 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memórias do Instituto Oswaldo Cruz, Vol. 100, No. 5, August 2005, pp. 541-548 Susceptibility of clinical isolates of multiresistant Pseudomonas aeruginosa to a hospital disinfectant and molecular typing Célia Maria Carvalho Pereira Araujo Romão/*/+, Yaisa Naziozeno de Faria, Luciana Roberto Pereira, Marise Dutra Asensi* Instituto Nacional
de Controle de Qualidade em Saúde *Instituto Oswaldo Cruz-Fiocruz,
Av. Brasil 4365, 21040-900 Received 31 March
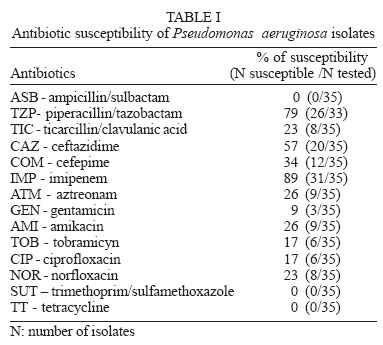
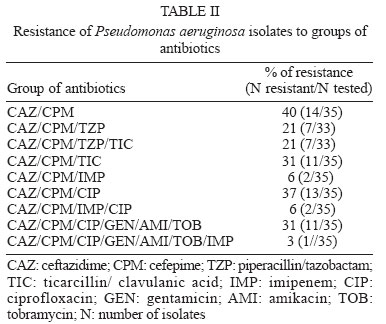
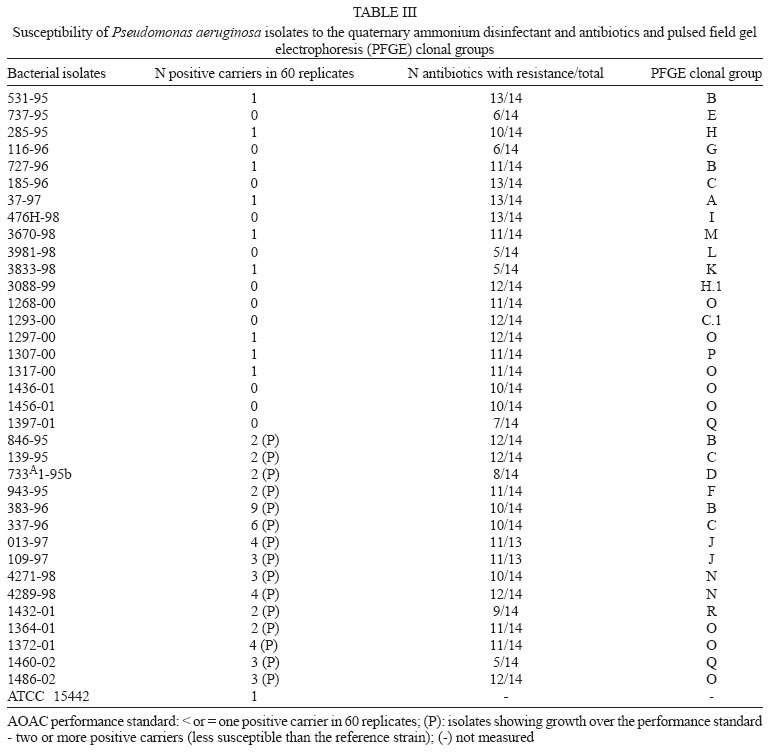
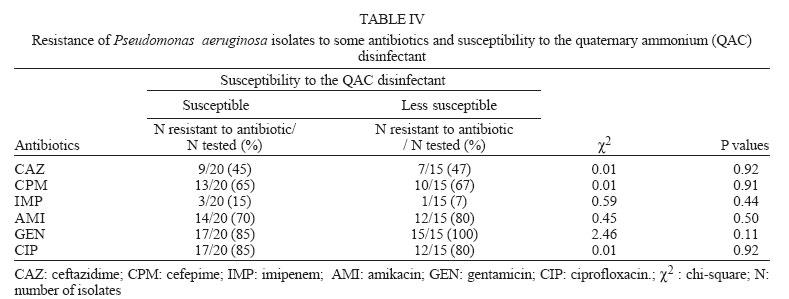
2005 Code Number: oc05127 The aim of this study was to evaluate the susceptibility of 35 resistant Pseudomonas aeruginosa clinical isolates to a quaternary ammonium hospital disinfectant. The methodology was the AOAC Use-Dilution Test, with disinfectant at its use-concentration. In addition, the chromosomal DNA profile of the isolates were determined by macro-restriction pulsed field gel electrophoresis (PFGE) method aiming to verify the relatedness among them and the behavior of isolates from the same group regarding the susceptibility to the disinfectant. Seventy one percent of the isolates were multiresistant to antibiotics and 43% showed a reduced susceptibility to the disinfectant. The PFGE methodology detected 18 major clonal groups. We found isolates with reduced susceptibility to the disinfectant and we think that these are worrying data that should be further investigated including different organisms and chemical agents in order to demonstrate that microorganisms can be destroyed by biocide as necessary. We also found strains of the same clonal groups showing different susceptibility to the disinfectant. This is an interesting observation considering that only few works are available about this subject. PFGE profile seems not to be a reliable marker for resistance to disinfectants. Key words: Pseudomonas aeruginosa - disinfectants - pulsed field gel electrophoresis Pseudomonas aeruginosa is one of the most important pathogen particularly in immunocompromised hosts and remains a prominent Gram-negative bacterium that causes hospital-associated infections. Infections by this microorganism are often difficult to treat because of its virulence, intrinsic and acquired antibiotic resistance, and the relatively limited choice for effective antimicrobial agents (Lyczac et al. 2000, Chuanchuen et al. 2002, Zavascki et al. 2005). It is also particularly resistant to biocides (disinfectants, antiseptics, and preservatives). Antibiotic resistance in bacteria has been subject of a great deal of research. By contrast biocide resistance is an emerging issue that is now attracting interest (Mac Donnell & Russel 1999, Higgins et al. 2001). Decontamination, disinfection, and sterilization are basic components of any infection control program (Widmer & Frei 1999, Rutala & Weber 2001). Engelhart et al. (2002) recently described a P. aeruginosa outbreak in haematology-oncology unit associated with contamination of the surface equipment when a non-germicidal cleaning solution, instead of disinfectants, was used for decontamination of the patients' environment. A wide variety of chemical agents are used as disinfectants in healthcare settings including glutaraldehyde, sodium hipochlorite, fenolics, quaternary ammonium compounds (QAC) and chlorhexidine. QAC are cationic surfactants that are widely used for the control of bacterial growth in clinical and industrial environment (Mc Bain et al. 2004). They have been used for a variety of medical, pharmaceutical, and other purposes (Hugo & Russell 1992). They are in general low-level disinfectants, showing activity to Gram-positive and Gram-negative bacteria (Romão 1996). There are some papers that deal with microbial resistance to biocides and antibiotics (Murtough et al. 2001) but beside the aspects about cross-resistance and co-resistance between antibiotics and disinfectants some questions should be investigated: are the hospital isolates being eliminated by commercial hospital disinfectants as expected? Are the hospital isolates as susceptible as the reference microorganisms used in disinfectant testing? Health-care professionals frequently ask us about these issues since data about these subjects are scarce in our country. According to Herruzo-Cabrera et al. (2004), the increased susceptibility of laboratory-adapted organisms may allow any disinfectant product to pass the standard tests but the product may fail in clinical settings. On the other hand, it has been observed that strains with the same PFGE (pulsed field gel electrophoresis) pattern or belonging to the same clonal group showed differences in the susceptibility to antimicrobial agents (Harris et al. 1999) but very few data are available concerning the behavior of strains from the same clonal group regarding susceptibility to disinfectants. Is PFGE a reliable marker to disinfectant susceptibility? The aim of this study was to evaluate the susceptibility of clinical isolates of P. aeruginosa to a quaternary ammonium disinfectant commonly used in health care settings, at its use-concentration, assessing simultaneously the reference strain P. aeruginosa ATCC 15442 recommended to disinfectant testing by official methods (Beloian 1990, AFNOR 1998, Singleton 2000). The isolates were also molecular evaluated with the objective to verify the relatedness among them and the behavior of isolates from the same group regarding the susceptibility to the disinfectant. MATERIALS AND METHODS Bacterial isolates - Thirty five bacterial isolates of P. aeruginosa were obtained from the Culture Collection of Department of Bacteriology, Oswaldo Cruz Institute, Oswaldo Cruz Foundation, Rio de Janeiro. All of them were isolated from clinical species in different years as follows: 1995 (seven), 1996 (six), 1997 (three), 1998 (six), 1999 (one), 2000 (five), 2001 (five), and 2002 (two). The reference strain P. aeruginosa ATCC 15442 was used in disinfectant testing. All the isolates were kept in BHI (brain heart infusion) broth with 20% of glycerol at -70ºC. Disinfectant - A commercial quaternary ammonium hospital disinfectant - QAC disinfectant (benzalkonium chloride 4%; inert ingredients 96%) was used. The use dilution was 5% in sterile distilled water, as recommended by the manufacture. Antimicrobial susceptibility test - All bacterial isolates were tested for antibiotic susceptibility through disk diffusion method according to National Committee for Clinical Laboratory Standard (NCCLS 2000) recommendations. The quality control was carried out by using standard strains of Escherichia coli (ATCC 25922), P. aeruginosa (ATCC 27953), and Staphylococcus aureus (ATCC 25923). Fourteen antibiotics were used as follows: ampicillin/sulbactam (10/10 µg); piperacillin/tazobactam (100/10 µg); ticarcillin/clavulanic acid (75/10 µg); ceftazidime (30 µg); cefepime (30 µg); imipenem (10 µg); aztreonam (30 µg); gentamicin (10 µg); amikacin (30 µg); tobramycin (10 µg); ciprofloxacin (5 µg); norfloxacin (10 µg); tetracycline (30 µg); trimethoprim/sulphamethoxazole (1.25/23.75 µg). Isolates resistant to all tested antimicrobial agents in two or more of the following antibiotic group were defined as multiresistant: β-lactam antibiotics including imipenem and aztreonam, aminoglycosides and the fluoroquinolone ciprofloxacin or all of these (Silva Filho et al. 2001, Herruzo-Cabrera et al. 2004). Disinfectant susceptibility test - Susceptibility testing was performed using Association of Official Analytical Chemists (AOAC) Use-Dilution Method (Beloian 1990). Briefly, stainless steel ring carriers (penicylinders) were inoculated by soaking them in a 48 h broth culture with 107 to 108 cfu/ml of each bacteria strain for 15 min, yielding 105 to 106 cfu/carrier. The carriers were removed with a hooked inoculating needle and allowed to dry for 40 min at 36 ± 1ºC in Petri dish matted with two filter paper sheets. After drying, the inoculated carriers were placed individually into the disinfectant solution and exposed for 10 min. The penicylinders were removed carefully and placed into tubes containing 10 ml of neutralizing broth (Letheen Broth/DIFCO). After 20 min each carrier was removed to other new tubes with the same culture broth, in order to assure the neutralizing process. All tubes were incubated for 48 h at 36 ± 1ºC. Sixty carriers were used for each experiment. The controls were performed as follows: viability of medium broth one inoculated carrier was placed in a sterile tube with Letheen broth; the expected finding of bacteria growth was always found. Sterility of medium broth 5% of all media used were incubated for 7 days at 36 ± 1ºC. In addition, the sterility of the distilled water used to prepare disinfectant solution and the sterility of pipets were verified; all the sterility controls were satisfactory. The control of neutralization was performed after incubation of the test by inoculating tubes showing no growth with a 24 h culture of the corresponding isolate (one inoculating needle). The tubes were then incubated further 48 h at 36 ± 1ºC (Singleton 2000); the expected result was bacterial growth and it was always found. The P. aeruginosa strain ATCC 15442 was included in the study as the reference. The performance standard of the method is: only 1 positive/60 replicates of carriers is admitted to consider that the disinfectant is efficient to kill the test microorganisms. Isolates showing two or more positive carriers were considered less susceptible to the disinfectant than the reference strain. PFGE method - P. aeruginosa isolates were grown in tripticase soy agar overnight. Growth was suspended in 2 ml of sterile saline and cells were pelleted and washed with sterile saline. To the pellet it was added 30 µl of 50 mM EDTA (pH 8.0), 10 µl of lisozyme solution (10 mg/ml), and 200 µl of TEN solution (100 mM Tris-100 mM EDTA-150 mM NaCl pH 7.5). A 240 µl volume of 2% low-melting-point agarose was added and the mixture was solidified in plugs. Plugs were then incubated overnight at 50ºC, in EC solution (10 mM EDTA - 6 mM Tris - 0.5% lauryl sarkosyl - 0.5% Brij 58 - 0.2% sodium deoxycholate - 5.84% NaCl pH 7.5) at 37ºC and then treated with the proteinase K solution (0.5 M EDTA - 1% lauryl sarcosyl - 1mg/ml proteinase K pH 9.3). Afterwards plugs were washed with purified water, equilibrated with TE (100 mM Tris - 100 mM EDTA pH 7.5) and stored at 5ºC until use. Prior to the restriction, the plugs were washed with DNS solution (20 mM Tris - 1 mM MgCl2) four times and then with 100 µl of restriction enzyme buffer. DNA present in agarose plugs were digested with 10 U of Spe I during 20 h and the electrophoresis procedure was carried out in 1% agarose gels with TBE (Tris-borate - EDTA) 0.5´ as the running buffer in a CHEF DR III pulsed-field electrophoresis system (BioRad). Running conditions consisted of two ramps in sequence (ramp A-an initial switch time of 0.5 s, a final switch time of 25 s, and a run time of 20 h; ramp B-an initial switch time of 30 s, a final switch time of 60 s, and a run time of 3 h). The voltage was 6V/cm for both ramps and the temperature was kept constant at 13ºC. The fragments were stained with ethidium bromide and photographed. Band patterns were analyzed using GelCompar II (Applied Maths, Belgium), without using internal markers. Similarity between fragments was determined by the Dice's Coefficient. A dendrogram was generated by unweighted pair group method with arithmetic averages (UPGMA). Strain relatedness was assigned in accordance to Tenover et al. (1995), considering similarity index of 90%. Capital letters (A-R) were used to designate the main clonal groups and subclones were assigned by additional numerical suffixes. Statistical analysis - Comparisons between susceptible and less susceptible isolates to the disinfectant, concerning antibiotic resistance, were performed using the chi-square test. RESULTS Antibiotic susceptibility - The antibiotic susceptibility of the P. aeruginosa isolates is presented in Table I. The isolates differed in their susceptibility to the antibiotics tested and those with intermediary susceptibility were considered resistant. All of them showed resistance to antibiotics whereas 71% were considered multiresistant. They were more susceptible to imipenem with 89% (31/35) of susceptibility. Piperacillin + tazobactam was the second most active antibiotic with 79% (26/33) of susceptibility. Thirty four percent (12/35) were susceptible to cefepime and 57% (20/35) to ceftazidime. The percentage of susceptibility to gentamicin, amikacin, tobramicyn, ciprofloxacin, and norfloxacin was 9 (3/35), 26 (9/35), 17 (6/35), 17 (6/35), and 23 (8/35), respectively. All the isolates were resistant to tetracycline and to sulphametho-xazol + thrimethoprin. Table II shows the resistance of the isolates to groups of antibiotics. It can be observed that 40% of them were resistant to both ceftazidime and cefepime and 37% were resistant to the cephalosporines and to ciprofloxacin. Susceptibility to the QAC disinfectant - The evaluation of the susceptibility to the QAC disinfectant demonstrated that 15 isolates (43%) showed two or more positive cylinders, which is over the performance standard established by the used methodology (only one positive carrier is admitted), meaning less susceptibility to the disinfectant. In five cases, we found four or more positive penicylinder, whereas the reference strain showed growth within the performance standard (Table III). The percentage of resistance to some antibiotics of the susceptible and the less susceptible isolates to the disinfectant is shown in Table IV. Comparisons between the susceptible and less susceptible isolates to the QAC disinfectant, concerning antibiotic resistance, using the chi-square test, showed no significant differences between the two groups of isolates. We also compared the susceptibility to QAC disinfectant between isolates showing resistance to 10 or more antibiotics and those showing resistance to less than 10 drugs. No significant differences were observed using chi-square test (χ2 = 0.12; P value = 0.72). Molecular typing - Restriction analysis of chromosomal DNA using Spe I enzyme resulted in the dendrogram generated by GelCompar II and revealed 18 major clonal groups (Figure). Clonal groups O and B were the most frequent. Isolates belonging to same clonal group showed differences in their susceptibility to antibiotics. This was observed, for example, with isolates 531-95, 727-95, 846-95, and 383-95 from clonal group B (Table III). The same was observed concerning the susceptibility to the QAC disinfectant. Isolates 1268-00, 1297-00, 1307-00, 1436-01, and 1456-00 from group O were susceptible while isolates 1364-01, 1372-01, and 1486-02, of the same group, were less susceptible than the reference strain. It can be noted that strains 185-96, 139-96, 337-96, and 1293-00 belong to the same clonal group, showing the persistence and spread of this group from 1996 to 2000. Strains from 1996 and 2000 came from different hospitals. DISCUSSION P. aeruginosa is a leading cause of nosocomial infection especially in intensive care units and was the most frequent isolated pathogen among the non-fermentative Gram-negative bacilli isolates from the SENTRY Antimicrobial Surveillance Program Medical Centers, 1997-2001 (Jones et al. 2003). The intrinsic susceptibility is limited to only a few antimicrobial agents and the emergence of resistance during therapy occurs with a relatively high frequency (Bert & Lambert-Zechovsky 1999). In the Global SENTRY Antimicrobial Surveillance Program, 1997-1999 the occurrence rates of multi-drug resistant P. aeruginosa raged from 8.2% (Latin America) to 0.9% (Canada) (Gales et al. 2001). According to Martins et al. (2004) P. aeruginosa and Acinetobacter baumannii are the most resistant bacteria in Intensive Care Unit at Hospital São Paulo, in Brazil. Thus, we decided to study resistant isolates since they are the major problem in clinical settings. The isolates studied were resistant and multiresistant organisms. The presence of multi-drug resistant isolates probably occurred due to the empirical treatment adopted in many hospital routines that induces selective pressure of multiresistant bacteria. The most active drugs were imipenem and piperacillin + tazobactam. The antibiotic susceptibility of the studied isolates, concerning imipenem, is similar to those observed by Rhomberg et al. (2003) in the MYSTIC Program, 2002 in North America (88.5% susceptible) but in general their isolates were more susceptible. Isolates from the SENTRY Program, 1997-2001 (Jones et al. 2003) also had higher susceptibility than ours, and amikacin was the most active compound, but in our work only 26% of the isolates were susceptible to this drug. In Italy, Fadda et al. (2004) tested 1474 isolates of P. aeruginosa and observed the most active drug was meropenem (susceptibility rates of 80.7%), only 31.9% of the isolates were fully susceptible and 12.5% were classified as multiresistant isolates. The high resistance rates observed in the present study to gentamicin, amikacin, ciprofloxacin, aztreonam, cephalosporins of third and fourth generation, as well the high resistance to both ceftazidime and cefepime (40%) and to ceftazidime, cefepime and ciprofloxacin (37%) are of special concerning since these drugs are currently used in the treatment of infections caused by P. aeruginosa. Only two isolates were resistant to imipenem. However, attention must be paid in order to prevent and control the emergency and spread of resistance to carbapenems as isolates carbapenems-resistant have been reported in many countries including Brazil (Gales et al. 2001, 2003, Tsakris et al. 2003, Mendes et al. 2004). We compared susceptible and less susceptible isolates to the disinfectant concerning antibiotic resistance. At the disinfectant concentration used in the test we found no differences between the two groups. Rutala et al. (1997) compared the susceptibility to two disinfectants of antibiotic-susceptible and antibiotic-resistant bacteria and also found no differences. On the other hand, Kõljalg et al. (2002) concluded that strains resistant to antibiotics were usually less susceptible to clorhexidine. According to Russell (1998) the relationship between antibiotic and biocide resistance in Gram-positive and Gram-negative bacteria needs to be explored further. All studied strains were typed by PFGE DNA macro-restriction method. This methodology was chosen for this purpose since it is considered to have a high discriminatory capacity, good reproducibility and ease interpretation (Grudmann et al. 1995, Kersulyte et al. 1995). A great genetic diversity was observed, as expected, since the same was found by different authors (Grundmann et al. 1995, Talon et al. 1996, Ruiz et al. 2004). Römling et al. (1994) characterized more than 500 P. aeruginosa isolates finding many different patterns, indicating the extensive versatility of the species. We observed that isolates with the same PFGE pattern or belonging to the same clonal group showed differences in the susceptibility to antimicrobial agents. The same was found by Sader et al. (1993) and Loureiro et al. (2002). The latter observed the epidemic strain from pattern A showed 10 different antibiotic resistance patters that they associated with a possible pressure in the hospital environment. Interestingly in the present study, strains belonging to the same clonal groups showed different susceptibility to the disinfectant. Similarly Heir et al. (2004) observed that some profiles of Listeria monocytogenes included both benzalkonium chloride sensitive and resistant isolates. In our study we did not observe specific clonal groups related with more susceptibility to the disinfectant. However, the clonal group O occurred most frequently among the susceptible isolates to the disinfectant. The effective use of disinfectants is an important factor in preventing hospital-acquired infections (Rutala & Weber 2004). Disinfectants interrupt the transmission of microorganisms and provide an incremental public health benefit (Cozad & Jones 2003). Similarly to the increasing problems with antibiotic-resistant bacteria in modern hospitals, questions about bacteria resistance to disinfectants and antiseptics are on arise. Resistance to disinfectants typically results from cellular changes that impact on biocide accumulation, expression of efflux mechanisms and more rarely from target site mutations (Poole 2002). In Gram-negative bacteria efflux systems are multi-drug transporters including QacE and QacED1 proteins. qacE and qacED1 genes have been located in the 3' conserved segment of class 1 integrons in Gram-negative bacteria. In the variable regions of these integrons mobile genes cassettes are inserted, often carrying antibiotic resistance genes (Paulsen et al. 1993, Kazama et al. 1998), also for more recent antibiotics (carbapenems), as blaIMP, and, blaVIM genes (Gales et al. 2003, Tsakris et al. 2003, Mendes et al. 2004). Thus, QAC may co-select for antibiotic resistance since class 1 integrons carrying qac genes function as vectors for cassettes genes encoding antibiotic resistance (Gaze et al. 2005). This is particularly important in regard of dissemination of metallo-β-lactamases genes as carbapenems have a broad antibacterial spectrum and play a fundamental role in the treatment of infection caused by multiresistant P. aeruginosa. It is important to highlight that the presence of qac genes, detected by PCR, does not guarantee an effective real-world recalcitrance to disinfection as disinfectants are used in high concentrations and resistance to biocides may also involve other different mechanisms, but certainly may increase its probability and favour co-resistance of QAC and antibiotics (Chapman 2003). Resistance to biocides is often reported in terms of MIC. MIC provides a useful starting point in investigation but cannot be relied upon to show that reduced susceptibility occurred to in-use concentrations (Russell 2004). In our study we evaluated the susceptibility of the isolates using the in-use concentration of the disinfectant and a carrier test that is officially adopted to assess the efficacy of disinfectants. Most reports analyze the effect of disinfectants against reference strains so that results of these experiments should be reproducible by other laboratories but concerning about susceptibility of clinical isolates to disinfectants is now attracting special attention. According to Herruzo-Cabrera et al. (2004) ATCC strains are laboratory adapted and may not be good predictors for the susceptibility of patient strains. They concluded that disinfectant efficacy should be confirmed with recently isolated organisms. In our work it was shown that 43% of the studied isolates were less susceptible to disinfectant than the reference strain. The high rate of disinfectant decreased susceptibility observed is worrying considering the tests were performed with disinfectant in-use concentration that means a real-world situation. We think that the use of reference strains is important for regulatory purposes, quality control of biocides, and surveillance programs of efficacy but our results revealed that clinical isolates must be checked for their susceptibility. We found isolates with reduced susceptibility to the QAC disinfectant and these data point out the issue must be further investigated including different organisms and chemical agents. It is also important to consider that resistance to quaternary ammonium may co-select for antibiotic resistance via class 1 integrons and vice-versa. In addition, we observed that strains of the same clonal group showed different susceptibility to the disinfectant. This is an interesting observation because only few works are available about this subject. PFGE profile seems not to be a reliable marker for resistance to disinfectants. REFERENCES
Copyright 2005 Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc05127t4.jpg] [oc05127t2.jpg] [oc05127t1.jpg] [oc05127t3.jpg] [oc05127f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}