 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Mem Inst Oswaldo Cruz, Rio de Janeiro, Vol. 100, No. 1, February ,2005, pp. 73-78 Human immunodeficiency virus type 1 (HIV-1) genotyping in Rio de Janeiro, Brazil: assessing subtype and drug-resistance associated mutations in HIV-1 infected individuals failing highly active antiretroviral therapy JC Couto-Fernandez/+, C Silva-de-Jesus, VG Veloso*, M Rachid**, RSG Gracie***, SL Chequer-Fernandez, SM Oliveira****, D Arakaki-Sanchez****, PJN Chequer****, MG Morgado Laboratório
de AIDS e Imunologia Molecular, Departamento de Imunologia, Instituto Oswaldo
Cruz-Fiocruz, Av. Brasil 4365, 21045-900 Rio de Janeiro, RJ, Brasil *Instituto
de Pesquisa Clínica Evandro-Chagas-Fiocruz, Rio de Janeiro, RJ, Brasil
**Secretaria Estadual de Saúde do Rio de Janeiro, Rio de Janeiro,
RJ, Brasil ***Laboratório de Geoprocessamento-DIS/CIC/Fiocruz, Rio
de Janeiro, Brasil ****Programa Nacional de DST e AIDS, Ministério
da Saúde, Brasília, DF, Brasil +Corresponding author. E-mail: coutofer@ioc.fiocruz.br Received 7 July
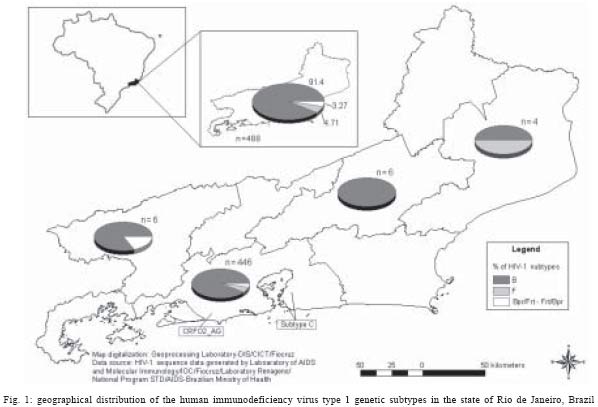
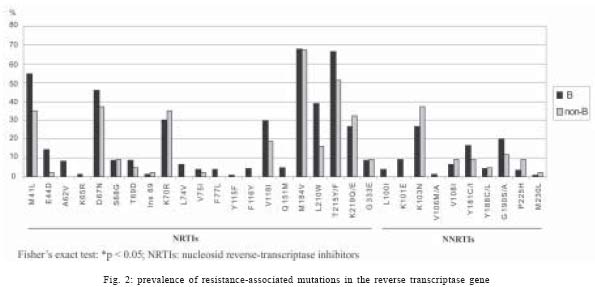
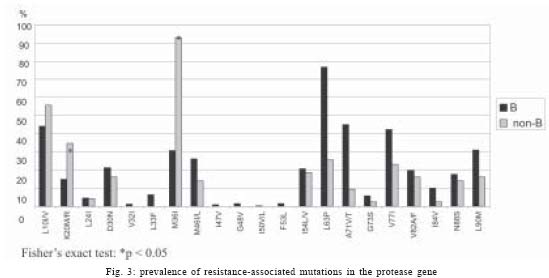
2004 Code number: oc05014 In order to assess the human immunodeficiency virus type 1 (HIV-1) drug resistance mutation profiles and evaluate the distribution of the genetic subtypes in the state of Rio de Janeiro, Brazil, blood samples from 547 HIV-1 infected patients failing antiretroviral (ARV) therapy, were collected during the years 2002 and 2003 to perform the viral resistance genotyping at the Renageno Laboratory from Rio de Janeiro (Oswaldo Cruz Foundation). Viral resistance genotyping was performed using ViroSeqTM Genotyping System (Celera Diagnostic-Abbott, US). The HIV-1 subtyping based on polymerase (pol) gene sequences (protease and reverse transcriptase-RT regions) was as follows: subtype B (91.2%), subtype F (4.9%), and B/F viral recombinant forms (3.3%). The subtype C was identified in two patients (0.4%) and the recombinant CRF_02/AG virus was found infecting one patient (0.2%). The HIV-1 genotyping profile associated to the reverse transcriptase inhibitors has shown a high frequency of the M184V mutation followed by the timidine-associated mutations. The K103N mutation was the most prevalent to the non-nucleoside RT inhibitor and the resistance associated to protease inhibitor showed the minor mutations L63P, L10F/R, and A71V as the more prevalent. A large proportion of subtype B was observed in HIV-1 treated patients from Rio de Janeiro. In addition, we have identified the circulation of drug-resistant HIV-1 subtype C and are presenting the first report of the occurrence of an African recombinant CRF_02/AG virus in Rio de Janeiro, Brazil. A clear association between HIV-1 subtypes and protease resistance mutations was observed in this study. The maintenance of resistance genotyping programs for HIV-1 failing patients is important to the management of ARV therapies and to attempt and monitor the HIV-1 subtype prevalence in Brazil. Key words: human immunodeficiency virus type 1 - subtypes - genotyping - resistance - Brazil The human immunodeficiency virus type 1 (HIV-1) shows remarkable genetic diversity with many implications in pathogenesis, vaccine development, diagnosis, and antiretroviral (ARV) drug susceptibility (Kanki et al. 1999, Caride et al. 2000, Kaleebu et al. 2002). Antiviral resistance is one of the primary reasons for highly active antiretroviral therapy (HAART) failure over time (Shafer et al. 1998, Vella & Palmisano 2000). The emergence of HIV-1 drug-resistant variants within treated patients is attributed to viral replication errors due to the fast replication rate. On average, 10 billion HIV particles are produced every day and, associated to the highly error prone nature of the viral reverse transcriptase (RT), at least one new mutation can be introduced in each new virus genome (Mansky 1998). The selection of drug-resistant viruses during the therapy associated to other factors like, adherence, drug pharmacological factors, and host immune response pressure, also contribute to the evolution of HIV-1 drug-resistance in infected patients (reviewed by Simoni et al. 2003). The knowledge of the HIV-1 resistance patterns has generated information concerning the potential utility of HIV genotyping and phenotyping drug resistance tests for the management of antiretroviral therapy (Hirsch et al. 2000). Genotyping assays for drug resistance determine the nucleotide sequence of HIV-1 protease and RT allowing the detection of resistance associated mutations in the genome that may precede a shift in the phenotyping susceptibility affecting the long-term efficacy of HAART. The primary goal of HIV-1 antiretroviral genotyping is to extend maximal viral suppression for the longest time period, ideally to prevent HIV progression and AIDS complications in treated patients (reviewed by Hisch et al. 2003). Since 1996, the Brazilian Ministry of Health has been successfully conducting programs of universal access to antiretroviral therapy, supplying antiretroviral drugs to the majority of HIV-1 infected patients. By December 2003, approximately 130,000 HIV-1 infected patients in this country have been treated by the Public Health System, substantially contributing to the decrease of the mortality and morbidity levels over the last years in Brazil (Marins et al. 2003, Boletim Epidemiológico 2003 - www.aids. gov.br). However, the emergence of viral resistance during HIV-1 infection may compromise the Brazilian policy for HIV-1 infection treatment. Thus, in order to assess the drug resistance profiles and to improve antiretroviral strategies of therapy in patients failing to respond to previous regimens, the Brazilian Government has established a National Network for HIV Genotyping (Renageno). As a member of this HIV-1 genotyping resistance network composed by 14 laboratories distributed throughout the country, we describe in this paper the HIV-1 drug resistance profile and subtype prevalence in patients failing HAART from state of Rio de Janeiro, Brazil. MATERIALS AND METHODS Population and sample collection - Whole-blood samples from 547 HIV-1 treated-patients that were failing HAART were collected between March 2002 to October 2003 from hospitals distributed through out the state of Rio de Janeiro, Brazil. The genotyping resistance test was performed in patients showing at least tree therapeutic regimen failures, characterized by the persistence of higher viral load counts after continuous use of three or more ARV drugs, including at least one protease inhibitor (IP). All patients were followed at outpatient clinics from the Public Health System and were engaged in the policy of freely accessing ARV drugs sponsored by the Brazilian Ministry of Health. ARV treatment was based on the consensus established by the National Program of STD/AIDS from the Ministry of Health (2003). Patients fulfilling the ARV failing criteria and approved for performance of the genotyping resistance analysis in the Public Health System, signed a written consent accepting their inclusion in the study. The study was approved by the Brazilian National Committee for Ethics in Research (project-Conep 2857). Plasma samples from each patient were separated, aliquoted and stored at -80oC until processing. HIV-1 resistance genotyping and subtype determination - The ViroSeqTM HIV-1 Genotyping System (Celera Diagnostic, Abbott Laboratories, US) was used for the identification of resistance-associated mutations in the HIV-1 polymerase (pol) gene according to the manufacturer. Briefly, the process comprises first the isolation and purification of plasma viral RNAs by ultra centrifugation (21,000 g ´ for 120 mn sample preparation module), followed by cDNA synthesis and genomic amplification by polymerase chain reaction assay (PCR) of the HIV-1 pol fragment (RT-PCR and PCR module), spanning the entire protease (PR) gene and approximately two thirds of the RT gene. A 1.8 kilobase (Kb) amplicon fragment was subsequently used as a sequencing template to generate approximately 1.2 Kb of HIV-1 sequence data. The amplified PCR products were sequenced using seven primers included in the kit, formulated with the BigDye Terminator sequencing chemistry (Sequencing Module - BigDye v.2.0). The sequencing products were analyzed on an ABI Prism ABI 3100 Genetic Analyzer (Applied Biosystems, US) coupled to the DNA sequencing analysis software. The ViroSeqTM HIV-1 Genotyping System consists of a software that automatically imports the sequence data from the sequence analysis software and assembles seven or six sequence segments into a single sequence, which is then compared to the HXB2 reference strain (Kuiken et al. 2002). After the edition and establishment of the consensus sequence, the mutation analysis software (ViroSeqTM software V.2.6) generates the resistance mutation profiles for the different ARV drugs. All sequences obtained from samples were subjected to quality control assessments using the Blast-Renageno resistance analysis web (http://aids.gov.br/renageno) to ensure that were no sample mix-ups or contamination. For the determination of the genetic subtype and in order to confirm the HIV-1 resistance profile, all sequences were analyzed using the Stanford Sequence Resistance Database (http://hivdb.stanford.edu). Mutations were compilated according to the International AIDS Society US consensus (D'Aquila et al. 2002). Samples presenting discordant protease/RT subtyping were further analyzed using the SimPlot program (Ray 1999) to confirm the virus recombinant profile (data not shown). RESULTS A total of 547 HIV-1 infected patients failing ARV therapy from the state of the Rio de Janeiro were sent for genotyping analysis at the Laboratory of AIDS and Molecular Immunology (Renageno Laboratory) of the Oswaldo Cruz Institute-Fiocruz. The majority of the patients (90%) resides in the metropolitan region and surrounds (17% - Niterói and São Gonçalo). The majority of the studied patients (64%) showed more than 200 cells/mm3 of CD4 cell counts and plasmatic viral load (80%) higher than 10,000 copies/ml. A total of 488 plasma samples (89.2%) from treated patients were successfully amplified by the PCR technique and consequently genotyped using ViroSeq Genotyping System and the HIV-1 genetic subtypes were also determinated. A map of the Rio de Janeiro territory showing the distribution of HIV-1 subtypes found across the eight different regions is depicted in Fig.1 (Limonad 1996). From the 488 HIV-1 resistant genotyped patients, we were able to precisely determine the geographical origin for 95.3% of them. Based on the genotyping database, 445 (91.2%) samples were classified as subtype B, followed by 24 (4.9%) subtype F and 16 (3.3%) viral recombinant forms between subtypes B and F. The recombinant B/F variants showed different recombination patterns when both genomic regions (PR and RT) were analyzed, 11 (2.3%) sequences showed evidence of subtype divergence such as PRF/RTB and 5 (1%) sequences the profile PRB/RTF. Those divergent genomes together represented 37.2% of the total of the non-B HIV-1 analyzed samples. The subtype C was identified in two patients (0.4%) in the Rio de Janeiro, one from Niterói and the other from São Gonçalo municipal district. The circulating recombinant form CRF_02/AG virus was identified infecting one patient (0.2%) in the metropolitan area from Rio de Janeiro. The cumulative prevalence of non-B HIV-1 subtypes was 8.8% of the total of samples analyzed. The HIV-1 genotyping resistance profile associated to the ARV drug discriminated according to the subtype B and non-B infections are shown in Figs 2 and 3. Eight samples (1.5%) did not show any mutation associated to ARV resistance. The frequency of ARV mutations in the RT gene (Fig. 2) of HIV-1 positive individuals failing HAART was: M184V (67.7%), followed by T215Y/F (65.1%), M41L (53.2%), D67N (45.2%), L210W (37.2%), K70R (30.8%) and K219Q/E (27.3%). Overall, 35% of the individuals included in the present analysis showed an association to four NRTI resistance mutations (M184V, M41L, D67N, T215Y/F). The K103N NNRTI resistance-associated mutation was the most prevalent (27.7%), corresponding to more than 50% in the non-B viruses, followed by the mutations G190S/A (19.5%) and Y181C/I (15.8%), P225H (3.9%) and M230L in four patients (0.8%). The profile of resistance mutations associated to the protease gene (Fig. 3) was the minor mutations, L63P (72.4%), L10F/R (45.4%), M36I (36.3%), A71V (42.1%), V77I (40.9%). The most prevalent major mutation found among the ARV failing therapies was L90M (29.6%), followed by D30N, I54V and V82A, occurring in 20% of the patients. There was a clear association of the minor substitutions L63P and M36I with subtype assignment B and non-B, respectively. Moreover, differences on the frequency of drug resistance mutations analysis between B and non-B subtype viruses were observed for several positions of the protease and RT genes (Figs 2, 3). The resistance associated mutations identified in the two cases of HIV-1 subtype C infections were D67N + K70R + K103N + P225H in the RT gene and K20R + M36I + V82A for protease in one patient and, an insertion at 69 position + T69D and K219Q (RT), in association with the substitution M36I (PR) in the other C sample. On the other hand, the CRF_02A/G did not show any resistance associated mutation in RT genes and carried out only the minor mutations L10I and M36I in the protease gene. DISCUSSION Studies performed in developed countries and more recently in Brazil have demonstrated substantial benefits from the ARV treatment in terms of survival and quality of life for patients with AIDS (Detels et al. 2001, Marins et al. 2003). However, the development of drug resistance remains the most serious obstacle to maintain HAART therapy suppressing HIV replication in the infected patient (Vella 2002). Evidence suggesting the clinical utility of drug resistance testing is being accumulated from retrospective and prospective intervention-based studies (Durant et al. 1999). In addition, several clinical trials have showed a significant correlation between drug resistance and virologic response to a new treatment regimen when prior therapy has failed (Durant et al. 1999, Baxter et al. 2000, Cohen et al. 2002). In this molecular epidemiological survey performed in samples obtained from patients failing HAART in all of the Rio de Janeiro State, it was possible to detect a high prevalence of mutations related to drug resistance in RT and/or protease genes, as well as, estimate the prevalence of different genetic subtypes in the state. Our results are in accordance with previous molecular epidemiological studies in Brazil (Tanuri et al. 2002). A large proportion of HIV-1 subtype B infections was observed in HAART failing patients from Rio de Janeiro, higher than had been previously described for this subtype in the region (Morgado et al. 1998, Bongertz et al. 2000, Brindeiro et al. 2003). Indeed, we have found that almost 92% of the virus circulating in the state belongs to subtype B. These results would suggest the maintenance of a higher prevalence of HIV-1 subtype B even with the introduction of other non-B subtypes. Moreover, the prevalence of subtype F was quite low in the present study (4.9%), even including the B/F recombinant forms (8.1%). According to previous results of our laboratory (Morgado et al. 1998) and others (Brindeiro et al. 2003) the prevalence of this subtype in Rio de Janeiro varied around 15%, based on studies of drug naïve HIV-1 positive individuals within distinct exposure categories. If these differences could be attributed to differential HIV-1 subtype ARV-drug susceptibility has to be further addressed. Only in a very limited number of patients from the west part of the state a similar proportion of B and F subtype infections could be observed (Fig. 1). We detected two patients infected with subtype C and presented the first report of the circulation an African CRF_02 A/G recombinant form in Brazil. Actually, clade C-related viruses are the most prevalent subtype in the global AIDS epidemic and CRF_02A/G is the recombinant form more prevalent in African countries. In Brazil, we have detected an increased prevalence of subtype C in Brazilian southern-most states (Brindeiro et al. 2003), however, the impact of the new introduction of these African variants in low prevalence regions is totally unknown. Analyzing the resistance-associated mutations to RT inhibitors in all sequence samples, we observed that the M184V mutation was the most prevalent among B and non-B subtypes. This substitution is associated to an early virologic failure during ARV therapy concomitant with lamivudine (3TC) (Havlir et al. 2000) and its frequency is in agreement to what has been described for HIV patients failing HAART (Wainberg 2004). In addition, 3TC is used largely in Brazil due to its practicality and low toxicity, which might explain the finding of a high proportion of the M184V mutation in the HIV-1 samples studied (67.7% of the total). The second group of more prevalent RT mutations were the TAMs that lead to strong resistance against the majority of RTI, including Tenofovir. The RT mutation patterns between B and non-B subtypes were basically the same and varied only in the residues related to AZT resistance, which occurred more frequently in subtype B sequences. Among the NNRTI associated mutations, K103N and G190S/A were the most prevalent. Probably this is a consequence of the drug selective pressure in treated patients and also due to the large application of these classes of drugs in the Brazilian therapeutic protocols during the last years, mainly in association with 3TC. As for the two subtypes C identified one subject carried the insertion 69, leading to complete resistance to NTRI, and the other accumulated two TAMs (D67N, K70R) in association with the NNRTI mutations K103N and the P225H. Interestingly, both HIV-1 subtype C viruses were identified in the Niterói/São Gonçalo municipal districts, near the Rio de Janeiro metropolitan area, showing high demographic concentration. Concerning the recombinant form CRF_02A/G identified in the city of Rio de Janeiro, only minor mutations of the protease were detected. The circulation of non-B resistant subtypes may exercise a great impact in the AIDS epidemic in Rio the Janeiro, the second state in number of AIDS cases in the country (www.aids.gov.br/boletimepidemiologico 2003). Analyzing the genotyping resistance profile of the protease-associated mutations, many subtype associated differences could be detected only for the minor mutations, such as at residues, 20, 36, 63, 71, and 77 (Fig 3). The minor protease mutations M36I and L63P were associated to non-B and B subtypes, respectively. Such differences could lead to different levels of ARV resistance through different genetic barriers between B and non-B viruses and may influence of progression to resistance during therapy of HIV-1 (Brindeiro et al. 2002). One example of this possible situation was the identification of several minor IP mutations (K20M, M36I) in addition to V82A in the genome of the both HIV-1 subtype C and in the African recombinant form CRF_02A/G (L10I, M36I). In summary, association between HIV-1 subtypes and the different resistance mutation profiles associated to IP was clearly observed in the present study. All mutations detected by resistance genotyping analysis were related to the ARV therapy prescribed and 98.5% of the HIV-1 infected patients failing therapy presented several mutations in the viral genome associated to drug resistance. The selection and circulation of drug-resistant viruses may represent a serious public health problem and may compromise whole the Brazilian AIDS program efforts in controlling the HIV transmission and AIDS mobility/mortality by ARV therapy. The maintenance of resistance genotyping programs supplied for HIV-1 failing patients is important in the management of HAART therapies and to the attempted monitoring of the HIV-1 subtype prevalence in Brazil. ACKNOWLEDGMENTS To the genotyping reference doctor (MRG) staff from the Rio de Janeiro State Secretariat of Health for the patients recruitment, to Dr Josué Nazareno de Lima from National Program of STD and AIDS for the technical coordination and to Dr Vera Bongertz for reviewing the manuscript. REFERENCES
Copyright 2005 Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc05014f2.jpg] [oc05014f1.jpg] [oc05014f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}