 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memórias do Instituto Oswaldo Cruz, Vol. 101, No. 3, May 2006, pp. 251-256 Seroepidemiology of hepatitis B virus infection and high rate of response to hepatitis B virus Butang® vaccine in adolescents from low income families in Central Brazil Michele Dias da S Oliveira, Regina MB Martins*, Marcos A Matos, Renata C Ferreira*, Márcia A Dias*, Megmar AS Carneiro*, Ana Luiza N Junqueira, Sheila A Teles/+ Faculdade de Enfermagem *Instituto de Patologia Tropical e Saúde Pública, Universidade Federal de Goiás, Rua 227 quadra 68 s/no, Setor Leste Universitário, 74605-080 Goiânia, GO, Brasil Financial
support: CNPq, Ceargs/Caps-UCSF Received
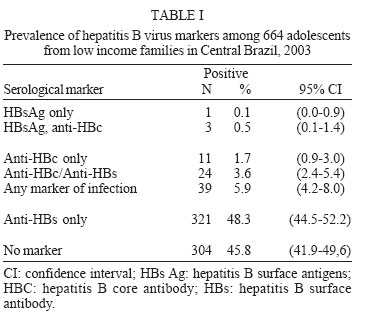
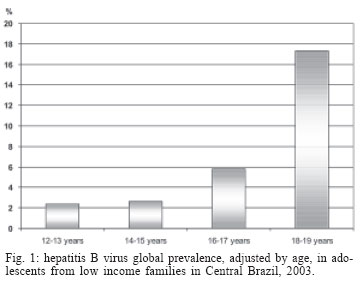
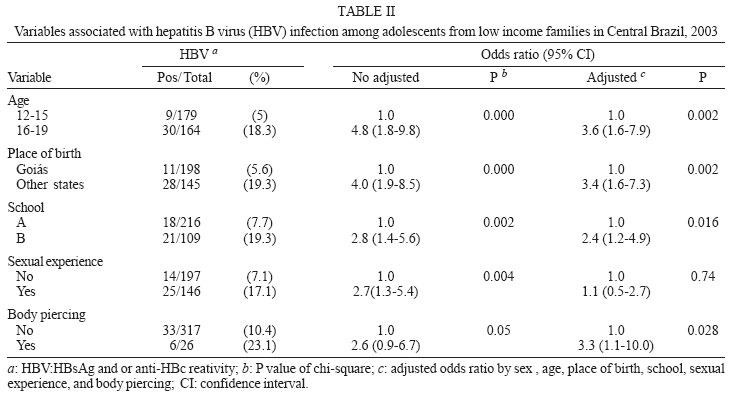
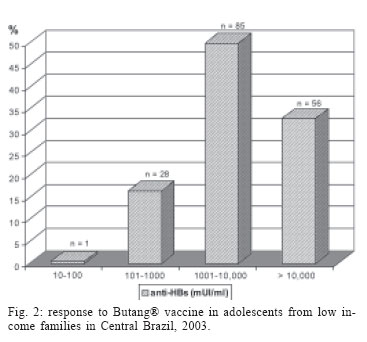
10 October 2005 Code Number: oc06044 In order to evaluate the seroepidemiology and response to Butang® vaccine in adolescents from low income families in Central Brazil, blood samples of 664 adolescents were tested for hepatitis B surface antigen (HBsAg), hepatitis B core antibody (anti-HBc), and hepatitis B surface antibody (anti-HBs) markers, and multiple logistical regression analysis was carried out to determine variables associated with hepatitis B virus (HBV) infection markers. further, three 20 µg butang® vaccine doses were offered to all susceptible individuals (n = 304). Among those who accepted them (n = 182), the seroresponse was evaluated in 170 individuals by quantitative anti-HBs. an overall hbv prevalence of 5.9% was found: four adolescents were HBsAg positive, 24 were anti-HBc, anti-HBs-reactive, and 11 were anti-HBc only. The analyse of risk factors showed that age 16-19 years, place of birth outside Goiás, school B and body piercing were statistically associated with HBV infection markers (p < 0.05). All 170 adolescents responded to butang®, and a geometric mean titer (gmt) of 4344 mui/ml was obtained. these results reinforce the importance of hepatitis b vaccine in adolescents despite of the hbv regional endemicity, and suggest that three doses of 20 µg of the butang® should guarantee protective anti-hbs levels to individuals at a critical time for hepatitis b acquiring such as latter adolescence and adulthood. Key words: hepatitis B - adolescents - vaccine - Brazil Hepatitis B virus (HBV) has been considered a global health problem. This has been cause of acute and chronic hepatitis, cirrhosis, and cancer of the liver (Mast et al. 2005). It is estimated 2 billion people have been infected and that more than 350 million of individuals are chronic carriers of HBV worldwide (Hou et al. 2005). Also, this infection has been answerable for 520,000 deaths each year (EASL 2003). In high endemic regions, hepatitis B is transmitted mainly by vertical or horizontal mode. In contrast, in low and intermediate endemic regions, it is disseminated generally by sexual and parenteral via (Hou et al. 2005, Mast et al. 2005) whereas an increase of HBV positivity throughout the adolescence and early adulthood was showed (Dominguez et al. 2000, Cisneros-Castolo et al. 2001, Gaze et al. 2002). During this period of life individuals are more susceptible to risk behaviors such as illicit drug use, alcohol abuse, multiple partners, and sexually transmitted diseases (Lawrence & Goldstein 1995, Miranda et al. 2005). Also, a higher risk of hepatitis B has been observed in economically disadvantaged adolescents (Porto et al. 1994, Silveira et al. 1999, Clemens et al. 2000, Gandolfo et al. 2003). Hepatitis B vaccination is the most effective strategy for HBV prevention. In Brazil, it has been available in private clinics since the beginning of 1990s, but due the elevated cost of doses only individuals with better socioeconomic conditions could be vaccinated. In 1999, in compliance with WHO recommendations (WHO 2003) the Brazilian Public Health Authorities implemented the universal hepatitis B vaccination for newborns and infants, and more recently it was extended for adolescents. Actually several countries manufacture the hepatitis B vaccines. This should play a role in the cost of doses and to improve the worldwide hepatitis B vaccine coverage, mainly in developing regions (Vryheid et al. 2000). Butang® is a Brazilian hepatitis B recombinant vaccine (Ioshimoto et al. 1999). It has been provided free of charge by health public services since 2001. However, there is still few informations about the immunogenicity of this vaccine in different groups (Baldy et al. 2004, Martins et al. 2004). In order to assist decisions on strategies for hepatitis B vaccination in a target group of the Brazilian immunization program, an investigation was carried out to evaluate the prevalence and risk factors for HBV infection, the adherence to and the antibody response to Butang® vaccination in low-income scholar adolescents in Goiânia city, Central Brazil. MATERIAL AND METHODS Subjects - The study was carried out between November 2003 and November 2004 in public schools in a low income region in the Metropolitan Area of Goiânia city (1,600,000 inhabitants), state of Goiás, Central Brazil. In the region, there are five public schools attending adolescents. The objectives of the investigation were presented to their directors, and the two largest schools (School A and School B) complained with the study. To evaluate the prevalence and risk factors for HBV infection, the study sample was calculated on the basis of an alpha error of 5%, an expected anti-HBc prevalence of 9% (Clemens et al. 2000), precision of 3%, and a design effect of 2%. In accordance with theses data, the sample size necessary was 674 adolescents. They were recruited using a systematic sampling method. Ten individuals refused to participate. Thus, 664 individuals (12 to 19 years old) matriculated on November 2003 in the School A and School B were included in the study who represented a participation of 98.5%. Informed consent was obtained for enrollment in the investigation and also for administration of vaccination series. Subjects younger than 18 years required parental consent. The study was approved by the Research Ethics Committee of Hospital da Santa Casa de Misericórdia de Goiânia, Goiás (protocol 011/03). Initially, all 664 adolescents were interviewed face-to-face using a standard questionnaire regarding socio-demographic: sex, age, birthplace, and household income; school: A or B; and HBV risk factors during lifetime: sexual activity (homo or heterosexual), previous sexual transmitted disease-STD, number of sexual partners, age at first sexual intercourse, prostitution, sexual abuse, consume of alcohol and illicit drugs, prison, homeless experience, tattooing, and body piercing. Adolescents were assured that their information would not be shared with parents and school staff. Serological tests - Blood samples were collected from all participants and sera were stored at -20ºC. They were screened for hepatitis B surface antigen (HBsAg), hepatitis B core antibody (anti-HBc), and hepatitis B surface antibody (anti-HBs) by enzyme-linked immunoabsorbent assays (ELISA) (Abbott Laboratories, US). Samples that presented isolated reactivity for anti-HBc or HBsAg were retested. HBV vaccination - Individuals not reactive for HBV infection markers (n = 304) were invited to vaccination. In the adolescent group that agreed with immunization, three doses of 20 µg at 0, 1, and 6-month intervals of the Brazilian recombinant hepatitis B vaccine (Butang®; Instituto Butantan, Brazil) were administered. Adverse effects of immunization such as injection site reactions, fever, and malaise were recorded by passive report. Post-vaccination samples were taken from all subjects one month after the third dose. The quantitative anti-HBs antibody was determined by automatic analysis using the Microparticle Immunoenzymatic Test AxSYM® Ausab® (Abbott, Germany). Samples with anti-HBs > 1000 mIU/ml were diluted 1:10 and re-tested. The criterion for protection was defined as concentration of anti-HBs equal to or higher than 10 mIU/ml. Statistical analysis - For analyses, the positivity for the HBsAg and/or anti-HBc markers was considered HBV infection. Prevalence and 95% confidence intervals (95% CI) were calculated. Student's t test (continuous variable), Chi-square test, and Fisher's exact test (categorical variables) were used to compare variables and to evaluate association between HBV positivity and risk factors. These, estimated by odds ratio in univariate analysis, were further analyzed by stepwise logistic regression model to identify possible confounders. Statistical significance was assessed at the 0.05 probability level in all analyses. The geometric mean of anti-HBs titres (GMT) was calculated with 95% CI. Statistical evaluations were performed using SPSS version 11.0 (SPSS Inc., Chicago, US, 1999). The mean age of the adolescents investigated was 15.2 years (standard deviation = 2.1). Two hundred sixty four (39.8%) were males and 400 females (60.2%). A total of 383 (59.2%) individuals were born in the state of Goiás. The remainder was from other Brazilian states. Almost the totality reported a household income equal or less than US $100 per month. They were matriculated in the two largest school of the region. There were not statistical difference between the schools regarding age, sex and socioeconomic conditions of the adolescents (p < 0.05). As shown in Table I, 39 of 664 adolescents (5.9%; 95% CI: 4.2-8.0) were exposed to HBV. Of them, four were infected since they were HBsAg-reactive. Twenty-four had been infected and developed natural immunity, and 11 were positive for anti-HBc only. Three hundred twenty-one were reactive for anti-HBs alone, suggesting previous HBV vaccination. Global HBV prevalence increased significantly with age, rising from 2.4% in the 12-13 (95% CI: 0.7-6.3) age group to 17.3% (95% CI: 11.0-26.0) in those with 18-19 years (χ2 = 19.7; p = .00) (Fig. 1). Individuals with previous serological evidence of HBV vaccination were excluded for HBV risk factors analysis. The prevalence of HBV infection markers was significantly higher for those adolescents in the older age-group (p < 0.05), those who were born in other Brazilian states (p < 0.05), those that were attending in school B (p < 0.05) and those who reported sexual activity (p < 0.05) in univariate analysis. These variables and body piercing that showed a marginal HBV association (χ2 = 3.83; p = 0.05) were included in a stepwise regression logistic model. Then, when demographic characteristics and potential confounders were controlled, age 16-19 years (OR = 3.6; CI 95%: 1.6-7.9), place of birth outside Goiás (OR = 3.4; 95% CI: 1.6-7.3), school "B" (OR = 2.4 fold; 95% CI: 1.2-4.9), and body piercing (OR = 3.3; 95% CI: 1.1-10.0) were independently associated with HBV infection markers (Table II). The variables sexual abuse, multiple partners, previous prison, homeless, tattooing, illicit drug, and alcohol use were more frequently found in adolescents who were HBV reactive than those who were not, however, they did not reach statistic significance. A total of 304 subjects were eligible for HBV immunization. Nevertheless, only 195 (64.1%) accepted the first vaccine dose and 182 (93.3%) the three doses. Among them, 170 (93.4%) were tested for quantitative anti-HBs. All responded to Butang® vaccine. One subject (0.6%) presented anti-HBs titer between 10-100 mIU/ml. Anti-HBs titers between 101-1000 mIU/ml were detected in 16.5%. Fifty percent developed anti-HBs titers between 1001-10,000 mUI/ml, and titers higher than 10,000 mUI/ml were detected in 32.9% (Fig. 2). Also, a GMT of 4344 mUI/ml (95% IC: 3492 - 5404) was obtained. DISCUSSION Although Brazil has been globally considered an area of intermediate HBV endemicity, variable rates has been found in all five Brazilian regions and even inside the same region (Souto 1999). Goiânia city have been appointed as a low HBV endemicity area (Martelli et al. 1999). Our findings in low income adolescents ratify this assumption. In this study, we found a prevalence of HBV infection of 5.9% in adolescents. This is higher when compared with data in adolescents and young adults from developed countries where hepatitis B vaccination programs were fully implemented such as Greece (2.5%) (Gogos et al. 2003), Italy (0.9%) (Bonanni et al. 2003), Spain (0.9%) (Salleras et al. 2005), and the United States (1%) (McQuillan et al. 1989). However, regarding individuals from developing regions where HBV vaccination programs were partially or not implemented, this prevalence was similar to that observed in Mexico (5%) (Cisneros-Castolo et al. 2001) and Bolivia (6.9%) (Gandolfo et al. 2003). In Brazil, Clemens et al. (2000) reported a rate of 5.2% in adolescents of four regions, ranging from 2.5% in those with better socioeconomic conditions to 9% in lowincome individuals. After adjustment by age, an increasing HBV infection prevalence was observed. This has also been observed by others (Dominguez et al. 2000, Cisneros-Castolo et al. 2001, Gandolfo et al. 2003). More, older adolescents had 3.6 fold (95% CI: 1.6-7.9) more chance to be exposed to HBV than those younger, suggesting changes in the lifestyle linked with risk behaviors for hepatitis B transmission. In this investigation, most adolescents positive for HBV infection markers were born in the Brazilian northern states (data not shown). This could have contributed for the finding that individuals who were born outside the state of Goiás had greater likelihood of HBV positivity than those from Goiás, highlighting the importance of migratory movement to HBV dissemination (Passos et al. 1993, Souto et al. 1998). The expansion of the regional industry and the development of agriculture and cattle breeding have increased the migratory flow of persons into Central Brazil. Thus, in countries as Brazil with continental dimensions and unequal social conditions where different HBV rates may be detected in a single region, this variable should be always stressed in epidemiological studies. Although there was not statistical difference among the adolescents matriculated in School A and School B regarding household income, age and sex, those attending School B had twice more chance to be positive for HBV infection markers. School B is close to a larger truck stop where commercial sex workers are frequently found. Perhaps this unsafe environment may have contributed with the present finding since higher prevalence of sexually transmitted diseases has been found at places where truck drivers traditionally halt (Gawande et al. 2000, Gibney et al. 2001, Manjunath et al. 2002). Individuals using body piercing have been associated with greater risk for hepatitis B when compared with those not pierced (Hayes & Harkness 2001). This was also found in the present investigation highlighting the potential risk of viral dissemination through cosmetic skin penetration practices. Further, since in studies of sexual behavior the validity of self-reported behavioral variables may be limited (Lauritsen & Swicegood 1997, Carroll et al. 2002, Roberts & Ryan 2002), for some authors body piercing may also serve as a presumed proxy measure for risk behaviors. In fact, in the present investigation the majority of adolescents using body piercing reported unprotected sex, alcohol, and drug use (data not shown). Finally, the findings of sexual experience should be considered with reserves since the sexual activity has been appointed as one of the major cause of HBV transmission in low endemicity region (Hou et al. 2005). As above mentioned when behavioral variables are investigated response bias should be considered even when all strategies to reduce it were done. Hepatitis B vaccination in adolescents represents a great challenge for health care provider. Generally a poor compliance with vaccination has been observed in these individuals (Lawrence & Goldstein 1995). Indeed the HBV vaccine was offered for all susceptible adolescents, but only 64% accepted it. Otherwise among those vaccinated almost the totality (93.3%) received the complete vaccine series. Others have also reported a better compliance with full scheme in school-based HBV immunization programs (Seid et al. 2001, Zuckerman & Langer 2005), reinforcing the convenience of this strategy to achieve this target group for hepatitis B vaccination. Although in immunocompetent youths the seropro-tection rates following the three-doses series are similar using 10 or 20 µg, the latter provides higher geometric means titers (Schiff et al. 1995, Turchi et al. 1997). In this investigation, all subjects responded to 20 µg of the Butang® vaccine with developing anti-HBs titers higher than 1000 mUI/ml. Also, a GMT of 4344 mUI/ml (95% IC: 3492-5404) was obtained. This was more than five times the geometric mean titer of anti-HBs previously reported using doses of 10 µg of the Butang®, and even more than twice using the Engerix B® vaccine (Baldy et al. 2004, Martins et al. 2004). Since long-term response associated with duration of protection seems proportional to the peak of post-vaccination anti-HBs levels, and that this could provide an indication of duration of protection (Assad & Francis 2000, Whittle et al. 2002), the present vaccine scheme for early adolescent should guarantee protective anti-HBs levels at a critical time for hepatitis B acquiring such as latter adolescence and adulthood. In conclusion, the increasing of hepatitis B markers along the adolescence reinforces the benefits of vaccination before engagement in activities that put the individual at risk for HBV infection. Therefore larger efforts should be done to increase the hepatitis B vaccine coverage in adolescents in despite of the regional HBV endemicity. The school-based immunization could be one strategy. ACKNOWLEDGEMENTS To Isolina Maria Xavier Rodrigues for technical support, and Elaine Maria Xavier Seronni for English revision of the manuscript. REFERENCES
Copyright 2006 Instituto Oswaldo Cruz - Fiocruz |

{kind=link}
{kind=link}
{kind=link}
{kind=link}