 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memórias do Instituto Oswaldo Cruz, Vol. 100, No. 4, July 2005, pp. 451-455 Effects of antifolates - co-trimoxazole and pyrimethamine-sulfadoxine - on gametocytes in children with acute, symptomatic, uncomplicated, Plasmodium falciparum malaria A Sowunmi/+, BA Fateye, AA Adedeji, FA Fehintola, AE Bamgboye, CP Babalola*, TC Happi, GO Gbotosho Department of Pharmacology & Therapeutics and Institute for Medical Research and Training *Department of Pharmaceutical Chemistry, University of Ibadan, Ibadan, Nigeria Financial support:
the UNDP/World Bank/WHO Special Programme for TDR. AS was supported by a
WHO/TDR Career Development Grant.| Received 24 January
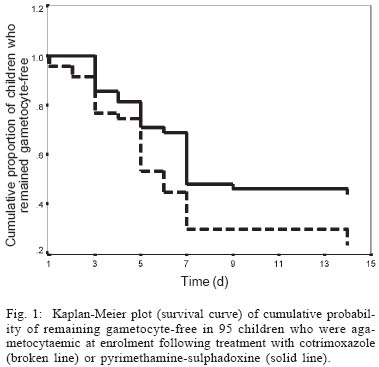
2005 Code Number: oc05112 Antimalarial drugs including the antifolate, pyrimethamine-sulfadoxine (PS), can modulate the prevalence and intensities of gametocytaemia following treatment of acute malaria infections. They may also directly influence the transmission and spread of drug insensitivity. Little is known of the effects of co-trimoxazole (Co-T), another antifolate antimalarial, on gametocytes in children with acute malaria infections. We compared the effects of Co-T and PS on the prevalence and intensities of gametocytaemia and gametocyte sex ratios in 102 children aged 0.5-12 years presenting with acute and uncomplicated falciparum malaria. Compared to pre-treatment, both drugs significantly increased gametocyte carriage post-initiation of treatment. However, gametocyte carriage was significantly lower on day 14 in those treated with Co-T than PS. Significant increase in gametocytaemia with time occurred in PS - but not Co-T-treated children. Kaplan-Meier survival curve of the cumulative probability of remaining gametocyte-free in children who were agametocytaemic at enrolment showed that by day 7 of follow up, children treated with PS had a significantly higher propensity to have developed gametocytes than in Co-T-treated children (Log-rank statistic 5.35, df = 1, P = 0.02). Gametocyte sex ratio changes were similar following treatment with both drugs. PS and Co-T treatment of acute malaria infections in children from this endemic area is associated with significant increases in prevalence and intensities of gametocytaemia but these effects are more marked in those treated with PS than Co-T. Key words: co-trimoxazole - pyrimethamine-sulfadoxine - malaria - gametocytaemia - sex ratio - children - Nigeria The antifolate antimalarial, pyrimethamine-sulfadoxine (PS), has become increasingly used as first line treatment of falciparum malaria in several African countries because of increasing resistance in Plasmodium falciparum to chloroquine. In spite of frequent use and of in vivo and in vitro studies (Hogh et al. 1998, Sowunmi & Fateye 2003a), its effects on gametocytes in children with falciparum infections remain incompletely understood. With increasing use, resistance in P. falciparum to PS is increasing (Sibley et al. 2001) probably as a consequence of long half lives of its components. It has recently been suggested that, co-trimoxazole (Co-T), an antifolate antimalarial with relatively short half-lives of its components compared to PS, may be used as alternative to the latter for the treatment of uncomplicated falciparum infections in children because it is as efficacious as PS (Omar et al. 2001, Fehintola et al. 2004). It is assumed that the relatively short half-life of Co-T may, when compared with PS, reduce the chances of engendering resistance in P. falciparum to this drug and may provide additional advantage with transmission of drug resistant infections over PS. It is noteworthy that antifolate antimalarials are not effective in the treatment of uncomplicated falciparum malaria in South America, for example, Brazil (Fontes et al. 2002). However, while the effects on PS on gametocytes and gametocyte sex ratios (GSR) are known (GSR may influence infectivity to mosquitoes and transmission _ see Robert et al. 1996, Sowunmi et al. 2003 a,b), the effects of Co-T on gametocytes are relatively unknown in African children with falciparum malaria. We hypothesized that PS and Co-T have similar effects on gametocyte prevalence, density, and sex ratio, and possess similar effects on gametocyte survival in children treated with these drugs. We tested this hypothesis in a group of children with acute symptomatic uncomplicated P. falciparum malaria who were randomized to and who received PS and Co-T for the treatment of their infections. PATIENTS AND METHODS Patients - Between June and August 1999, a randomized trial of Co-T and PS for the treatment of uncomplicated falciparum malaria was conducted in 102 children at the University College Hospital in Ibadan, a hyperendemic area for malaria in Southwestern Nigeria (Salako et al. 1990). Ethical clearance for the study was provided by the local ethics committee. In general, to be enrolled, the children had to be aged 0.5-12 years, and have symptoms compatible with acute, falciparum malaria (with fever or history of fever in the 24-48 h preceding presentation) and a pure P. falciparum parasitaemia of > 2000 asexual forms/µl blood. Those who had taken antimalarial drugs in the two weeks preceding presentation, provided a urine sample found positive for four aminoquinolines or sulphonamides (by the Dill-Glazko and lignin tests, respectively), or who had a concomitant illness, such as sickle-cell anaemia, or severe or complicated malaria (WHO 2000) were excluded. The informed consent of a parent or guardian was obtained for each child included in the study. A child was withdrawn from the study if she/he developed concomitant illness during the follow-up period, or if his/her parent or guardian requested it. Thick and thin blood films from all patients who participated in the study were examined for the presence and density of asexual and sexual parasites at enrolment and start of treatment (day 0), and at follow-up at days 1-7, and then on day 14. Co-T was given as 20 mg/kg of the sulfamethoxazole component twice daily for five days (day 0-4); PS was given as the 25 mg/kg of the sulfadoxine component at presentation (day 0). All drugs were administered orally. Assessment of parasitaemia and gametocyte sex ratio - Thick and thin blood films prepared from a finger prick were Giemsa-stained and were examined by light microscopy under an oil-immersion objective, at × 1000 magnification, by two independent assessors who did not know the drug treatment of the patients. Parasitaemia in thick films was estimated by counting asexual parasites relative to 1000 leukocytes, or 500 asexual forms, whichever occurred first. From this figure, the parasite density was calculated assuming an average leukocyte count of 6000/µl of blood (Shaper & Lewis 1971, Ezeilo 1971, Sowunmi et al. 1995). Gametocytes were also counted in thick films against 1000 leukocytes assuming an average leukocyte count of 6000/µl of blood at enrolment (day 0) and on days 3, 5, 7, and 14. Gametocytes were sexed, in thick blood film, if gametocytaemia was > 12 sexual forms/µl. Gametocyte sex determination was based on the following criteria (Carter & Graves 1988, Robert et al. 1996): males are smaller than females; the nucleus is bigger in males than females; the ends of the cells are round in males and angular in females; the cytoplasm stains pale purple in males and deep blue in females; and the granules of malaria pigment are centrally located in females and more widely scattered in males. GSR was defined as the proportion of gametocytes in peripheral blood that were microgametocytes (Pickering et al. 2000, West et al. 2001). Statistical analysis - Data were analysed using version 6 of the Epi-Info software (Anon 1994), and the statistical program SPSS for Windows version 10.01 (SPSS 1999). Proportions were compared by calculating χ2 with Yates' correction or Fisher exact test. Normally distributed, continuous data were compared by Student's t-tests and analysis of variance (ANOVA). Data not conforming to a normal distribution were compared by the Mann-Whitney U-test and the Kruskal-Wallis test (or by Wilcoxon rank sum test). Kaplan-Meier analysis was used to estimate the cumulative probability of remaining free of gametocytes during follow-up for all cases of malaria combined and for those cases that were free of gametocytaemia at enrolment. Differences in survival time were assessed by inspection of Kaplan-Meier curves and pairwise log-rank tests. P-values of < 0.05 were taken to indicate significant differences. RESULTS Demographic characteristics and therapeutic responses - A total of 104 children were enrolled into the study. Two children, one in each treatment group, were excluded from the study due to parental relocation. These children were cleared of their peripheral parasitaemia at the time of exclusion. The demographic characteristics of the children enrolled in the study and the therapeutic responses to the treatment given are summarized in Table I. These were similar in the two treatment groups. However, parasite clearance was significantly shorter in those treated with Co-T than PS. Prevalence of gametocytaemia - The prevalence of gametocytaemia before and after treatment with PS, and before, during and after treatment with Co-T is shown in Table II. Gametocyte carriage was similar on days 0-7 in both treatment groups and it peaked at day 7 in both the PS and Co-T groups. Gametocyte carriage was significantly lower on day 14 in those treated with Co-T than PS (χ2 = 5.6, P = 0.018). Eleven and 19 children treated with Co-T and PS, respectively were gametocyte carriers on both days 7 and 14. The difference between these proportions was significant (χ2 = 4.0, P = 0.046). In general, compared to pre-treatment, both drugs significantly increased gametocyte carriage post-initiation of treatment (χ2 = 20.9, P = 0.003 for Co-T and χ2 = 28.4, P = 0.0001 for PS, see Table II). In children without patent gametocytaemia at enrolment, there was a greater propensity to be gametocyte-positive by day 7 with a significantly greater proportion of children treated with PS having gametocytes by day 14 of follow up compared with Co-T (63.6% vs 34.3%, χ2 =5.9, P = 0.016) (Table II). Gametocytaemia - Gametocytaemia before and after treatment with PS, and before, during and after treatment with Co-T is shown in Table II. Gametocytaemia was similar throughout the duration of the study in both Co-T and PS-treated children with peak gametocytaemia occurring in both treatment groups on day 7. Peak gametocytaemia (on day 7) was significantly higher than day 3 game-tocytaemia in both treatment groups (t = 0.066, P = 0.018 for Co-T; t = 0.08, P = 0.017, by Wilcoxon sign rank test for paired data). Gametocytaemias occurring on days 3-14 were not compared with pre-treatment gametocytaemia because of the small number of patients in both groups. However, multiple comparison of gametocytaemia using Friedman test showed that there was significant increase in gametocytaema with time on days 3, 5, 7, and 14 in those treated with PS (P = 0.011). In comparison, there was no significant increase in gametocytaemia with time on days 3, 5, 7, and 14 in those treated with Co-T (P = 0.29). The Kaplan-Meier survival curve of the cumulative probability of remaining gametocyte-free in children who were agametocytaemic at enrolment is shown in Fig. 1. By day 7 of follow up, children treated with PS had a significantly higher propensity to have developed gametocytes than in Co-T-treated children (Log-rank statistic 5.35, df = 1, P = 0.02). Temporal changes in gametocyte sex ratios - In Co-T-treated children, 7, 28, 104, 134, and 44 gametocytes were counted on days 0, 3, 5, 7, and 14, respectively and approximately 77% of these gametocytes could be sexed. In PS-treated children, 7, 34, 230, 293, and 168 gametocytes were counted on days 0, 3, 5, 7, and 14, respectively and approximately 76% of these gametocytes could be sexed. The data on GSR at enrolment were pooled because of the small number of gametocyte carriers observed pre-treatment (three among Co-T-treated children and two among PS-treated children). Overall, pre-treatment GSR was female-biased, but became male-biased by day 3 in both treatment groups, and remained male-biased till day 14 in both groups (Fig. 2). GSR was similar in the two treatment groups on days 3, 5, 7, and 14 (P = 0.4, 0.7, 0.7, and 0.2, respectively on days 3, 5, 7, and 14. DISCUSSION Co-T and PS were both effective in the treatment of uncomplicated falciparum malaria in children from this endemic area of Southwest Nigeria. Apart from a significantly shorter parasite clearance in the Co-T-treated children, none of the outcome measures, clinical or parasitological, differed between the two antifolate drug combinations. The results support those of recent findings from the same area (Fehintola et al. 2004) and are in agreement with those from Kenya (Omar et al. 2001). However, the results are contrary to the suggestion that Co-T is less effective than PS for the treatment of malaria (WHO 1996). In many areas in Africa, for example in Uganda, there has been appreciable decline in the sensitivity of P. falciparum to Co-T (Kilian et al. 1998). The prevalence of gametocytaemia significantly increased following treatment with both drugs but this effect was more marked in those treated with PS than in those treated with Co-T. Sexual development in the malaria parasite and its modulation may be influenced by several factors (Carter & Miller 1979, Mons 1988). It is not clear whether the significantly lower carriage on day 14 in those treated with Co-T was due to fundamental differences in the responses of the asexual parasite populations to switch to gametocyte production following exposure to the two drugs. The components of Co-T have shorter half lives than those of PS and it is possible that this, coupled with individual variation in response, may partly explain the observed difference in gametocyte prevalence between the two drugs. Although there were no significant differences in gametocyte density in the two treatment groups, the significant increases in gametocyte prevalence with time, the greater proportion of children with patent gametocytaemia on both days 7 and 14 among children treated with PS, and the significantly higher propensity to have developed gametocytes by day 7 in PS compared with Co-T treated children (see Fig. 1) suggest a more marked effects of PS on gametocyte production. These findings with PS is in agreement with our previous observations (Sowunmi & Fateye 2003 a,b). Thus, the significantly reduced effects of Co-T on gametocyte retention may be an advantage for the use of Co-T over PS in endemic setting. Despite lower gametocyte prevalence and insignificant increase in gametocytaemia with time in Co-T treated children, both Co-T and PS appear to have similar effects on GSR. None of the post-treatment initiation GSR data differed between the two antifolate drug combinations; both drugs favoured gametocyte maleness. It is not clear whether the effects of the drugs on gametocytaemia is fundamentally different from their effects on GSR. Since GSR may be influenced by several factors (West et al. 2002, Gardner et al. 2003), this may impact on the temporal changes in GSR. The male-biased sex ratio after PS treatment is in agreement with our recent findings from the same area (Sowunmi & Fateye 2003b). The gametocyte maleness seen after initiation of treatment with both drugs suggests that antifolates, in general, may favour gametocyte maleness. Since gametocyte infectivity to mosquito is increased by gametocyte maleness (Roberts et al. 1996) and infectivity correlates with gametocyte density (Tchuinkam et al. 1993, Robert et al. 2000), both Co-T and PS by enhancing gametocyte maleness, gametocyte carriage and gametocytaemia, may markedly enhance malaria transmission whether the treated patients have antifolate sensitive or resistant infections. This a demerit for the use of these drugs alone for the treatment of malaria. REFERENCES
The following images related to this document are available:Photo images[oc05112f5.jpg] [oc05112f2.jpg] [oc05112f6.jpg] [oc05112t1.jpg] [oc05112t2.jpg] [oc05112f4.jpg] [oc05112f1.jpg] [oc05112f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}