Gibco-BRL), 20 nM of each primer, and 2 U Taq polymerase (Gibco-BRL). From the first round of amplification, 1 µl was re-amplified with the nested primers in the same conditions. For each PCR assay, water and an anti-HCV negative sample were used as negative controls. The amplification gave a 253-bp product from HCV RNA positive samples. Nested PCR products were sequenced automatically by the dideoxynucleotide chain termination method, in a Megabace System (Amersham-Pharmacia). The homology among HCV sequences from the Federal District and those already deposited at GenBank was analyzed using the BLAST program (available at http://www.ncbi.nih.nlm.gov). A data bank was generated and analyzed in EPI-Info, 6.04d, from the Center of Diseases Control and Prevention (CDC). The level of significance of tests (p) was set at 0.05. The median age of the 57 blood donors included in our study was 33.5, ranging from 18 to 57 years old. The majority of them were men (78%) and first-time donors (82%). Twenty-two individuals (38.6%) reported risk factors possibly associated to HCV transmission: intravenous drug use (40.9%), surgery (36.4%), blood transfusion (9.1%), and sexually or parentally transmitted diseases (4.5%). HCV RNA positivity was found in 41 samples (71.9%). At a previous study in Central Brazil, Martins et al. (1994) found a similar frequency (76.6%) of HCV viremia in anti-HCV positive blood donors. These PCR positive samples were genotyped by nucleotide sequences similarity analysis using BLAST. The frequency of genotype 1 was 60.9% and that of genotype 3 was 39.1%. The 41 PCR positive samples were subtyped as 1a (34.1%), 1b (26.8%), and 3a (39.1%). In the supplementary immunoblot assay, 50.8% (n = 29) were reactive, 17.6% (n = 10) had an indeterminate result, and 31.6% (n = 18) were non-reactive. Of the 41 PCR positive samples, 65.8% (n = 27) had a reactive, 17.1% (n = 7) an indeterminate, and 17.1% (n = 7) a non-reactive result on the immunoblot supplementary assay. For the 16 samples with a negative result on PCR, 68.75% were also negative, 18.75% were indeterminate, and 12.50% were positive on immunoblot assay. The correlation between HCV viremia and positivity by serological assays is shown in the Table. Due to the fact that some authors previously reported a relation between anti HCV ratio > 3 and detectable HCV-RNA by RT nested PCR (Gretch et al. 1992, Gonçalves et al. 2000), the 57 samples initially classified as reactive or indeterminate on the anti-HCV serological assay were further divided into two groups: 56.1% (n = 32) had ratio OD/C > 3 and 43.9% (n = 25) < 3. Among the 32 samples with OD/C > 3, 93.7% (n = 30) were positive for HCV RNA by PCR, whereas the 25 with OD/C < 3 only 44% (n = 11) were PCR positive. No correlation between anti HCV reactive, PCR positive samples and ALT levels was observed (p = 0.40) and only four individuals showed elevated levels of transaminases. Nowadays, the prevention of transfusion-associated hepatitis C in Brazil relies on the screening of blood samples and the prevalence of anti-HCV reactive samples among blood donors in Brazil was 0.52% in 2001 and 0.48% in 2002 (http://www.anvisa.gov.br). Nevertheless, PCR may improve the reliability of HCV diagnosis and is very sensitive and specific in detecting viremia and therefore potentially infectious blood donors (Sönmez et al. 1996, Ginabreda et al. 1997, Gonçales et al. 2000). We found a correlation between the presence of serum HCV RNA and anti-HCV positivity (p < 0.05). However, among individuals with the ratio OD/C < 3 on ELISA and classified as indeterminate or negative by the supplementary immu-noblot assay, HCV RNA was identified in 44% of the sample. Immunoblot indeterminate results were generally (70%) associated with PCR positivity, indicating the need to screen these donors for HCV-RNA in peripheral blood. These results suggest that anti-HCV assays are not sensitive enough to screen all asymptomatic HCV carriers. Two samples (3.5%) had a high OD/C ratio on ELISA (> 3) and a positive result on the supplementary im-munoblot, but were negative for HCV RNA. This may reflect very low levels of viremia or virus clearance, since a proportion of individuals varying from 15 to 25% do not progress to chronic infection (Hoofnagle 2002). Routine immunoassays, such as ELISA, proved to be valuable in identifying potentially infectious donors capable of transmitting hepatitis C, mainly in individuals with OD/C ratios > 3. We observed that, in most cases (93.7%), this high anti-HCV ratio was associated with HCV-RNA positivity by PCR. However, the screening of low-risk populations such as blood donors can give a substantial number of anti-HCV false-positive results, mainly when low ELISA optical densities are obtained (Martins et al. 1994). We observed that 24.6% of the sera with OD/C < 3 were negative by RT-PCR. Genotyping of HCV isolates has been shown to be of clinical importance. Nucleotide sequencing analysis of a selected part of the viral genome has been used to determine the genotype of HCV isolates (Ginabreda et al. 1997). To limit the occurrence of false-negatives in the PCR assay, we used primers in the 5'UTR of the HCV genome, which is over 98% conserved among different isolates (Ginabreda et al. 1997). The usage of the 5'UTR sequencing for HCV subtyping is considered controversial, since this is a very conserved region of the genome (Pawlotsky 2002). Generally, only genotypes are used for clinical decision related to therapy as different subtypes from the same genotype have few clinical consequences (Krug et al. 1996, Pawlotsky 2002). The highest prevalence of HCV genotype 1 (60.9%), followed by genotype 3 (39.1%) in the Federal District corroborates previous data from Brazil. In Bahia, Northeastern Brazil, HCV genotype 1 is the most frequent one (66.1%), followed by the genotype 3 (33.9%). In the Southeast Region, genotype 1 is also predominant (55%), followed by genotypes 3 (37%), and 2 (8%) (Bassit et al. 1994, Krug et al. 1996, Martins et al. 1998, Busek & Oliveira 2003, Codes et al. 2003). ACKNOWLEDGEMENTS To John Penney, for reviewing this manuscript. REFERENCES
Copyright 2004 Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc04175t1.jpg] |
| |||||||||

{kind=link}