 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memórias do Instituto Oswaldo Cruz, Vol. 101, No. 5, August, 2006, pp. 517-521 IS6110 restriction fragment length polymorphism typing of Mycobacterium tuberculosis isolates from East Azerbaijan Province of Iran Mohamad Asgharzadeh, Karen Shahbabian*/+, Jafar Majidi, Ahmad Mirza Aghazadeh, Cirus Amini**, Ali Reza Jahantabi*, Abdolnaser Rafi** Drug Applied Research
Center *Department of Microbiology, School of Medicine **Research Center
for TB and Pulmonary Diseases, Tabriz University of Medical Sciences, Tabriz,
Iran Financial support: Drug Applied Research Center, Tabriz University of Medical Sciences Received 6 December
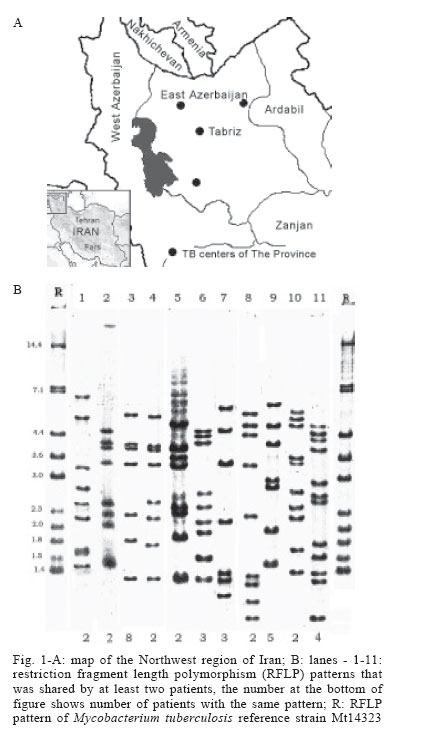
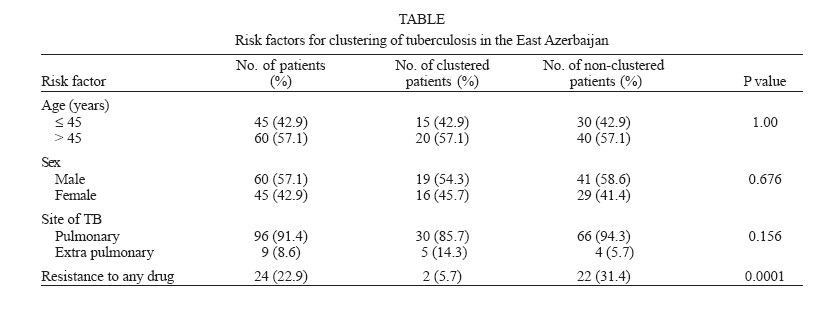
2005 Code Number: oc06087 To investigate the genetic variation among Mycobacterium tuberculosis isolates in the East Azerbaijan Province of Iran and to evaluate the level of and risk factors for recent transmission of tuberculosis (TB), we performed IS6110-based restriction fragment length polymorphism analysis of strains, isolated from 105 patients during the period of September 2002 to March 2003 in TB centers and university hospitals of the province. Among 105 isolates, 81 different IS6110 patterns were found, of which 70 were observed only once and 11 were shared by two to eight isolates. Ninety-six isolates (91.4%) were found to have more than five copies of IS6110 and together with high patterns polymorphism, shows that IS6110-RFLP typing could be useful for studying the epidemiology of TB in Azerbaijan. The minimum estimated rate of recent transmission was 23%, suggesting that the degree of recent transmission in East Azerbaijan Province is relatively low. Clustering was not associated with age, sex or site of infection of TB but drug-resistant isolates were less likely to be clustered than sensitive isolates (p < 0.05). Key words: tuberculosis - restriction fragment length polymorphism - IS6110 - Iran DNA fingerprinting of Mycobacterium tuberculosis is a valuable tool to study tuberculosis (TB) epidemiology. many other studies on this methodology have been done in various parts of the world including developed and developing countries (Pineda-Garcia et al. 1997, Gutierrez et al. 1998, Dahle et al. 2001, Diaz et al. 2001, Bhanu et al 2002). The method of fingerprinting based on IS6110 repetitive element has become standard (Hermans et al. 1990, Van Embden et al. 1993) and its stability (Niemann et al. 2000, Warren et al. 2002) and discriminatory power have been proven (Kremer et al. 1999). The usefulness of DNA fingerprinting has already been defined in source tracing (Kiers et al. 1997) and understanding of TB transmission in the general population (Alland et al. 1994). Fingerprinting results from various parts of the world demonstrate that in areas with low incidence of TB, the majority of cases are due to reactivation of previous infection whereas in high incidence areas reinfection is responsible for the majority of TB cases (Alland et al. 1994, Dahle et al. 2001) but there are some exceptions (Bauer et al. 1998, Narayanan et al. 2002). The East Azerbaijan Province is located in the North West of Iran, in neighbor-hood of Nakhichevan state of Republic of Azerbaijan (Fig. 1A). The estimated population of the Province is 3,500,000 of which about two-fifth are inhabitants of Tabriz, the capital city of the Province. The estimated rate of TB in Iran in 2002 was 29 in 100,000 and notification rate is 17 in 100,000 (WHO 2004). However, TB incidence is not homogeneous in different parts of this country. In East Azerbaijan Province the estimated rate of TB in 2002 was low; this can be due both to low case finding or low prevalence of TB in this part of the country. The aims of this study were to determine the genetic diversity of M. tuberculosis population in East Azerbaijan Province, and to detect the manner of transmission of the disease in this area. MATERIALS AND METHODS Patient population and bacterial isolates - The study population comprised all patients with TB confirmed by culture from September 2002 to March 2003 in TB centers and university hospitals of the province. Information about age, sex, geographical origin, and history of tuberculosis were recorded. The species identification of the isolates was based on polymerase chain reaction (PCR) method and standard microbiological tests. The susceptibilities of the isolates to isoniazid (INH), rifampin (RF), streptomycin (SM), and ethambutol (ETB) were determined by the proportional method. Restriction fragment length polymorphism analysis - RFLP analysis was performed as described previously (Van soolingen et al. 1994). Briefly, extracted mycobacterial DNA was digested with PvuII, subjected to electrophoresis, and hybridized with a 245-bp PCR-amplified probe directed against the right arm of IS6110. After hybridization, the insertion sequences were visualized with a colorimetric system, the DIG DNA labeling and detection kit (Roche, Germany) by following the manufacturer's instructions. A mixture of PvuII-digested supercoiled DNA ladder (Sigma) and HaeIII-digested ΦX174 DNA (Fermentas) was used as an internal marker. PvuII-digested genomic DNA of M. tuberculosis reference strain Mt14323 was used as an external marker in each gel (Van Embden et al. 1993). The IS6110 fingerprint patterns were compared by visual examination. A cluster of M. tuberculosis was defined as two or more isolates which exhibited the same number of copies of the IS6110 fragment with identical molecular sizes. The IS6110 RFLP patterns obtained from this region were compared to those, available from previous studies in various parts of the country. Statistical analysis was carried out by using the chi-square test (or Fisher's exact test, when expected values were five or less) and student's t-test. P values below 0.05 were considered statistically significant. RESULTS Patients and isolates - During the study period, out of 154 samples that were collected and submitted for culture, 125 (81%) M. tuberculosis isolates have been obtained. Clinical isolates were recovered from sputum (n = 97), bronchial fluids (n = 19), abscess aspirates (n = 2), urine (n = 2), cerebrospinal fluids (n = 2), pleural fluid (n = 1), endometrial biopsy (n = 1), and neck mass biopsy (n = 1). Six of the isolates could not be used for RFLP analysis; therefore the RFLP patterns of 119 isolates from 119 patients were determined. Fourteen strains were excluded because they were isolated from Nakhichevaneese patients, but the patterns compared with Iranian strains' patterns for detecting probable transmission of the infection. Therefore, our study group consisted of 105 patients, who had no history of previous TB. The age of the patients ranged from 12 to 90 years which young patients (≤ 45 yrs old) represented 43% of study population. The male to female ratio was 1.3:1. Eighty-one (77%) of the 105 strains were susceptible to INH, RF, SM, and ETB. Twenty-three percent of the strains were found to be resistant to at least one drug, with 15.2% of the strains resistant to SM, 9.5% resistant to INH, 5.7% resistant to RF, and one strain resistant to ETB. Among these strains, two strains were multi-drug-resistant (MDR). IS6110 RFLP clustering - The copy number of IS6110 in each of the isolates was determined from the number of bands hybridizing with the probe. The number of IS6110 copies per isolates varied from zero to 18. Most strains (91.4%) carried six or more IS6110 copies. Nine strains (8.6%) contained less than six copies of IS6110, of which four strains had five copies, one strain had four copies, one strain had three copies, and three strains had no copies of IS6110; none of the low-copy number patterns (except zero-copy patterns) belonged to a cluster. Eighty-one distinct IS6110 RFLP patterns were revealed: 70 of these patterns were unique and 11 were shared by two to eight strains. Thirty-five strains (33.3%), belonging to one of 11 clusters (Fig. 1B) were found among the total 105 strains. The rate of diversity of the patterns by RFLP analysis with IS6110 for the M. tuberculosis strains in this study was 77.1%. the minimum estimate for the proportion of TB that was due to transmission in East Azerbaijan Province is 23% [(35-11)/105]. If low-copy number strains would have been included, clustering would even be less. Characteristics of the clusters - The largest cluster comprised eight patients, who were all residents of Tabriz. Five of these patients were female and three of them knew each other; although our epidemiologic data do not allow to confirm this, transmission by contact or by frequenting the same place. The rest were residents from different parts of the city and no epidemiological linking was detected; however, all were suffering from poor living conditions. The second cluster was made up of five patients: three were from Tabriz and the others were from Maraghe, about 200 km away from Tabriz; no connection between the patients was detected. Another cluster was composed of four patients from different cities around Tabriz; two of them would commute to Tabiz. Two other clusters harbored three patients and the remaining six clusters comprised two patients, who were all from Tabriz. One of the smallest clusters containing two Iranian patients shared RFLP pattern with one strain of Nakhichevaneese patient that shows the transmission of infection probably from that region. Comparison of IS6110 RFLP patterns with other Iranian strains - The clustered and non-clustered patterns were compared to those of other 192 patterns that were previously obtained from various parts of the country (of these 192 patterns, 54 were previously obtained from North-West of Iran). Out of 11 clusters of our study only one (2.8% of isolates) was found to have the same pattern as an isolate that was previously observed in Northwest of Iran. Non-clustered isolates shared 21 RFLP fingerprints (20% of isolates) with other Iranian strains, however, by removing previous patterns of the region from the comparison the percentage of identical patterns reduced to 6.6%. Risk factors associated with clustering - to identify risk factors associated with recent transmission, 35 clustered patients were compared with 70 non-clustered patients (Table). We did not observe any statistically significant differences in the rate of clustering for age, sex and site of TB (p > 0.05). Among isolates, 40.7% of drug-sensitive strains compared with 8.3% of drug-resistant strains, were clustered. The resistant strains were harbored in two smallest clusters, one strain was SM and INH resistant and the other was INH resistant. Statistical analysis showed significant differences between clustered and non-clustered patients for resistant to any drug (p < 0.05). DISCUSSION IS6110-based DNA fingerprinting of M. tuberculosis has proven to be highly effective in detecting the sources of infection and in providing data for improving the control programs of tuberculosis. In this study, we used IS6110-RFLP typing to investigate active tuberculosis transmission in East Azerbaijan Province of Iran. Of the 105 isolates in this study, nine strains (8.6%) showed fewer than six copies of Is6110. Other studies showed similar data: 5.4% of strains from Tehran (Farnia et al. 2004) and 3.2 % of strains from Fars Province had low copies of IS6110 (Doroudchi et al. 2000). Interestingly, very different data were obtained from khorasan Province, where 38% of the isolates showed low or no copies of IS6110 (Farnia et al. 2001). The percentage of isolates containing low copy number of IS6110 in East Azerbaijan is lower than that observed in regions such as Malaysia (Dale et al. 1999), India (Narayanan et al. 2002), and Turkey (Durmaz et al. 2003). These finding indicate that IS6110-RFLP typing can be used without additional typing markers for this area. Also, our study detected 11 clusters, of which the majority was comprised of two or three patients; such data suggest that tuberculosis in this region of Iran is likely due to micro-epidemics. By comparing our patterns with those obtained in previous studies, only seven isolates had RFLP patterns identical to patterns observed previously in other parts of the country. This low rate of similarity was also reported by Farnia et al. (2001) and is probably due to the distance between the studied areas and the lack of immigration between the areas. However, since RFLP analysis was not performed in all regions of the country, including in neighboring provinces, the true extent of clustering among patients of this region with patients elsewhere in Iran is probably underestimated. We found 33.3% clustering among m. tuberculosis strains, suggesting that the majority of the tuberculosis cases in East Azerbaijan are due to reactivation. It is known that in mixed populations the degree of DNA polymorphism is greater (Van Embden et al. 1993). Although immigration from other parts of the country is almost inexistent in Tabriz, there is considerable number of patients from Nakhichevan (during our study, 11.8% of the initial strains were isolated from Nakhichevaneese patients); these could import new strains and lead to the high genetic diversity of M. tuberculosis genotypes. Furthermore, it should be noticed that the study was performed during a period of six months only, and because of the characteristics of disease transmission and development, a study using a larger time frame should be performed to evaluate the real clustering rate. In a study on TB transmission in Paris, male sex is a risk factor for TB-clustering (Gutirrez et al. 1998). In the present study however, clustering, although not significant, was higher for female than for male TB patients. this might be due to discrimination of the female population, as reflected by lower education, more poverty, and malnutrition. Generally, young age is a risk factor for recent transmission (Alland et al. 1994, Small et al. 1994, Maguire et al. 2002) but in our study, no difference was observed between the younger or older age categories; unemployment and generalized poor living condition could be the reason for this. Another contrast to other studies (Shafer et al. 1995, Kruuner et al. 2001, Vukovic et al. 2003) was our findings that drug-resistant strains are less likely to be in a cluster than drug-sensitive strains (p = 0.0001). It has been suggested that drug sensitive strains are more transmissible and the absence of drug resistant strains in the largest clusters supports this suggestion. We can conclude that IS6110 DNA fingerprinting helped us to find epidemiological links between some TB cases and that this technique estimate better the magnitude of recent transmission of the disease in the Province. However, a longer period of study should be performed to confirm some of the risk factors that are different from many forementioned studies. ACKNOWLEDGMENTS To Davood Habibzadeh from Research Center for tuberculosis of Tabriz for assistance in obtaining patient information and Mehrnoosh Doroudchi from Immunology Department of Shiraz University of Medical Sciences for providing M. tuberculosis 14323. REFERENCES
Copyright 2006 Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc06087f1.jpg] [oc06087t1.jpg] |
| |||||||||

{kind=link}
{kind=link}