 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memórias do Instituto Oswaldo Cruz, Vol. 101, No. 3, May 2006, pp. 245-250 Frequency of serovars and antimicrobial resistance in Shigella spp. from Brazil Gisele Peirano+, Flávia dos Santos Souza, Dalia dos Prazeres Rodrigues, Shigella Study Group Laboratório
de Referência Nacional de Cólera e outras Enteroinfecções
Bacterianas, Instituto Oswaldo Cruz-Fiocruz, Financial
support: CNPq (process 142069/2001-9), NRLCED, IOC-Fiocruz Received
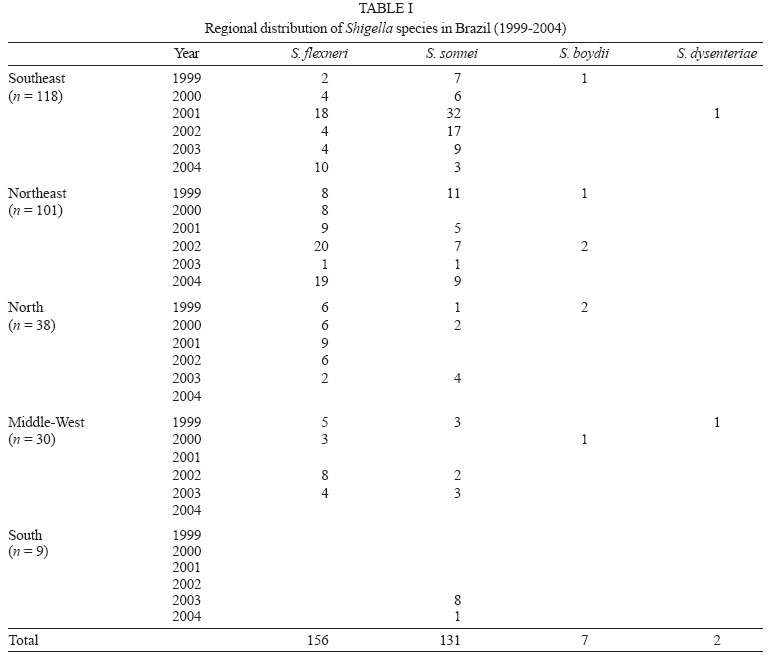
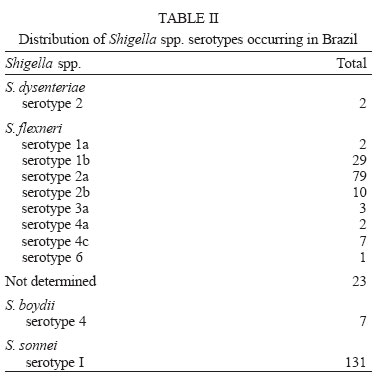
20 September 2005 Code Number: oc06043 A total of 296 Shigella spp. were received from State Public Health Laboratories, during the period from 1999 to 2004, by National Reference Laboratory for Cholera and Enteric Diseases (NRLCED) - IOC/Fiocruz, Rio de Janeiro, Brazil. The frequency of Shigella spp. was: S. flexneri (52.7%), S. sonnei (44.2%), S. boydii (2.3%), and S. dysenteriae (0.6%). The most frequent S. flexneri serovars were 2a and 1b. The highest incidence rates of Shigella isolation were observed in the Southeast (39%) and Northeast (34%) regions and the lowest rate in the South (3%) of Brazil. Strains were further analyzed for antimicrobial susceptibility by disk diffusion method as part of a surveillance program on antimicrobial resistance. The highest rates of antimicrobial resistance were to trimethoprim-sulfamethozaxole (90%), tetracycline (88%), ampicillin (56%), and chloramphenicol (35%). The patterns of antimicrobial resistance among Shigella isolates pose a major difficulty in the determination of an appropriate drug for shigellosis treatment. Continuous monitoring of antimicrobial susceptibilities of Shigella spp. through a surveillance system is thus essential for effective therapy and control measures against shigellosis. Key words: Shigella - serovars - antimicrobial resistance surveillance - Brazil Shigellosis is endemic throughout the world and it is among the most common causes of bacterial diarrhoeal diseases. It is responsible for approximately 165 million cases annually, of which 163 million are in developing countries and 1.5 million in industrialized ones. It is estimated that 1.1 million people die annually from Shigella infection and nearly 580,000 cases of shigellosis are reported among travelers from industrialized countries. The frequency of S. flexneri , S. sonnei, S. boydii, and S. dys-enteriae were 60, 15, 6%, and 6% (30% of S. dysenteriae cases were type 1) in developing countries; and 16, 77, 2, and 1% in developed ones, respectively. In developing countries, the predominant serotype of S. flexneri is 2a, followed by 1b, 3a, 4a, and 6 (Kotloff et al. 1999). Although epidemic Shiga dysentery is the most serious manifestation of Shigella infection in developing countries, the majority of Shigella infections are due to endemic shigellosis. S. flexneri is the endemic species and is responsible for approximately 10% of all diarrhoeal episodes among children younger than five years. S. dysenteriae type 1 causes epidemic and endemic disease, whereas, in developed countries, S. sonnei is predominantly involved in common source sporadic outbreaks. S. boydii, was first detected in India and up to now has been uncommonly found, excepting in the Indian subcontinent (Niyogi 2005). Except for S. sonnei, each species contains multiple serotypes based on the structure of the O antigen, and, at least 49 serotypes of Shigella have been recognized, representing subtypes from three of the four groups; of which 15 belong to S. flexneri (Simmons & Romanowska 1987, Bopp et al. 2003). Besides the self-limiting duration of disease, effective antimicrobial therapy reduces dysentery duration and severity and can also prevent potentially lethal complications. Concomitantly, the excretion of the pathogen in stools is shortened significantly, reducing spread of the infection (Bhattacharya & Sur 2003). However, Shigella spp. can easily become resistant to antibiotics (WHO 2001). Indiscriminate use of drugs and horizontal gene transfer has led to Shigella species becoming resistant to commonly used antibiotics. Resistance patterns are influenced by geographic location, year that isolates were obtained, classes of antimicrobial agents, and pressure exerted by antimicrobial use. It was noticed that, over the past decades, Shigella strains have progressively become resistant to most of the widely use antimicrobials, such as ampicillin, chloramphenicol, tetracycline, and trime-thoprim-sulfamethoxazole (Lima et al. 1995, Ashkenazi et al. 2003). The antimicrobials that remain effective are ciprofloxacin and other fluoroquinolones, ceftriaxone, and azithromycin (Anonymous 2004). There are also quite striking geographic differences in the corresponding resistance rates. The antimicrobial resistance pattern differs between places. This may be due to the occurrence and spread of antimicrobial-resistant clones. Surveillance programs on antimicrobial resistance not only identify pathogenic bacterial species, by reporting data like serotyping, microorganisms incidence rates, and susceptibility to the antimicrobial agents currently used for treatment, but also contribute to monitoring the intervention strategies used to control their spread (WHO 2001). Since in Brazil shigellosis is not considered a compulsory notifiable disease, it has been difficult to estimate its incidence rate and respective importance on disseminating antimicrobial resistance. This study was conducted to evaluate the frequency of species, serovars, and antimicrobial resistance profiles of Shigella spp. received from 1999 to 2004, by Brazilian Shigella Surveillance Program on Antimicrobial Resistance conducted by National Reference Laboratory for Cholera and Enteric Diseases, Fiocruz, Ministry of Health, Brazil. MATERIALS AND METHODS Bacterial isolates - This study included 296 Shigella isolates selected from NRLCED Strain Collection. Such strains were isolated from human fecal samples, from both hospitals and outbreaks, and sent by State Public Health Laboratories to NRLCED for further identification and serotyping. Selective and differential media were used for isolating Shigella (xylose-lysine-desoxycholate XLD Agar, Oxoid, UK). Isolates identification was confirmed by standard biochemical laboratory methods (Bopp et al. 2003). Shigella antisera was raised in NRLCED, Fiocruz, and serological identification was performed by slide agglutination with polyvalent somatic (O) antigen grouping sera followed by testing with monovalent antisera for specific serovar. Strains were also submitted to antimicrobial susceptibility testing as part of a surveillance program on antimicrobial resistance and stored in NRLCED Strain Collection. All isolates were stored on phosphorous nutrient agar glass tubes and kept at room temperature (20-30ºC). Antimicrobial susceptibility testing - Antimicrobial susceptibility testing was performed in 278 Shigella strains by standard disk diffusion method, following NCCLS guideline. Tests were performed on Mueller Hinton agar plates, using antimicrobial disks (Oxoid): ampicillin (AMP 10 µg), amikacin (AMK 30 µg), cefoxitin (FOX 30 µg), ceftriaxone (CRO 30 µg), cephalothin (CEF 30 µg), chloramphenicol (CHL 30 µmg), ciprofloxacin (CIP 5 µg), gentamicin (GEN 10 µg), imipenem (IPM 10 µg), nalidixic acid (NAL 30 µg), nitrofurantoin (NIT 300 µg), tetracycline (TET 30 µg), and trimethoprim-sulfamethoxazole (SXT 1,25/23,75 µg). Standard control strains of Escherichia coli (ATCC 25922), Pseudomonas aeruginosa (ATCC 27852), Enterococcus faecalis (ATCC 29212), and Staphylococcus aureus (ATCC 29213) were used for monitoring the accuracy and precision of the disk diffusion test. The interpretation of zone diameters inhibition was that recommended by NCCLS (2003). The
serogroups prevalence of the 296 Shigella isolates was as
follows: S. flexneri, n = 156 (52.7%), S. sonnei, n = 131 (44.2%), S. boydii, n = 7 (2.3%), and S.
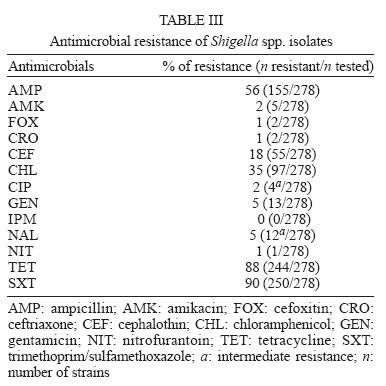
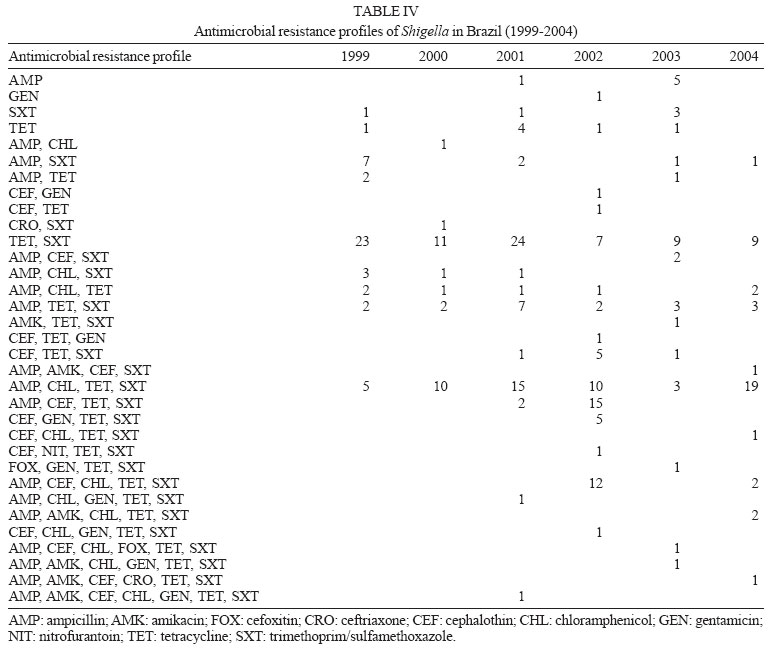
dysenteriae, The most frequent serotypes identified for S. flexneri were 2a and 1b. Both S. boydii and S. dysenteriae showed a very low number of isolates. Table II shows the distribution of Shigella species and serovars. Overall, the highest rates of antimicrobial resistance among Shigella isolates were to trimethoprim-sulfa-methozaxole (90%), tetracycline (88%), ampicillin (56%), and chloramphenicol (35%). Additionally twelve isolates and four isolates showed intermediate resistance to nalidixic acid and to ciprofloxacin, respectively. None of the isolates was resistant to imipenem (Table III). S. flexneri and S. sonnei shared a similar antimicrobial resistance profile for most of the antibiotics. Among the 278 Shigella isolates tested, 97.8% were resistant to both one or more antimicrobial agents, and 91% to either two or more antimicrobial agents. Antimicrobial resistance profiles to TET and SXT resistance occurred in 30% of isolates and to AMP, CHL, TET, and SXT in 22% of isolates (Table IV). DISCUSSION Shigellosis is becoming an increasingly significant public health problem due to development of multiple antimicrobial resistance, frequently resulting in treatment failure, leading in turn to health complications and deaths (Sur et al. 2004). In the Brazilian Shigella Surveillance Program, S. flexneri was the predominant isolated Shigella serogroup (≈ 53%) during the studied period, followed by S. sonnei (≈ 44%). This is in contrast with studies from other places in Brazil, which detected S. sonnei as the most frequent serogroups: Ribeirão Preto-SP (Medeiros et al. 2001), and Salvador-BA (Diniz-Santos et al. 2005). However, our finding is consistent with other reports from Northeastern Brazil (Lima et al. 1995), Porto Alegre-RS (Santos et al. 1997), and São José do Rio Preto-SP (Almeida et al. 1998), and those from other Latin America developing countries such as Argentina (Merino et al. 2004), Peru (Jones et al. 2004), and Chile (Fulla et al. 2005). We also noticed some differences in the Shigella geographical isolation incidence among Brazilian regions. S. flexneri was observed to have higher isolation incidence in the Northeast, and S. sonnei were more frequently isolated in the Southeast. These two Brazilian regions are social and economically quite different, the Southeast being more likely to have developed cities. This may be due to the modern lifestyle of developed cities, where the main ways of contracting shigellosis are by eating and/or drinking fecal contaminated food/water, and by person-to-person contact. The pathogens can be also transferred by flies, fingers, feces, food, and fomites. High-risk groups include children in day-care centers, homosexual men, people in custodial institutions, migrant workers, and travelers. Our data showed very low occurrence of S. boydii and S. dysenteriae. Infections by S. dysenteriae usually occur in less developed countries, often reaching epidemic levels, with periodic outbreaks (Niyogi 2005). Serotypes 2a and 1b were the most frequent serotypes of S. flexneri in this study, accounting for 59 and 21%, respectively, of the S. flexneri serotyped isolates. These are the most common serotypes occurring in developing countries (Kotloff et al. 1999, Souza 2001). Appropriate antibiotic treatment of shigellosis depends on identifying Shigella resistance patterns that are circulating locally. These imply in local surveillance of antimicrobial resistance and its implication in empirical therapy (Ashkenazi 2004). According to analyzed isolates, S. flexneri antimicrobial resistance patterns were mainly detected to ampicillin, chloramphenicol, tetracycline, and trimethoprim-sulfamethoxazole. S. sonnei presented a similar resistance profile, except for chlorampenicol, but with increasing resistance to cephalotin. Overall, it could be observed that such main resistance antimicrobial pattern (ampicillin, chloramphenicol, tetracycline, and trimethoprim-sulfamethoxazole) continues to be prevalent among Shigella isolates from Brazil (Lima et al. 1995, Rodrigues 2000). Also, in a recent study (Diniz-Santos et al. 2005) Shigella species presented a very high resistance rate to trimethoprim-sulfamethoxazole (90.1%), ampicillin (22%) alone or in combination with sulbactam, and also to piperacillin. Antimicrobial agents as effective options for shigellosis treatment are becoming limited due to globally emerging drug resistance. Multiple resistant strains have occurred in Europe (Maraki et al. 1998), Africa (Egah et al. 2003), Asia (Lee et al. 2001), and South America (Fulla et al. 2005). In the United States, the most common resistance rates among 620 Shigella isolates (86% of which were S. sonnei) were to ampicillin (77%), streptomycin (54%), trimethoprim-sulfamethoxazole (37%), sulfamethoxazole (32%), and tetracycline (31%) (CDC 2004). A similar resistance pattern was reported from England and Wales (Cheasty et al. 1998). Data from developing countries, such as Chile, indicate that most Shigella spp. are resistant to ampicillin (82%), cotrimoxazole (65%), tetracycline (53%), and chloramphenicol (49%) (Fulla et al. 2005). Reports from Bangladesh, where shigellosis is highly endemic, show a similar resistance pattern (Sur et al. 2003) compared to the ones in Latin America. Outbreaks caused by multiresistant S. dysenteriae type 1, including strains resistant to nalidixic acid, has also been reported. (Sarkar et al. 2003). Thus, neither ampicillin, chloramphenicol, tetracyclines nor trimethoprim-sulfamethoxazole should be considered appropriate empiric therapy for shigellosis any longer. Nowadays, recommended therapy for people infected with Shigella includes fluoroquinolones (Bhattacharya & Sur 2003, Khan et al. 2004, Anonymous 2004), azithromycin (Basualdo & Ardo 2003), and third-generation cephalosporins (Niyogi et al. 2001). However, it has been observed that S. sonnei have shown readily acquisition of resistance to ampicillin and cephalosporins through conjugative resistance-plasmids carrying resistance cassettes to beta-lactamases (Radice et al. 2001) and, in both S. sonnei and S. flexneri, chromosomal mutations that confer quinolones resistance (Jeong et al. 2003). Continuous monitoring of antimicrobial susceptibilities of Shigella spp. through a surveillance system is thus essential for effective therapy and control measures against shigellosis. It is also of concern the use of nalidixic acid as a first step screening test to detect mutations causing fluoroquinolone resistance. ACKNOWLEDGEMENTS To Mr Evaldo Soares for technical assistance. REFERENCES
Copyright 2006 Instituto Oswaldo Cruz - Fiocruz |

{kind=link}
{kind=link}
{kind=link}
{kind=link}