 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Seropositivity for hepatitis B virus, vaccination coverage, and vaccine response in dentists from Campo Grande, Mato Grosso do Sul, Brazil Sonia MF Batista/+, Márcia SA Andreasi, Ana MT Borges*, Andréa SC Lindenberg**, Anísio L Silva, Thiago D Fernandes, Edy F Pereira, Eline AM Basmage***, Divina DP Cardoso* Departamento de Patologia, Centro de Ciências Biológicas e da Saúde, Universidade Federal de Mato Grosso do Sul, Cidade Universitária, 79070-900 Campo Grande, MS, Brasil *Instituto de Patologia Tropical e Saúde Pública, Universidade Federal de Goiás, Goiânia, GO, Brasil **Centro Especial de Doenças Infecciosas e Parasitárias, Hospital Dia, Nova Bahia, Campo Grande, MS, Brasil ***Laboratório Central de Saúde Pública de Mato Grosso do Sul, Campo Grande, MS, Brasil Financial
support: Secretaria de Estado de Saúde, Conselho Regional
de Odontologia de Mato Grosso do Sul, Universidade Federal de Mato
Grosso do Sul, Universidade Federal de Goiás Received
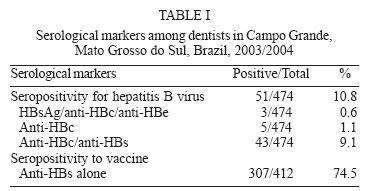
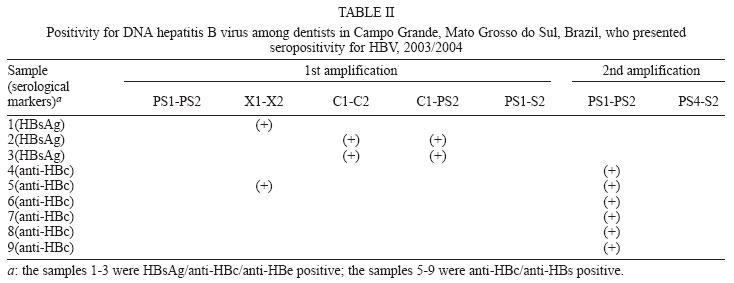
20 October 2005 Code Number: oc06046 This study investigated the seropositivity for hepatitis B virus (HBV), the vaccination index, and the vaccine response index in dentists from Campo Grande, MS. Blood samples from 474 dentists (63.7% women and 36.3% men), with a mean age of 38.5 ± 10.5 years were analyzed by enzyme-linked immunosorbent assay to detect the serological markers: HBsAg, anti-HBs, and anti-HBc. The HBsAg positive samples were tested for anti-HBc IgM, HBeAg, and anti-HBe. A total of 51 (10.8%) dentists showed seropositivity for HBV. Three (0.6%) were HBsAg/anti-HBc/anti-HBe positive, 43 (9.1%) were anti-HBc/anti-HBs positive, and 5 (1.1%) had only anti-HBc. Viral DNA was detected by polymerase chain reaction in 9 (17.6%) out of 51 HBV seropositive samples. A vaccination index of 96.6% (458/474) was observed, although 73.1% (335/458) completed the three-dose schedule. Excluding 46 HBV seropositive individuals from 458 that reported vaccination, 412 were analyzed for vaccine response index. It was observed that 74.5% (307/412) were anti-HBs positive; this percentage increased to 79.1% when three doses were administered. The results showed a high vaccination index and a good rate of vaccine response; however, the failure in completing the three-dose schedule and the occurrence of HBV infection reinforce the need for more effective prevention strategies. Key words: hepatitis B - dentists - vaccination - seroprevalence - Brazil The hepatitis B virus (HBV) is a causal agent of hepatitis, which is asymptomatic in most individuals, but it can show features of fulminant, acute, or chronic hepatitis, considering that the last one might evolve to serious complications, such as cirrhosis and hepatocellular carcinoma (Ganem & Prince 2004). Each year, from 500,000 to 1.2 million individuals die as a consequence of HBV infection (Lavanchy 2004). Studies carried out in the pre-vaccination era showed that HBV infection in dentists was about three to six times greater than in the general population (Feldman & Schiff 1975, Smith et al. 1976). Since the manufacturing of the first vaccines against HBV in 1982, and with the increase in the vaccination coverage, the prevalence of infection has been gradually falling (Cleveland 1996, Mahoney et al. 1997). The hepatitis B vaccination coverage among dentists is highly variable and it is not yet compatible with the possible elimination of the occupational risk of HBV infection (Camilo 1998, Ammon et al. 2000, Rodrigues 2002, Martins & Barreto 2003), considering the fact that these professionals are in continuous exposure to blood or other fluids potentially contaminated with HBV (Cleveland & Cardo 2003). This study presents the seropositivity for HBV, the vaccination index, and the vaccine response index in dentists from Campo Grande, state of Mato Grosso do Sul (MS), Brazil. Furthermore, HBV infection and putative association with epidemiological features were also investigated, considering that there is no information about this population group in MS. MATERIALS AND METHODS Studied population - From 1222 dentists associated to the Regional Odontology Council (Campo Grande, Mato Grosso do Sul), 474 subjects were randomly selected and invited to participate in this study. This sample was considered sufficient to detect seropositivity for HBV infection of 20% with an accuracy of 3%. The blood samples were collected between August 2003 and November 2004. The Ethical Committee of the Federal University of Mato Grosso do Sul approved the study protocol. Informed consents were obtained from all dentists and a standardized questionnaire was used to collect sociodemographic, epidemiological information, and vaccination data. Detection of HBV serological markers - All blood samples were tested in duplicate, using a commercial immunoassay (DiaSorin, Italy), in order to detect the following serological markers: HBsAg, anti-HBs, and anti-HBc. The HBsAg positive samples were also tested for anti-HBc IgM, HBeAg, and anti-HBe. In accordance with the positivity criteria established by this kit, the anti-HBs positive samples had concentration of antibody higher than 10 mIU/ml. In the present study, HBV infection was defined as the presence of the serological marker anti-HBc, associated or not with HBsAg or anti-HBs. All participants were notified of the results by mail and were provided with an interpretation of their serological markers. The dentists with HBsAg positive serological test were referred for clinical evaluation. Vaccination and vaccine response indices - All dentists that reported previous vaccination were considered for the vaccination index analysis. The subjects that reported previous vaccination and had no serological marker for HBV infection were considered for the vaccine response index analysis. Viral DNA detection - The positive samples for HBsAg, as well as those positive for anti-HBc associated or not with anti-HBs, were analyzed to detect viral DNA by polymerase chain reaction (PCR). The viral DNA was extracted from serum and amplified as described previously by Niel et al. (1994). The oligonucleotides used as primers were: PS1 5'CCATATTCTTGGGAACAAGA3' (nt 2826-2845), PS2 5'GGTCCCCAGTCCTCGAGAAG3' (nt 124-143), X1 5'ACCTCCTTTCCATGGCTGCT3' (nt 1363-1382), X2 5'TAGGCAGAGGTGAAAAAGTT3' (nt 1818-1837), C1 5'CTGTGGAGTTACTCTCGTTTTTGC3' (nt 1935-1958), C2 5'CTAACATTGAGATTCCCGAGATTG3' (nt 2432-2458), S2 5'GGGTTTAAATGTATACCCAAA GA3' (nt 841-819), PS4 5'ACACTCATCCTCAGG CCATGCAGTG3' (nt 3194-3218) (Niel et al. 1994, Gomes et al. 1996). In the first round of amplification, the primer pairs PS1-PS2, X1-X2, C1-C2, C1-PS2, PS1-S2 were used to amplify five HBV fragments. The negative samples were submitted to a second amplification (semi-nested PCR) using primer pairs PS1-PS2 and PS4-S2 for products of C1-PS2 and PS1-S2, respectively. The utilized PCR procedure is able to detect 100 copies per genome (Gomes SA, pers. commun.). Statistical analysis - The data were analyzed using the EPINFO 6.04 (Centers for Disease Control and Prevention, Atlanta, GA, US, 1997) statistical software package. Chi-square test and Fisher's exact test with 95% confidence intervals were used when appropriate. Results were considered significant when p value <0.05. Among 474 dentists, 302 (63.7%) were female and 172 (36.3%) were male. Their age ranged from 21 to 69 years, with a mean age of 38.5 ± 10.5 years. More than 50% of the dentists were married (60.7%), had a professional specialty (57.4%), had up to 20 years of professional practice (72.1%), and practiced in both private clinics and public service (65.5%). According to the results of serological tests performed on 474 dentists, 51 (10.8%) showed seropositivity for HBV infection. Three subjects (0.6%) were HBsAg/anti-HBc/anti-HBe positive, 43 (9.1%) were anti-HBc/anti-HBs positive, and five (1.1%) presented reactivity for only anti-HBc (Table I). A significant association was observed between HBV infection and older age (χ2 = 17.97; p = 0.00) and longer duration of professional career (years of professional practice (χ2 = 12.65; p = 0.00). A higher frequency of HBV infection was also found among dentists who informed an irregular use of protective glasses (18.6 vs 9% p = 0.01) and clothing (18.3 vs 8.9% p = 0.01), in comparison to their counterparts. HBV-DNA was detected in 9/51(17.6%) of HBV seropositive samples. All HBsAg positive samples, 3/3 (100%), were also positive for HBV-DNA in the first amplification reaction. Moreover, HBV-DNA was detected in 1 (n = 5) and 6 (n = 43) of anti-HBc (sole marker) and anti-HBc/anti-HBs positive samples, respectively. Five out of 48 samples with anti-HBc, associated or not with anti-HBs, presented positivity only in the second amplification reaction (Table II). Among the participants of this study, 458/474 (96.6%) reported vaccination against HBV. From these, 335/458 (73.1%) received the three recommended doses and only 26/458 (5.7%) reported a post-vaccination serological test for anti-HBs. HBV vaccination was significantly lower among dentists who informed older age (91.5 vs 99.2%, p = 0.00) and older duration of professional practice (91.7 vs 99.4%, p = 0.00). Excluding 46 individuals that presented any serological marker for HBV infection from those 458 subjects who reported previous vaccination, 412 dentists were analyzed for the vaccine response index (Table I). It was observed that 307 (74.5%) subjects presented seropositivity for the HBV vaccine; taking into consideration the three doses, the index increased to 79.1%, which was significantly higher than those who received one or two doses of the vaccine (p = 0.04). No significant difference in the vaccine response index was observed in relation to gender, vaccination schedule, vaccine administration route, and vaccine site (p > 0.05). For dentists who received the third dose of the vaccine one year before the participation in this study, the vaccine response index was 95.7%, significantly higher than those who completed the three-dose schedule in a period longer than one year before (76%) (p = 0.00). Among 458 dentists who reported previous vaccination, 105 subjects were negative for all serological markers tested. From these, 97 (92.4%) received the last dose of the vaccine in a period longer than one year before the participation in this study. DISCUSSION The present study showed that seropositivity for HBV infection among dentists (10.8%) from Campo Grande, MS, was higher than that recorded among blood donors (9.4%) in the same city (Aguiar et al. 2001). In dentists from the other regions of Brazil, the infection rates ranged from 10 to 17.9% (Ozaki et al. 1998, Camilo 1998, Rodrigues 2002). On the other hand, it was observed 9% of seropositivity for HBV infection among dentists from the United States (Cleveland 1996) and 7% among dentists from Berlin, in Germany (Ammon et al. 2000). Studies carried out among dentists in the pre-vaccination years showed 15% of seropositivity for HBV infection in the United States (Gruninger et al. 1991) and 23.3 to 31.2% in Brazil (Ottoni et al. 1995, Baldy 1995). In this study, HBV seropositivity significantly increased with age and duration of professional practice. This is in accordance with other studies (Ottoni et al. 1995, Cleveland 1996, Camilo 1998, Rodrigues 2002). Consistent with previous findings (Ammon et al. 2000), our findings highlight the role of protective glasses and clothing use as preventive measures for HBV infection among dentists. Among 51 HBV-seropositive dentists, 46 subjects reported previous HBV vaccination. Among these, 33 received the three recommended doses. It was considered that the infection had possibly occurred before the vaccination; or, yet, that these professionals were non-responders to the vaccine and, in the susceptible condition, ran the same risk of acquiring infection as the non-vaccinated subjects. The frequency of HBV-DNA in both anti-HBc/anti-HBs and anti-HBc (sole marker) positive groups is in accordance with the literature (Gomes et al. 1996, Bréchot et al. 2001, Minuk et al. 2005) and suggest that HBV infection might persist in individuals with a serological profile of resolved infection. In the present study, the majority of the dentists (96.6%) reported HBV vaccination, although only 73.1% completed the three-dose schedule. Nevertheless, the percentage of adhesion of these professionals to HBV immunization is considered higher than those observed in other studies (Cleveland 1996, Camilo 1998, Ammon et al. 2000) as among health-care workers (HCWs) (Silva et al. 2003, 2005). In Brazil studies have shown vaccination indices similar to those observed in the present study (Rodrigues 2002, Martins & Barreto 2003). In spite of high compliance with HBV vaccination, more efforts are necessary for dentists to receive full-scheme (three vaccine doses). HBV vaccination was lower among dentists who informed older age and longer duration of professional practice, which is in accordance with previous studies (Cleveland 1996, Camilo 1998, Rodrigues 2002, Martins & Barreto 2003). In this study, among those with full-scheme vaccination, only 5.7% subjects reported the post-vaccination test, which is in agreement with other studies (Cleveland et al. 1994, Sorabjee & Garje 2004, Saffar et al. 2005, Oh et al. 2005). These data suggest that dentists should be counseled to detect anti-HBs one or two months after completing the three-dose vaccination series. Vaccine response was higher among subjects who completed the three-dose schedule, in comparison with those who only received one or two vaccine doses. Furthermore, the frequency of vaccine response was significantly lower among older subjects, in accordance with other authors (Ferraz et al. 1992, Cleveland et al. 1994, Cuevas et al. 1997, Averhoff et al. 1998, Arca et al. 1998, Silva et al. 2005). Consistent with previous investigations (Zumaeta et al. 1995, Prakash et al. 2000), differences in vaccine response were not observed regarding gender, smoking status, vaccination schedule, vaccine administration route, and vaccine site, although females and non-smokers are more likely to demonstrate high vaccine response (Cleveland et al. 1994, Averhoff et al. 1998). After vaccination, a gradual decline in anti-HBs titers is frequently found (Floreani et al. 2004). Corroborating other studies (Ferraz et al. 1992, Oliveira 1997, Cuevas et al. 1997, Turchi et al. 1997, Arca et al. 1998, Lopes et al. 2001), we observed that the vaccine response index was significantly higher among dentists who received the third dose up to one year before the interview, compared to their counterparts. In our study, about one third of dentists were non-responders for HBV immunization (whose susceptible status was generally unknown). Therefore, these subjects are still under risk for HBV infection, especially due to the background prevalence reported in MS (Motta-Castro et al. 2003, 2005). To effectively curb HBV infection in this setting, prevention programs must be reinforced, and the relevance of a complete vaccination schedule must be underlined. REFERENCES
Copyright 2006 Instituto Oswaldo Cruz - Fiocruz |

{kind=link}
{kind=link}