 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Epidemiological pattern and mortality rates for hepatitis A in Brazil, 1980-2002 - A Review Cláudia L Vitral/*/+, Ana Maria C Gaspar, Francisco José D Souto** Departamento de Virologia, Instituto Oswaldo Cruz-Fiocruz, Av. Brasil 4365, 21040-900 Rio de Janeiro, RJ, Brasil *Departamento de Microbiologia e Parasitologia, Instituto Biomédico, UFF, Niterói, RJ, Brasil **Núcleo de Doenças Infecciosas e Tropicais de Mato Grosso, Faculdade de Ciências Médicas, Universidade Federal de Mato Grosso, Cuiabá, MT, Brasil Financial support: Finep, CNPq +Corresponding author. E-mail: clvitral@ioc.fiocruz.br Received 1 December
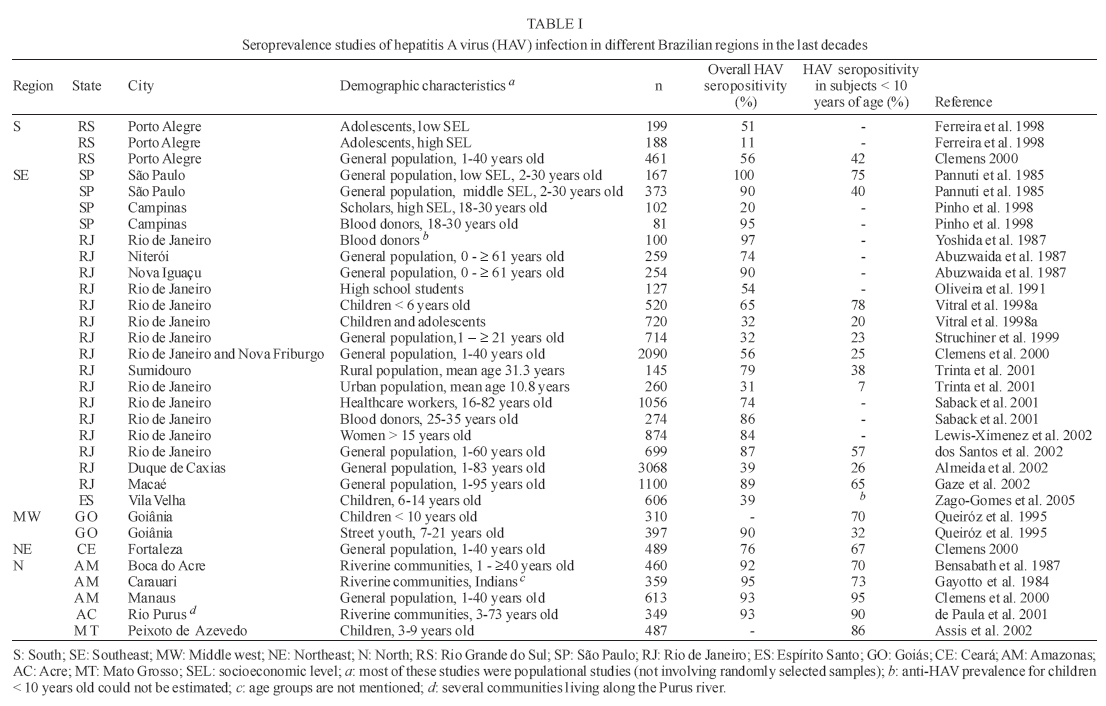
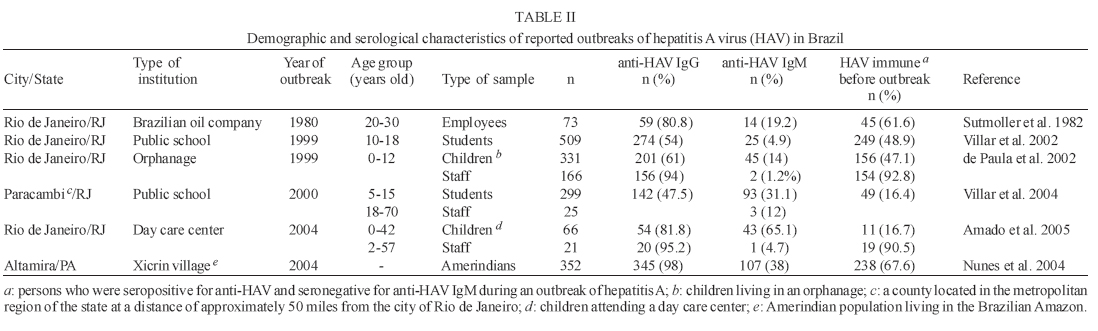
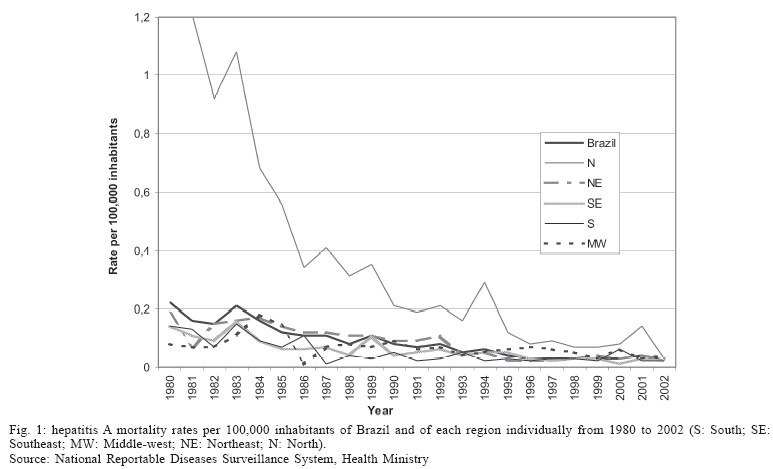
2005 Code Number: oc06024 The prevalence of hepatitis A virus (HAV) infection is high in developing countries, in which low standards of sanitation promote the transmission of the virus. In Latin America, which is considered an area of high HAV endemicity, most HAV-positive individuals are infected in early childhood. However, recent studies have shown that prevalence rates are decreasing. Herein, we review the data on HAV prevalence and outbreaks available in scientific databases. We also use official government data in order to evaluate mortality rates in Brazil over the last two decades. Studies conducted in the northernmost regions of Brazil have indicated that, although improved hygiene has led to a reduction in childhood exposure to HAV, the greatest exposure still occurs early in life. In the Southeastern region, the persistence of circulating HAV has generated outbreaks among individuals of low socioeconomic status, despite adequate sanitation. Nationwide, hepatitis A mortality rates declined progressively from 1980 to 2002. During that period, mortality rates in the Northern region consistently exceeded the mean national rate and those for other regions. Excluding the North, the rates in all regions were comparable. Nevertheless, the trend toward decline observed in the South was paralleled by a similar trend in the North. Key words: hepatitis A virus - hepatitis A/epidemiology - hepatitis A/mortality - Brazil Infection with hepatitis A virus (HAV) occurs worldwide and is the most common cause of acute viral hepatitis. The highest prevalence of this infection is seen in developing countries, where low standards of sanitation promote the transmission of the virus. Acquired primarily by the fecal-oral route, HAV infection is easily disseminated, either by person-to-person contact or by ingestion of contaminated food or water (Ferreira & Pretto 1999). Very often, HAV infection is asymptomatic or evolves without causing jaundice, thereby going undetected. The likelihood of presenting some symptoms increases with age, and most HAV infections in children < 6 years are clinically silent. For this reason, in areas of high endemicity, most people become infected in early childhood, although the number of diagnosed cases is small (Ferreira & Pretto 1999). If symptoms occur, hepatitis A usually has a benign course, with complete resolution and no sequelae. In some individuals, especially adults, the disease is unusually prolonged or recurrent, but it never progresses to chronicity (CDC 1999). Fulminant liver failure is a severe but uncommon event (< 1% of cases) and is seen more frequently in adults. Even after liver transplantation, mortality from fulminant disease exceeds 50% (Lemon & Shapiro 1994). The main concepts regarding the epidemiology and control of hepatitis A are reviewed in this paper. Recent data concerning Brazil, where this disease is endemic, are also discussed, with the aim of providing information that might inform future decisions regarding the control of HAV infection in the country. Epidemiological patterns of HAV infection Various patterns of HAV infection have been described, varying in relation to the level of economic development (Gust 1992, Jacobsen & Koopman 2004). In areas of high endemicity, HAV is transmitted primarily by person-to-person contact. Although 90% of the children become infected by the age of 10, hepatitis A does not present a clinical problem, and outbreaks are uncommon events. This epidemiological pattern is typical in Africa and in the Middle East, as well as in several nations in Latin America and Asia. In areas of moderate endemicity, the incidence of HAV infection is high, and infection occurs most frequently in late childhood, adolescence or young adulthood. In such areas, outbreaks are common, transmission occurring by person-to-person contact or through consumption of contaminated food or water. This pattern of transmission has been seen in previously endemic regions in Latin America, Asia, and the Middle East, where average seroprevalence rates have been declining in the last years (Tanaka 2000, Kang et al. 2004). In developed countries, HAV endemicity is low, and rates of infection are highest among young adults (Pham et al. 2005). The virus is primarily transmitted through consumption of contaminated food and water, although some cases of person-to-person transmission have been reported. In such areas, outbreaks are also common. Despite this more favorable situation, HAV is still the most common etiologic agent of acute viral hepatitis in the United States (Hoofnagle & Lindsay 2004). Finally, in areas of very low endemicity, the disease rate is also very low, and infection typically occurs in adulthood. Cases of infection are sporadic, and individuals are usually contaminated during travels to endemic areas. This pattern can be seen in Scandinavia, a country with some of the lowest rates of HAV seroprevalence in the world (CDC 1999). The impact of socioeconomic improvements on the prevalence of HAV infection It is well known that HAV infection is strongly correlated with poverty and inadequate sanitation. In fact, the prevalence of HAV infection could even be used as an index of the level of development of a given country. Several countries, such as those in Southeast Asia, have presented socioeconomic improvements in recent decades. In those countries, a significant decline in HAV seropreva-lence has been seen among the youngest individuals (Chen 2003, Kang et al. 2004, Tosun et al. 2004, Letaief et al. 2005, Manfredi et al. 2005, Sacy et al. 2005). In the past, Latin America was considered an area of high endemicity for HAV infection, and most of its inhabitants were infected in early childhood. However, a recent multicenter study carried out in six countries (Mexico, the Dominican Republic, Chile, Brazil, Venezuela, and Argentina) has shown that HAV seroprevalence rates have decreased in the past 20 years, and that there has been a shift from high to medium endemicity of HAV throughout Latin America (Tapia-Conyer et al. 1999, Clemens et al. 2000, Tanaka 2000). After analyzing the data of four major Brazilian cities, Clemens et al. (2000) suggested that the epidemiological pattern of HAV infection in Brazil is following a similar trend. Hepatitis A in Brazil Seroprevalence studies - To identify publications on hepatitis A in Brazil, we used the Medline database, as well as the Literatura Latinoamericana y del Caribe en Ciencias de la Salud (LILACS, Latin American and Caribbean Health Sciences Literature) database. The search strategy included all the studies published through October 31, 2005, employing the following free-text search terms: (hepatitis A OR HAV) AND (prevalence OR epidemics OR survey OR incidence OR outbreak) AND (Brazil), as well as their counterparts in Portuguese. All descriptive and comparative studies were considered, regardless of the methodology used. Studies dealing with subpopulations, such as of individuals with chronic liver diseases or of HIV-seropositive individuals, were excluded from the analysis. We identified 60 articles in Medline and 27 in LILACS. Most articles found in LILACS had previously been identified in the Medline search. Some of these articles were excluded because they presented epidemiologic data on hepatotropic viruses other than HAV. Therefore, a total of 21 publications about hepatitis A sero-prevalence and 6 articles on hepatitis A outbreaks in Brazil were evaluated for this review (Tables I and II). Most studies of HAV seroprevalence in Brazil have been conducted in the Southeastern region, especially in the state of Rio de Janeiro, attesting to the greater number of research groups studying the topic in that state. (Table I summarizes the data found in publications about seroprevalence of HAV infection in Brazil since the end of 1970s. The data are difficult to compare because of the different methodologies employed in these studies. Some studies included a representative, and randomly selected, sample of the general population, whereas others dealt with a smaller number of individuals or with groups of individuals of different ages. Despite the difficulties in analyzing studies conducted at different times and that used different methodologies, some patterns were observed and merit special attention. The results of studies conducted in the Northern and Northeastern regions indicate that exposure to HAV early in life was greater in those regions than in the cities of Southern and Southeastern Brazil (Clemens et al. 2000). It has been demonstrated that this regional discrepancy is considerably more significant when only children under five years of age are considered. In Northern Brazil, HAV seroprevalence rates as high as 90% have been reported for this age group. Of note is the fact that this highly endemic pattern of HAV infection does not seem to have changed over the last few years. A recent seroprevalence study carried out in a small city in the state of Amazonas (Assis et al. 2002) showed that HAV seroprevalence rates among children under 10 years of age are as high as those reported by Bensabath et al. (1987) 15 years earlier. It is possible that the poor sanitary conditions seen in the state of Amazonas are responsible for maintaining the epidemiological pattern of HAV in stasis over the last decades. A clear inverse correlation between exposure to HAV and socioeconomic level has been demonstrated in several studies (Pannuti et al. 1985, Abuzwaida et al. 1987, Ferreira et al. 1996, Pinho et al. 1998, Zago-Gomes et al. 2005). Typically, sanitation facilities are first provided in metropolitan regions; which explains why exposure to HAV remains more common in rural regions and small cities, principally affecting their youngest inhabitants. However, changes in HAV seroprevalence cannot be always considered indicative of socioeconomic changes. Improvements in sanitary conditions have been implemented in several urban areas, and the socioeconomic level of the inhabitants remained the same. This profile was demonstrated in a study carried out in two different populations of low socioeconomic status in Rio de Janeiro, a city located in the Southeastern region. Serum samples were collected in 1978 and again in 1995 (Vitral et al. 1998a). During this 17-year period, living standards improved; sewage systems were installed, and access to running water was provided. Consequently, HAV seroprevalence fell from 98.1 to 7.8% among children under the age of 5. Nevertheless, the socioeconomic level of the population remained the same. A decline in HAV seroprevalence (from 54.3 to 31%, p = 0.0006) was also observed in another study conducted in the city of Rio de Janeiro, in which serum samples were collected in 1986 and again in 1996 from health care students attending a public university (Oliveira et al. 1991, Vitral et al. 1998b). The decline in HAV seroprevalence within this community reflects a decreasing exposure to HAV, which is closely associated with better living standards. Hepatitis A outbreaks in Brazil - Improved hygiene and socioeconomic conditions have led to a reduction in HAV exposure during childhood in several regions of the world (Jacobsen & Koopman 2004). However, the persistence of circulating HAV may result in hepatitis A outbreaks, particularly in adolescents and adults (Wheeler et al. 2005). Prior to 1999, there had been only one reported hepatitis A outbreak in Brazil (Sutmoller et al. 1982) (Table II ). That outbreak occurred among employees of a Brazilian oil company located on Fundão Island, within the city of Rio de Janeiro, and appeared to be associated with drinking contaminated water from polluted wells. From 1999 to the present, a total of five outbreaks have been reported, four of which occurred in closed communities (schools and day care centers) in the state of Rio de Janeiro (Table II ). It is known that such establishments constitute significant sources of enteric virus transmission. It is interesting to observe that all of these outbreaks involved individuals who, although of low socioeconomic status, were living in houses with adequate sanitation. However, Villar et al. (2002, 2004) found that, despite adequate sanitation, these individuals are at risk for HAV infection due to the overcrowding that is typically seen in such communities. The authors found that conditions in which more than four persons were living in a two-room dwelling correlated with higher HAV seroprevalence. Other factors have been reported to increase the chances of HAV dissemination within schools. Such factors include improper hygiene (more often seen among younger pupils), poor sanitary conditions in school bathrooms, and contact with HAV-infected individuals, especially those that are asymptomatic. Under these conditions, person-to-person transmission seems to be the main mode of HAV dissemination, given the high proportion (> 50%) of individuals susceptible to HAV infection and below the age of 20 seen in most of the hepatitis A outbreaks occurring since 1999 (de Paula et al. 2002, Villar et al. 2002, 2004, Amado et al. 2005). In epidemics involving children aged < 5 years of age, only 16 to 17% were HAV immune (seropositive for anti-HAV and seronegative for anti-HAV IgM) prior to the outbreak (Villar et al. 2004, Amado et al. 2005). Recent laboratory test results suggest that an outbreak of HAV infection has occurred in an Amerindian population in the Amazon Basin (Nunes et al. 2004), a region known to be highly endemic for HAV. Serological markers of HAV were investigated in 352 indigenous people after a child died of icterohemorrhagic fever. In this population, 30.5% of the individuals were positive for anti-HAV IgM. The rates of HAV seroprevalence seen in the populations involved in these outbreaks demonstrate the same tendency seen in seroepidemiological studies carried out in some Brazilian regions (Vitral et al. 1998a,b, Tapia-Conyer et al. 1999, Clemens et al. 2000, Almeida et al. 2001, 2002, Carrilho et al. 2005), the results of which indicate a possible change in the epidemiological pattern of hepatitis A in the country. Therefore, it is likely that outbreaks will begin to occur with greater frequency. Those same results indicate that the youngest individuals, especially those under 5 years of age, are mostly unprotected from HAV infection, regardless of their socioeconomic status, and should be the target of future vaccination programs (Dagan et al. 2005, VanDamme et al. 2005, Wasley et al. 2005). Hepatitis A mortality in Brazil - Surveillance data on the incidence of hepatitis A in Brazil are lacking. There is no pre-1994 data available, and, in recent years, hepatitis A has been considered a disease that no longer needs to be reported, thereby compounding the problem. In addition, a great part of the hepatitis cases that have been reported are still classified as "acute hepatitis due to unknown cause", which could be related to the lack of properly equipped diagnostic laboratories in remote areas of Brazil. Therefore, in an attempt to generate reliable information on the trends seen in hepatitis A incidence in Brazil, we analyzed only the rate of hepatitis A mortality since fatal cases are generally well investigated and properly diagnosed. Aiming to calculate the mortality rate per 100,000 individuals, the 1980-2002 National Reportable Diseases Surveillance System database was consulted, as were the 1980, 1990, and 2000 Brazilian demographic census databases. The distribution of mortality by gender and age (< 10 years, 10-19 years and ≥ 20 years) was also evaluated. Fig. 1 shows the evolution of mortality rate per 100,000 inhabitants during the period of 1980 to 2002. A progressive decline in hepatitis A mortality rate could be seen in all Brazilian regions during the period. A mortality rate of 0.2/100,000 inhabitants was seen in 1980. From that year on, the rate decreased: to < 0.1/100,000 inhabitants in 1990 and to < 0.05/100,000 inhabitants in 1995, until the rate of 0.02/100,000 inhabitants in 2002. During that period, the mortality rate in Northern Brazil was consistently 3 to 4 times higher than the mean national rate and than those reported in the other regions. However, the mortality rate observed in the northern region has also followed the trend toward a decline seen throughout the country. By the end of 2002, the rates seen in the North were almost the same as those seen in other Brazilian regions (0.03/100,000 inhabitants). These data clearly suggest a progressive decline in the incidence of fatal cases related to HAV infection in Brazil. Since these cases constitute a small, but predictable, portion of all acute hepatitis A cases, which are in turn part of the total number of HAV infections, these data suggest that there has been a decline in HAV circulation in all Brazilian regions over the two last decades. This epidemiological profile of hepatitis A is in accordance with the tendency seen in seroprevalence studies carried out in some Brazilian population groups (Vitral et al. 1998a, b, Clemens et al. 2000, Tanaka 2000). This profile has also been observed in other countries where standards of living are higher (Chen 2003, Kang et al. 2004, Tosun et al. 2004, Letaief et al. 2005, Sacy et al. 2005). It could be suggested that the observed drop in the hepatitis A mortality rate results from increases in the quality of health care and greater availability of liver transplantation in specialized centers in major urban cities of the country within the last decade. However, it is widely known that the availability of intensive therapy is limited in most public hospitals in Brazil. In addition, liver transplantation as a therapeutic strategy for patients with fulminant liver failure in Brazil is rarely an option due to the great difficulty in obtaining donated organs promptly. Another aspect indicating that the rate of hepatitis A mortality is falling as a direct consequence of declining HAV endemicity rates is that this tendency has been seen both in the South, which is a more developed region, and in the North, where intensive therapy is even less often available, and liver transplantation programs are either in their infancy or are nonexistent. The fact that hepatitis A mortality rates have been always higher in the Northern region, followed by the Northeastern region, is in agreement with data from cohort studies showing that the disease is more common in less developed regions of Brazil (Tapia-Conyer et al. 1999, Tanaka 2000). The higher mortality rates seen in these regions are probably related to limited financial support for intensive care. However, substantial mortality rates have been observed even in cities with more advanced and better equipped centers, supporting the hypothesis that mortality rates are highest in regions where HAV is extensively disseminated. During the period evaluated, the mortality rate was higher among males than females (at a ratio of 1.3:1), with exception of the years 1996, 1998, and 2002 (data not shown). Fig. 2 shows the age-specific mortality distribution during the period studied. It can be observed that mortality was almost always higher among individuals > 20 years of age, which could be related to the (expected) greater severity of HAV infection in older patients. Controlling hepatitis A in Brazil During the 1990s, formalin-inactivated vaccines were developed (HAVRIX by Smith-Kline Beecham; and VAQTA by Merck, Sharpe & Dohme). These vaccines proved to be safe and effective in preventing hepatitis A. Recently, data on vaccination strategies adopted in countries with low to intermediate rates of hepatitis A (the US and Israel) have been reported (Wasley et al. 2005, Dagan et al. 2005). In those two countries, vaccination programs were implemented simultaneously in 1999, and analyses were performed using data obtained up through 2003. In the United States, it was recommended that routine vaccination of children be implemented in 11 states with hepatitis A rates that were 20 or more cases per 100,000 inhabitants during the 1987 and 1997 baseline period (Wasley et al. 2005). In Israel, a country of rather small geographic dimensions and with a population estimated at 6.29 million, the vaccination strategy included all children aged 18 to 24 months (Dagan et al. 2005). Both vaccination programs achieved a significant reduction in the rate of hepatitis A, which was observed within a few years after their implementation. Interestingly, the vaccination strategy adopted in Israel resulted in a marked herd immunity effect. Although only toddlers had been immunized, a sharp decrease in disease rates was seen among older children, and even among adults. In addition, reductions in the disease rates were obtained in populations of both low and high socioeconomic status in the US and in Israel. Since children serve as a source of infection for other children and adults, they play an important role in HAV transmission, as demonstrated by Staes et al. (1997) and Smith et al. (1997). Data provided by those authors are in accordance with those obtained by others (Dagan et al. 2005, Valenzuela et al. 2005, Van Damme & Van Herck 2005) and with the recommendations of Advisory Committee on Immunization Practices of the Centers for Disease Control and Prevention [MMWR 1999; 48 (No. RR-12)]. Taken together, these data strongly suggest that vaccination of children is the most effective way to reduce the incidence of hepatitis A over time and to potentially eliminate infection. Unfortunately, the cost of vaccination remains high, preventing its wider use in developing countries. Brazil is a country of vast proportions and striking regional differences. Whereas the epidemiology of HAV infection seems to evolve more slowly in rural areas and in the Northern regions, a decline in its prevalence has been clearly observed in metropolitan regions. What would be the best large-scale vaccination strategy to be adopted in Brazil if costs were lower? Should HAV vaccination be included in the national program of immunization? Should children be the target of vaccination programs? Or perhaps vaccination strategies should target those older than 20 years of age, since this group presents the highest mortality rate? Routine pediatric vaccination has been claimed as the best strategy since, as previously mentioned, children play a critical role in disease transmission. However, in view of the high predicted HAV seroprevalence among adolescents and adults in areas of intermediate to high rates of hepatitis A, vaccination of individuals in this age group would involve considerable investment with a small return in effectiveness (Arankalle & Chadha 2003). The adoption of a serology-based vaccination strategy could reduce the costs since only individuals presenting serologically documented lack of immunity would receive the vaccine (Saab et al. 2000). However, the savings achieved would depend on several factors, such as the expected prevalence of natural immunity among individuals, as well as the costs involved in the prevaccination screening and the vaccination itself. Whether or not, and to which age group these strategies should be applied are decisions that will require more solid data from seroepidemiological studies. Such data will be critical for determining the actual pattern of HAV infection endemicity in different populations in the country, as well as for the evaluation of trends in hepatitis A incidence and mortality. It should be mentioned that there are four public Brazilian institutions involved in the production of vaccines (Bio-Manguinhos-Fiocruz, Instituto Butantan, Tecpar, and Fundação Ataulfo de Paiva). Thus, it is reasonable to assume that a nationally-produced (and therefore more affordable) HAV vaccine could facilitate the implementation of a national immunization program. Finally, providing better standards of living for Brazilians of low socioeconomic status, especially those living in the Northern regions, still represents a challenge. According to the 2000 Brazilian demographic census, 81.7% of the districts in the Southeastern region have sewage systems, compared with only 30.2% in the Northeastern region. In the North, only 5.7% of the households are connected to sewage systems. Undoubtedly, at least in the poorest Brazilian regions, improving sanitation is still a priority and will help to prevent the transmission of hepatitis A, as well as of other enterically transmitted infections. REFERENCES
Copyright 2006 Instituto Oswaldo Cruz - Fiocruz |

{kind=link}
{kind=link}
{kind=link}
{kind=link}