 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memórias do Instituto Oswaldo Cruz, Vol. 100, No. 3, May 2005, pp. 269-272 Detection of hepatitis C virus RNA by in situ hybridization in paraformaldehyde fixed biopsies H.S. Carvalho/+, M.L. Baptista, M.A. Pinto, M. Silva, C.M. Takiya*, V. Chagas**, V. Pannain**, H.S.M. Coelho***, CFT Yoshida Departamento de Virologia, Instituto Oswaldo Cruz-Fiocruz, Av. Brasil 4365, 21045-900 Rio de Janeiro, RJ, Brasil *Departamento de Histologia, CCS/UFRJ, Rio de Janeiro, RJ, Brasil **Departamento de Patologia, Serviço de Anatomia Patológica ***Departamento de Clinica Médica, Setor de Gastroenterologia, Hospital Universitário Clementino Fraga Filho, UFRJ, Rio de Janeiro, RJ, Brasil Financial support: Faperj, CNPq Received 6 December
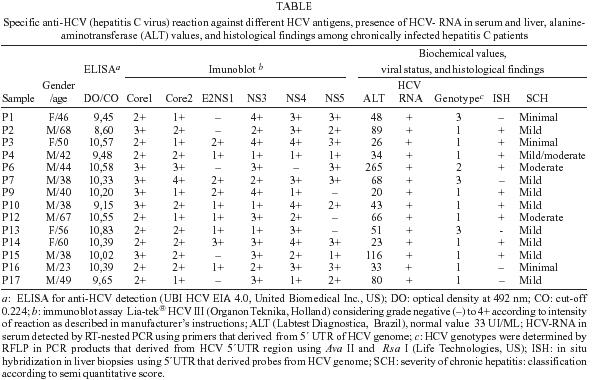
2004 Code number: oc05081 Fourteen hepatitis C virus (HCV) chronically infected patients were submitted to routine liver biopsy for histological evaluation. Liver samples were assayed to HCV-RNA by in situ hybridization, using digoxigenin labeled probe. HCV genotypes were found to be predominantly type 1 (71.4%), followed by genotype 3 (21.4%), and genotype 2 (7.2%). Alanine-aminotransferase levels were raised in 10 patients. The histopathological scores were minimal (21.4%), mild (57.2%), and moderate (21.4%). Viral RNA was detected in liver cells from nine patients (64.3%). ISH method provides localization and poor confirmation of HCV RNA in the liver tissue of HCV chronic patients. Key words: hepatitis C virus RNA - in situ hybridization - liver biopsy - chronic hepatitis - viral hepatitis In situ hybridization (ISH) technique was initially introduced in 1969 (John et al. 1969, Pardue & Gall 1969) for the localization of DNA sequences, after 20 years Macville described non-radioactive protocol to detect mRNA transcripts in different tissues (Macville et al. 1995). Currently the diagnosis is based on specific antibody detection (anti-hepatitis C virus anti-HCV) in serum and several nucleic acid-based technology are undertaken to detect the prevalence of circulating virus genome (Schiff et al. 1999). The detection of virus genome and viral protein in liver sections, is an additional diagnostic procedure (Walker et al. 1998). Nevertheless, the detection and exact localization of the HCV genome in the liver and in the other tissues may have a key role to understanding the pathogenesis and natural history of HCV infection (Qian et al. 2004). The aim of the present study was to establish a method for HCV RNA detection using in situ molecular hybridization in liver biopsies of chronically infected patients. Moreover, we investigated possible correlation between the presence of HCV in liver and histological, biochemical, serological, and molecular information. In this work, 14 HCV chronically infected patients (10 male and 4 female) who attended at the Liver Clinic, Hospital Universitário Clementino Fraga Filho/Federal University of Rio de Janeiro (RJ, Brazil) were investigated, which they were submitted to liver biopsies before starting antiviral therapy. All individuals were known to be positive for anti-HCV antibodies and for HCV RNA in serum. The mean age of male patients was 45 (± 13.7) years and of female patients was 53 (± 6.2) years. Exclusion criteria included the presence of coagulation disorders, HIV seropositivity, co-infection of hepatitis B and D virus, autoimmune hepatitis, alcoholic liver disease or any kind of drug use. The procedures protocol was submitted to the Human Research Committee of the Federal University of Rio de Janeiro and reviewed by the Institutional Reviewer Board. Liver specimens were divided in two samples: one for histological evaluation, which was fixed in 10% buffered formalin, and the other, designated to the ISH, was fixed in 4% paraformaldehyde/PBS. Both fragments were included in paraffin further, sectioned into 4 µm thickness pieces and fixed on silane-coated slides. The criteria adopted to determine the histological activity index was previously described (Ishak et al. 1995). Peripheral blood (10 ml) was collected from each patient to evaluate the biochemical liver function and also to confirm HCV serological and molecular status at the moment of the liver biopsy. Anti-HCV was tested using enzyme immunoassay UBI® HCV-EIA 4,0 (United Biochemical Inc., US). Supplemental testing was also carried out using an im-munoblot assay, Lia-Tek® HCV III (Organon Teknika, Holland). Alanine aminotrasferase (ALT) was assayed using a colorimetric procedure (Labtest Diagnostica, Brazil) and the upper normal threshold was 33 UI/ml. HCV-RNA was detected in sera samples using an RT-nested PCR, with primers derived from 5´ non-coding region of HCV genome. HCV genotyping was performed by restriction fragment length polymorphism analysis (RFLP) and identified according to Simmonds' classification (Simmonds et al. 1993). For ISH, probe was obtained by extraction of HCV RNA from serum samples of each patient (Quiagen) following for cDNA syntesis, using a negative-sense primer 5´ UTR HCV region (5´ ggT gCA Cgg TCT Acg AgA CC 3´). After cDNA was amplified by nested PCR using a set 18 to 36 (5´ ggC gAC ACT CCA CCA TRR AT 3´) and anti-sense synthetic oligonucleotides, 322 to 343 (5´ ggT gCA Cgg TCT Acg AgA CC 3´). For the nested PCR inner primers were: sense, 38 to 57 (5´ ACC ATR RAT CAC TCC CCT gT 3´) and antisense, 288 to 308 (5´ CAA gCA CCC TAT Cag gCA T 3´). The PCR consisted of 30-s denaturation step (94°C), a 1-min annealing step (72°C). Both PCR procedures were similar, except for the 25 consecutives cycles used in the nested. The amplified DNA was labeled with digoxigenin dNTPs during the nested PCR and the efficiency of this procedure confirmed by dot blot hybridization. The liver sections were deparaffinized in xylene and rehydrated in alcohol series. The optimal condition for the enzymatic digestion of liver sections was the use of proteinase K at concentration of 40 µg/ml in Tris-HCl pH 8.0, 1 mM EDTA (TE), followed by an incubation of 20 min at 37°C (Lau & Davis 1994). Liver sections were then washed with sterile water and a second fixation was carried out in a 4% paraformaldehyde/PBS for 5 min. After dehydration, sections were immersed into a solution containing 0.25% acetic anhydrous and 0.1M triethane (pH 8.0), during 10 min. Finally, sections were incubated in a pre-hybridization solution (5 × SSC; 1 × Denhardt's solution; 10% dextran sulfate; 1 mg/ml herring sperm DNA (Roche); 300 mM DTT; 0.05 M Tris; 5 mM EDTA; 600 mM NaCl, 50% deionized formamide and 0.1% NaCl). Each liver biopsy was, then, hybridized with its respective blood derived HCV probe. Hybridization was performed using probe in a pre-hybridization solution. The probes were previously heated at 95°C for 5-10 min and submitted to a fast cooling on ice. Then the liver sections were incubated with hibridization solution. Distincts hybridization temperatures (37, 39, 42, and 45°C) and probe concentrations (0,5 and 1 µg/ml) were tested on liver sections. The most consistent results were found with 0,5 µg/ml of the hybridization buffer at 42°C overnight. After hibridization, stringent washings eliminated nonspecific binding. Different conditions of concentration and periods of incubation were tested. The best were 2× SSC/30% formamide twice for 10 min and 1× SSC twice for 10 min. Immunodetection method was carried out following the manufacturer's instructions (DIG DNA Labeling and Detection Roche, US). Labeling was performed with the substrate nitroblue tetrazolium (NBT-BCIP- Roche, US). The sections were washed with water and counterstained using methyl green. The image capture of ISH in liver sections was obtained by Leitz Dialux microscope. The images were acquired using a video camera-Sony XC-003P > 52 (H X582/V) Leica DMRXA Leica QWIN standard. Liver biopsies from patients chronically infected with hepatitis B virus (HBV) were used as negative tissue controls. A specific probe for dengue virus also was used for checking the specificity and, finally, pre-hybridization solution without probes was also used, in order to exclude the possibility of non-specific reaction. A status compatible with chronic hepatitis C infection for 14 patients was investigated. The Table shows the results for anti-HCV against different HCV antigens, HCV-RNA in serum and liver, the genotypes of HCV, ALT levels and histological finding of these patients. ALT levels were normal in 4 patients, altered from 34 to 89 UI/ML in 8 patients and above 100 UI/ML in 2 patients. HCV RNA was detected in all serum samples. Genotyping by RFLP was performed in all of them, showing a high percentage of HCV genotype 1 (71.4%), followed by genotype 3 (21.4%), and genotype 2 (7.2%). The necroinflammatory activity was detected in all liver sections, ranging from minimal to moderate score, however, with no incidence of liver fibrosis or cirrhosis. HCV genome was identified in 9 out of 14 patients (64.2%). The viral genome was detected in isolated cells as hepatocytes, mononuclear, Kupffer, and sinusoidal cells by optical microscopy. However, HCV RNA was present in a lower frequency. The localization of ISH signals was citoplasmatic or perinuclear (Figure). The positive sinusoidal and mononuclear cells was scatter distributed in the lobule, most of them citoplasmatic and rarely associated with necroinflamatory lesions, as described by some authors (Walker et al. 1998). Comparing results between HCV-RNA detection in serum and liver by RT-PCR and ISH, respectively, a lower sensitivity of the second method was observed. This could be expected since ISH does not include amplification of viral genome. The limit of tissue HCV RNA detection estimated by cell culture assay was 14 ± 2 genomic equivalents of HCV positive strand per cell (Agnello et al. 1998) or by quantitative PCR, being about 50 genome copies per cell (Höfler 1990). Also, it must be considered the possibility of RNA damage during the several tissue-processing steps (Guerrero et al. 1997). In our protocol, ISH technique allowed detection, in average, of 1 to 4 strong positive fields per liver section, which corresponds to 3 to 4 portal tracts. Rodrigues-Iñigo et al. (1994) reported the percentage ranging from 0.04% to 83.3%. Furthermore, the frequency of infected cells seems to be correlated with circulating viral load as described in post-transplant recurrent viral hepatitis (Nuovo et al. 2002). The difference between these findings and ours could be attributed to different profile of host intra-hepatic immune response among the studied population (Thimme et al. 2002). We observed variations in levels of ALT among our patients, still we could not find any relation between ISH and semi quantitative Ishak's score. Indeed, ALT levels below upper limit of normal range can be found in our patients. On the other hand, elevated levels of ALT can also be observed in patients even in the absence of HCV-RNA in liver (Morimoto et al. 1997). The low concentration of HCV RNA has been described in liver parenchyma, suggesting that persistent infection may be caused by low levels of HCV replication, as observed in both hepatoma cells and in non-cancerous hepatocytes from patients with HCC (Agnello et al. 1998, Ohishi et al. 1999). Furthermore our results show a low frequency of HCV-RNA detected in cells, besides the different patterns of ALT levels and a weak degree of necroinflamatory activity suggest altogether that HCV cytopathic effect if present, would not be strong enough to kill hepatocytes (Fanning et al. 2001). HCV RNA detected by ISH was found in 8 out of 10 patients with samples of genotype 1, in only one case of genotype 2 and in none of the 3 patients of genotype 3. Our findings were in accordance with previous report on pattern of intra-hepatic viral replication among chronic hepatitis patients. In subjects infected with HCV genotype 3, the hepatic viral load seems to be lower than the other genotypes (Castillo et al. 2004). The principal advantage of ISH method consists in demonstrating the viral presence in a target organ mainly in long-standing abnormal results of liver function patients (ALF-EU). Castillo et al. using ISH in formalin fixed biopsies described occult HCV infection in 57 out of 100 patients with elevated liver enzyme levels, who were seronegative for anti-HCV antibodies and for HCV RNA (Morimoto et al. 1997). The association between histological index activity, serological markers, serum, and liver HCV RNA content could be used to assess the effectiveness of antiviral treatment in chronic hepatitis C (Arrojo et al. 2003) providing a solid basis for diagnosis and control of patients under antiviral therapy. Finally, ISH performed following the technique described here constitutes a reliable method of HCV detection and localization of HCV in tissue, since it allows identification of specific regions of the viral genome with high confidence. In this study ISH was less sensitive than HCV-RNA detection in serum by PCR, in such way that it could not be used as an isolated marker in the molecular diagnosis of HCV. However it may be an important investigative tool to study "serosilent" HCV infection in cryptogenic cases of liver disease as described in blood donors (George et al. 2002), HIV positive individuals (Bassett et al. 1998) and also reported in chimpanzees experimentally HCV infected (Ishak et al. 1995). Further studies, comprising a larger sample are under development in order to assess possible association between the presence of HCV-RNA in liver and clinical manifestations, histopathological status, viral genotypes, and even in patients without evidence of circulating HCV. ACKNOWLEDGMENTS To Dr Renato S Marchevsky (Laboratório de Neuroviru-lência, Bio-Manguinhos-Fiocruz) for preparing the images of in situ hibridization, Dr Marize Miagostovitch (Laboratório de Flavivírus, Departamento de Virologia, IOC-Fiocruz) for having kindly donated the dengue probes. REFERENCES
The following images related to this document are available:Photo images[oc05081f1.jpg] [oc05081t1.jpg] |
| |||||||||

{kind=link}
{kind=link}