 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memórias do Instituto
Oswaldo Cruz, Vol. 100, No. 4, July 2005, pp.
345-349 Megmar AS Carneiro, Sheila A Teles*, Márcia A Dias, Renata C Ferreira, Alessandra V Naghettine**, Simonne A Silva, Elisabeth Lampe***, Clara FT Yoshida***, Regina MB Martins/+ Instituto de Patologia
Tropical e Saúde Pública, *Faculdade de Enfermagem **Faculdade
de Medicina, Universidade Federal de Goiás, Caixa Postal 131, 74605-050
Goiânia, GO, Brasil ***Departamento de Virologia, Instituto Oswaldo
Cruz-Fiocruz, Rio de Janeiro, RJ, Brasil Received 2 December
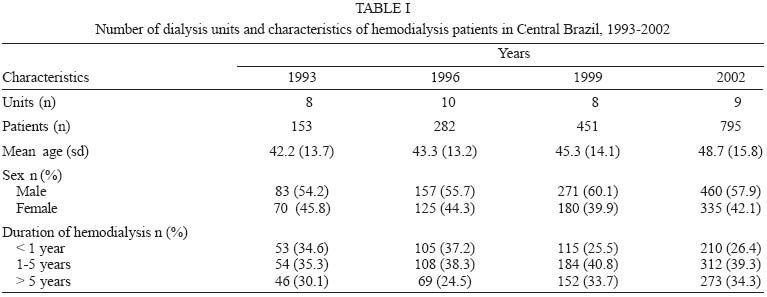
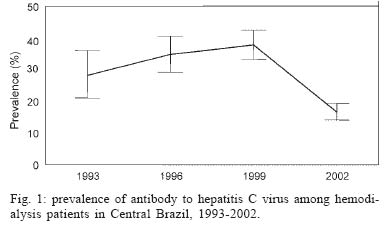
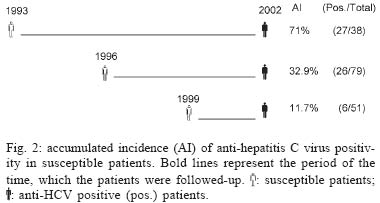
2004 Code Number: oc05095 Hepatitis C virus (HCV) has been a significant problem for hemodialysis patients. However this infection has declined in regions where the screening for anti-HCV in blood banks and hemodialysis-specific infection control measures were adopted. In Brazil, these measures were implemented in 1993 and 1996, respectively. In addition, all studied units have implemented isolation of anti-HCV positive patients since 2000. In order to evaluate the impact of these policies in the HCV infection prevalence, accumulated incidence, and risk factors in hemodialysis population of Goiânia City, Central Brazil, all patients were interviewed and serum samples tested for HCV antibodies in 1993, 1996, 1999, and 2002. In the first six years (1993-1999), anti-HCV prevalence increased from 28.2 to 37.2%, however a strong decrease in positivity was detected between 1999 and 2002 (37.8 vs 16.5%) when the measures were fully implemented. Also, a decrease of the anti-HCV accumulated incidence in cohorts of susceptible individuals during 1993-2002 (71%), 1996-2002 (34.2%), and 1999-2002 (11.7%) was found. Analysis of risk factors showed that length of time on hemodialysis, blood transfusion before screening for anti-HCV and treatment in multiple units were statistically associated with anti-HCV (p < 0.05). Our study showed a significant decline of hepatitis C infection in hemodialysis patients of Central Brazil, ratifying the importance of public health strategies for control and prevention of hepatitis C in the hemodialysis units. Key words: hepatitis C - hemodialysis - prevalence - incidence - risk factors - Central Brazil Hepatitis C virus (HCV) infects more than 170 million of people worldwide. This virus is a common cause of chronic liver diseases, including cirrhosis and hepatocellular carcinoma, both of which are associated with significant morbidity and mortality (Lauer & Walker 2001, Alberti & Benvegnu 2003, Poynard et al. 2003). HCV is efficiently transmitted by parenteral route. Therefore hemodialysis patients are at high risk of acquiring hepatitis C, because of the frequent past blood transfusion and regular vascular access (CDC 2001). In addition, HCV infected hemodialysis patients have an increased risk of death when compared with those not infected (Stehamn-Breen et al. 1998, Fabrizi et al. 2002). The prevalence of HCV infection in hemodialysis patients is usually greater than that found in general population (Fabrizi et al. 2002). On the other way, a high variability in the HCV positivity rates has been found in individuals undergoing hemodialysis, ranging from 3.4% in patients of Netherlands (Schneeberger et al. 2000), to more than 70% in Eastern Europe (Vladutiu et al. 2000). In Brazil, prevalence rates varying from 13% (Souza et al. 2003) to 64.7% (Vanderborght et al. 1995) have been reported. The screening of anti-HCV in blood banks and the adoption of hemodialysis-specific infection control measures have been implicated in the declining of HCV infection in hemodialysis patients (Djordjevic et al. 2000, Almoroth et al. 2002, Valtuille et al. 2002). In our country, the first measure has been implemented since November 1993, and the latter in the end of 1996 in compliance with news Health Ministry Standards for Renal units which are in accordance with most of Centers for Disease Control and Prevention (CDC 2001) recommendations. In this study, HCV infection prevalence, accumulated incidence, and risk factors were analyzed to evaluate the impact of these policies on the control of this infection in hemodialysis units in Central Brazil. MATERIALS AND METHODS Subjects - The study was carried out between 1993 and 2002 in all hemodialysis units from Goiânia city, Central Brazil (1,200,000 inhabitants), an intermediate endemicity area for hepatitis C infection (Martins et al. 1994). The characteristics of the patients are shown on Table I. During the survey period, all subjects received treatment three times a week and they were distributed in three shifts. Hemodialysis has been performed with bicarbonate and cuprophane or polysulphone dialyzers. These and bloodlines were disinfected and reused by the same patient. Hemodialysis machines were disinfected at the end of the day, and environmental surfaces after each session. Until 1996, almost all units had machines with a dialysis solution central delivery system, instruments and supplies as scissors, blood pressure cuffs and thermometer were shared between patients, and blood precautions were poorly compliance with. In 1996, as consequence of new Health Ministry Standards for Renal Units (Ministério da Saúde 1996), modern equipments with disinfection programs were acquired and the infection control measures recommended were adopted in our units, including strategies such as monthly screening for anti-HCV of susceptible patients and separate room for reprocessing of HCV-positive patients dialysers. Since 2000, hemodialysis patients have used routinely recombinant human erythropoietin (rHuEPO) (Ministério da Saúde 2000). In addition, anti-HCV positive individuals have been dialysed in the last shift or in a dedicated area in all studied units. All patients were interviewed for risk factors to HCV infection. A standardized form was used to collect data on age, sex, blood transfusion before November 1993 (mandatory screening for anti-HCV in blood banks), acupuncture, tattooing, illicit drug abuse, sexually transmitted diseases, multiple partners, length of time on hemodialysis, and treatment in multiple units. The protocol used in the present study was approved by Ethical Committee of the Federal University of Goiás. Details of the study were explained to all eligible participants and informed consent was obtained prior to subject enrollment. Serological tests - Blood samples were collected from all patients and sera were stored at -20ºC. Serum samples were tested with a third generation enzyme immunoassay method (HBK 520 HEMOBIO HCV, Embrabio). Positive samples were retested for confirmation using line immunoassay (INNO-LIA HCV Ab III, Innogenetics). Statistical analysis - Prevalence, incidence, odds ratios, p values and 95% confidence intervals (CI) were calculated. Statistical significance was assessed at 0.05 probability level in all analysis. Variables statistically significant with anti-HCV positivity (p < 0.05) were entered into multivariate model (Epiinfo, version 2000 package, developed by the CDC, Atlanta, GA). RESULTS The Fig. 1 shows the prevalence of anti-HCV among hemodialysis patients in Central Brazil along ten years. In 1993, 28.2% (95% CI: 21.4-35.8) of the patients had anti-HCV antibodies, and three years later, this increased to 34.7% (95% CI: 29.36-40.4%) remaining high until 1999 (37.8% 95% CI: 33.3-42.4%), when a significant decrease was observed reaching 16.5% (95% CI: 14.2-19.4) in the end of the study. One hundred sixty eight susceptible patients were followed-up along the investigation: 38 for nine years (1993-2002), 79 for six years (1996-2002), and 51 for three years (1999-2002). These subjects presented an anti-HCV accumulated incidence of 71% (27/38), 32.9% (26/79) and 11.7% (6/51), respectively (Fig. 2). Analysis of risk factors showed that, in 1993, only length of time on hemodialysis was significantly associated with HCV positivity (p < 0.01, data not shown). Blood transfusion before screening for anti-HCV, length of time on hemodialysis, and treatment in multiple units were statistically associated with HCV infection in 1996, 1999, and 2002 by univariate analysis (p < 0.01). Thus, these variables were included in the multivariate logistic regression model (Table II). Patients who received blood transfusion before screening for anti-HCV were more likely to be HCV positive than those transfused after this measure: in 1996, an adjusted odds ratio (AOR) of 7.3 was found (95% CI: 3.4-15.7; p < 0.01), which declined for 5.6 (95% CI: 3.0-10.1; p < 0.01), and 3.5 (95% CI: 2.0-6.0; p < 0.01) in 1999 and 2002, respectively. Individuals on hemodialysis treatment for more than five years had a 14.3-fold (95% CI: 6.0-33.8), 11.4-fold (95% CI: 4.1-31.1), and 24.6-fold (95% CI: 13.0-46.3) greater chance of acquiring hepatitis C compared to those treated less than one year in 1996, 1999, and 2002, respectively. Regarding treatment in multiple units, only in 1996 this variable was independently associated to HCV (AOR = 2.8; 95% CI: 1.5-5.3). DISCUSSION Epidemiological studies have been useful to evaluate the efficiency of public health strategies on hemodialysis population. In the first three years of the study, the increased proportion of anti-HCV positive patients reflected the absence of these policies for prevention of hepatitis C in hemodialysis units, which could be responsible for the high HCV prevalence until 1999. After 1996, as consequence of the new rules, all units were improved regarding area, equipment, and staff. Thus, these strategies should have contributed for the findings showed at the end of the survey period when a significant decrease of HCV infection prevalence (37.8 vs 16.5%) was observed. Also, the decline of the accumulated incidences in the cohorts of susceptible individuals during 1993-2002 (71%), 1996-2002 (34.2%), and 1999-2002 (11.7%) periods reinforces this assumption. Epidemiological and molecular studies have shown the role of the hemodialysis environment for dissemination of HCV between patients (Djordjevic et al. 2000, Schneeberger et al. 2000, Almoroth et al. 2002, Bdour 2002, Furusyo et al. 2004, Sartor et al. 2004). In our investigation, length of time on hemodialysis was independently associated with anti-HCV positivity in all period investigated. In 1996 and 1999, the adjusted odds for individuals undergoing hemodialysis for more than five years reached 14.3 (95% CI: 6.0-33.8) and 11.4 (95% CI: 4.1-31.1), respectively, and it increased for 24.6 (95% CI: 13.0-46.3) in 2002 when a high concentration of anti-HCV positive patients on treatment for a long time was observed. These patients had been treated before and during the policy changes occurred in our units, when the infection control measures were not in completely compliance yet. Breakdown in infection-control measures such as sharing of equipment, devices or multidose vial between patients have been reported as cause of viral dissemination (Bronowicki et al. 1997, Lagging et al. 2002, Krause et al. 2003). Piazza et al. (1994) showed that HCV RNA was resistant to drying at room temperature for at least 48 h. In addition, recently Froio et al. (2003) detected it on a hemodialysis machine used for HCV-negative patients, suggesting the importance of the environmental contamination of surfaces for HCV transmission. Also it was not unusual to find staff taking care of susceptible and infected patients in the same shift. Additionally, they did not routinely discard gloves after use. This practice may facilitate the dissemination of HCV between hemodialysis patients, since HCV RNA was found on the hands of dialysis personnel (Alfurayh et al. 2000). In units with high HCV positivity and low personnel/patient ratio (Petrosillo et al. 2001), as found in some Brazilian public and private health services, this negligent practice should amplify the chances of contamination. Some authors have appointed dialysis in multiple centers as a risk factor for HCV infection (Schneeberger et al. 2000, Busek et al. 2002). In this study, there was a significant association between treatment in different units and hepatitis C in 1996. It was expected since in this period, some units, where poor compliance with infection control practices was observed, were permanently or temporarily closed. As observed by others (Djordjevic et al. 2000, Vladutiu et al. 2000, Bdour 2002, Valtuille et al. 2002), in this investigation, blood transfusion before screening for anti-HCV was associated with hepatitis C. However, the probability of HCV positivity in individuals that received blood before this measure declined from 7.3 (95% CI: 3.4-15.7) in 1996 to 3.5 (95% CI: 2.0-6.0) in 2002. In the past, hemodialysis patients also acquired HCV infection by transfusion of infectious blood (CDC 2001). In Brazil, this is now a rare event because all blood units have been screened for anti-HCV. In fact, the residual risk for hepatitis C dropped dramatically after 1996 when the third generation ELISA was introduced in the screening for anti-HCV in blood banks (Kupek 2001). In summary, our study showed a significant decline of hepatitis C infection among end-stage renal disease patients in Central Brazil, ratifying the importance of public health strategies such as screening for anti-HCV in blood banks and infection control measures for control and prevention of hepatitis C in the hemodialysis environment. Regarding the isolation of hepatitis C patients, some authors have also recommended this measure in hemodialysis setting (dos Santos et al. 1996, Barril & Traver 2003, Saxena et al. 2003), although this is not universally accepted (CDC 2001, Valtuille et al. 2002, Froio et al. 2003). Further studies will be necessary to elucidate the real role of this strategy in our dialysis population. ACKNOWLEDGEMENTS To Dr André Kipnis for reviewing the manuscript. We dedicate this article to the patients and staff of the hemodialysis units of Goiânia City. REFERENCES
The following images related to this document are available:Photo images[oc05095t1.jpg] [oc05095f2.jpg] [oc05095f1.jpg] [oc05095t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}