 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memórias do Instituto Oswaldo Cruz, Vol. 101, No. 5, August, 2006, pp. 535-542 Evaluation of rapid alternative methods for drug susceptibility testing in clinical isolates of Mycobacterium tuberculosis Luciano Mengatto, Yosena Chiani, María Susana Imaz/+ Instituto Nacional
de Enfermedades Respiratorias "E. Coni", Blas Parera 8260, Santa
Fe (3000) Argentina Received 29 January
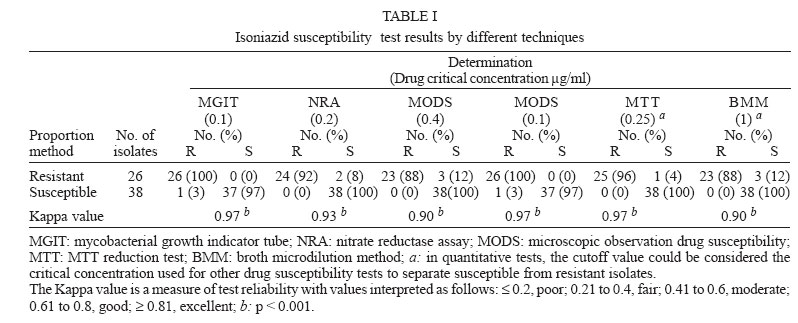
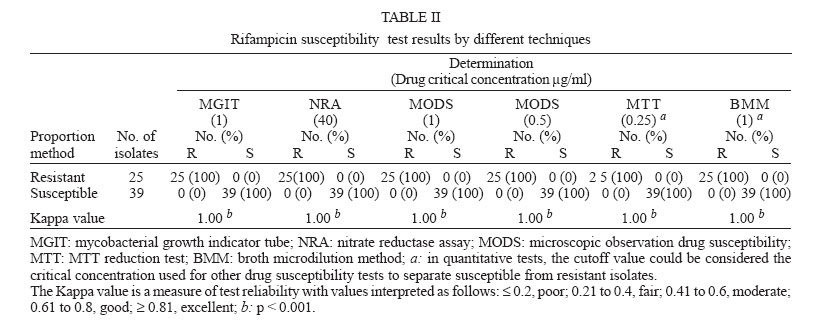
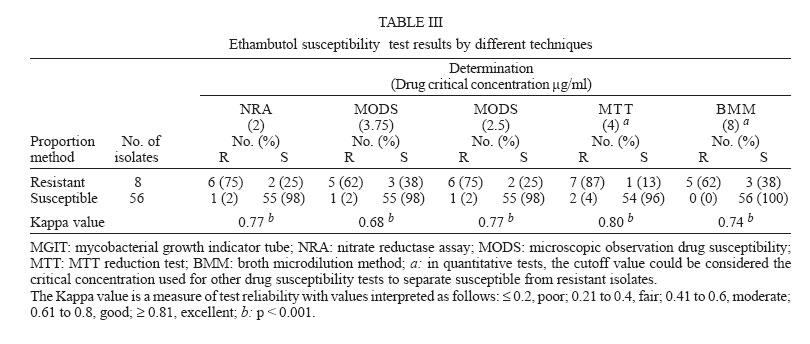
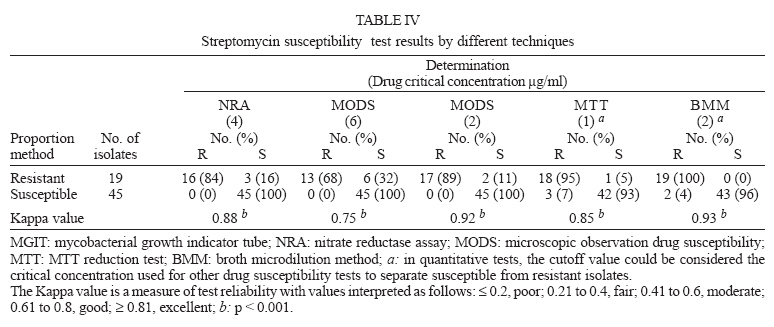
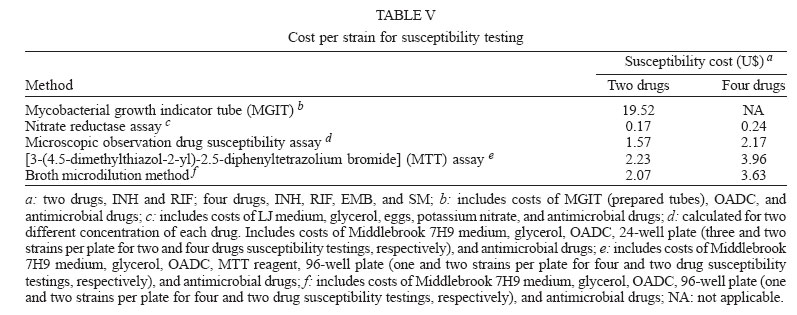
2006 Code Number: oc06090 A study was carried out to compare the performance of a commercial method (MGIT) and four inexpensive drug susceptibility methods: nitrate reductase assay (NRA), microscopic observation drug susceptibility (MODS) assay, MTT test, and broth microdilution method (BMM). A total of 64 clinical isolates of Mycobacterium tuberculosis were studied. The Lowenstein-Jensen proportion method (PM) was used as gold standard. MGIT, NRA, MODS, and MTT results were available on an average of less than 10 days, whereas BMM results could be reported in about 20 days. Most of the evaluated tests showed excellent performance for isoniazid and rifampicin, with sensitivity and specificity values > 90%. With most of the assays, sensitivity for ethambutol was low (62-87%) whereas for streptomycin, sensitivity values ranged from 84 to 100%; NRA-discrepancies were associated with cultures with a low proportion of EMB-resistant organisms while most discrepancies with quantitative tests (MMT and BMM) were seen with isolates whose minimal inhibitory concentrations fell close the cutoff. MGIT is reliable but still expensive. NRA is the most inexpensive and easiest method to perform without changing the organization of the routine PM laboratory performance. While MODS, MTT, and BMM, have the disadvantage from the point of view of biosafety, they offer the possibility of detecting partial resistant strains. This study shows a very good level of agreement of the four low-cost methods compared to the PM for rapid detection of isoniazid, rifampicin and streptomycin resistance (Kappa values > 0.8); more standardization is needed for ethambutol. Key words: drug-susceptibility testing - Mycobacterium tuberculosis - rapid methods The emergence of tuberculosis in conjunction with the increasing number of multi-drug resistant strains of Mycobacterium tuberculosis has increased the need for rapid and reliable methods of diagnosis and drug susceptibility testing (DST). The Lowenstein-Jensen (LJ) or agar proportion method (PM) (Canetti et al. 1963, 1969, Kent & Kubica 1985) and the radiometric method in BACTEC TB-460 system (Becton-Dickinson) (Roberts et al. 1983) are the current standard methods recommended to perform susceptibility testing of M. tuberculosis. However they are either time consuming or require the use of radioisotopes, that should be disposed of. Recently, new commercial methods were developed, including mycobacterial growth Indicator Tube (MGIT) (Rusch-Gerdes et al. 1999) and molecular tests such as INNOLIPA Rif TB (Innogetics, Ghent, Belgium) (Rossau et al. 1997). However they are rapid, but expensive, making them impractical for use in developing countries. A number of new simple and inexpensive methods for drug susceptibility testing have been recently described. The microscopic observation drug susceptibility (MODS) assay is a liquid culture method based on microscopic detection of characteristic M. tuberculosis morphology (Caviedes et al. 2000). The broth microdilution method (BMM) has shown to be a practical and rapid method to determine minimum inhibitory concentrations (MICs) of antituberculosis drugs (Leite el al. 2000, Coban et al. 2004). To improve the mycobacterial growing reading, an association of this method with colorimetric compounds, like the oxidation-reductor indicator MTT [3-(4.5-dimethylthiazol-2-yl)-2.5-diphenyltetrazolium bromide] has been successfully used (Caviedes et al. 2002). Another new method recently developed is the nitrate reductase assay (NRA) based on the ability of M. tuberculosis to reduce nitrate to nitrite; the reduction can be detected by using specific reagents which produce color change (Angeby et al. 2002). In the present study 64 clinical isolates of M. tuberculosis were tested by a commercial method (MGIT) and four inexpensive methods for DST: the MODS assay, the BMM, the MTT reduction test, and the NRA. The ensuing overall comparison provides a convenient frame of reference for the reliability of these rapid DST methods in the routine of the micobacteriology laboratories. MATERIALS AND METHODS Strains and inoculum preparation - A total of 64 clinical isolates and H37Rv ATCC 27294 (sensitive to all the antituberculosis agents) were evaluated in this study. The M. tuberculosis strains were obtained from 64 different patients whose isolates were referred to the Laboratory of the National Institute of Respiratory Diseases "E. Coni" (Santa Fe, Argentine) for drug susceptibility testing between 2003 and 2005. All clinical isolates were grown in LJ medium and tested in a blind manner for all different methods. The strains were defined as M. tuberculosis according to growth rates, pigmentation, colony properties, and routine biochemical methods (catalase, nitrate reduction, and niacin accumulation tests) (Centro Panamericano de Zoonosis 1988). Colonies from LJ were transferred to a tube containing 6-9 sterile glass beads and 3-4 ml of 7H9-S broth [Middlebrook 7H9 broth base (Difco, Sparks, MD, US; 4.7 g/l), with 0.2% glycerol, supplemented with 10% oleic-albumin-dextrose-catalase (OADC; Becton Di-ckinson, Sparks, MD, US)]. Tubes were vigorously agitated and clumps were allowed to settle 30 min. The supernatants were then adjusted with distilled water to equal the density of a 0.5 McFarland standard to be used in the BMM, MGIT, and MODS assays and to equal the density of a 1 McFarland standard to be used in the NRA, PM, and MTT assays. The reference H37Rv was tested each time the experiences were performed with clinical isolates. Antituberculous drugs - Rifampicin (RIF), isoniazid (INH), ethambutol (EMB), and streptomycin (SM) were obtained in powder form from Sigma Chemical Co (St Louis, MO, US). Stock solutions of INH, EMB, and SM were prepared in deionized water at 10 g/l and RIF was prepared in dimethylsulfoxide at 20 g/l. Stock solutions were kept at -20ºC for no more than one month. PM - The PM was performed on LJ medium according to Canetti et al. (1963) with the recommended critical concentrations of 0.2 µg/ml for INH, 40 µg/ml for RIF, 2 µg/ml for EMB, and 4 µg/ml for SM. To define drug-susceptible from drug-resistant organisms, the PM was considered the gold standard. MODS assay - This assay was performed in sterile 24-well plates (Falcon, Becton Dickinson, Franklin Lakes, NJ, US). To prepare the inoculum, the bacterial suspension, adjusted to a turbidity equivalent to that of a 0.5 McFarland standard, was diluted to 10-3 in 7H9-S broth. Antibiotic working solutions were prepared at the following concentrations: INH, 1 and 4 µg/ml; RIF, 5 and 10 µg/ml; EMB, 25 and 37.5 µg/ml; SM, 20 and 60 µg/ml. Five hundred and forty microliters aliquots of diluted bacterial samples were distributed in wells of a 24-well plate. For each isolate, a 60 µl aliquot of each one of the drug working solutions was added. Sixty microliters of 7H9-S broth was added in a drug-free control well containing the diluted bacterial suspension. Each plate contained an additional well of drug-free medium; no bacteria were inoculated into this well, which served as a control for cross contamination. Plates were covered and sealed with plastic bags and incubated at 37ºC in normal atmosphere. Starting on day 3, every 1 or 2 days, wells were examined for the presence of mycobacteria under an inverted light microscope (x40 magnification). For the purposes of this study, growth was defined as the emergence of visually detectable serpentine clusters of bacteria. If there was growth in the control well then drug-containing wells were visualized on the same day; growth in the presence of drug was regarded as resistant whereas no growth in the presence of drug was considered as susceptible. The final drug concentrations were: INH, 0.1 and 0.4 µg/ml; RIF, 0.5 and 1 µg/ml; EMB, 2.5 and 3.75 µg/ml; SM, 2 and 6 µg/ml (Caviedes et al. 2000, Moore et al. 2004). MGIT - MGIT susceptibility testing was performed according to the manufacturer's recommendations. For each isolate tested, three tubes were prepared: two contained the antituberculosis drugs, and one was a drug-free growth control. To all tubes, 0.5 ml of MGIT OADC growth supplement (Becton Dickinson, Sparks, MD, US) was added, and 0.1 ml of the antibiotic solution was also added to each one of the drug-containing tubes, giving a final concentration of 0.1 µg INH per ml and 1 µg RIF per ml. All three tubes were then inoculated with 0.5 ml of a 1:5 dilution (in distilled water) of a standard inoculum, tightly capped, and incubated at 37ºC. A positive MGIT control tube was prepared by adding 5 ml of a 0.4% sodium sulphite solution to an empty MGIT tube. An uninoculated MGIT tube, showing minimal or no fluorescence, served as negative control. Starting on day 3, tubes were daily examined for fluorescence by placing them on a 365 hm UV transiluminator. An isolate was considered as susceptible whenever the tube containing the drug did not fluoresce within two days after the growth control tube fluoresced, and as resistant whenever the tube with the drug was positive within 2 days of the positivity of the growth control. NRA - The NRA was performed as described by Angeby et al. (2002). Briefly, the antibiotic was included in LJ medium at a concentration of: 0.2 µg/ml for INH, 40 µg/ml for RIF, 2 µg/ml for EMB, and 4 µg/ml for SM; 1000 mg/l of potassium nitrate (KNO3) was also added. Part of the inoculum, adjusted to equal the density of a 1 McFarland standard, was diluted 1:10 in distilled water. For each isolate, 0.2 ml of the undiluted inoculum was added into the tubes containing LJ medium with KNO3 and the antituberculosis drugs; and 0.2 ml of the 1:10 dilution was inoculated into drug-free media containing KNO3 (tubes in triplicate), serving the last three ones as control growth. Tubes were incubated at 37ºC for 14 days and 0.5 ml of a mixture of three reagents (1 part 50% concentrated hydrochloric acid, 2 parts 0.2% sulfanilamide and 2 parts 0.1% N-1-naphthylenthylenediamine dihydrochloride) was added to one drug-free control tube after 7 days of incubation. If its colour changed to pink then tubes with drugs were tested on the same day. An isolate was considered resistant if there was a colour change in the drug-tube greater than in the 1:10 diluted growth control. If the drug-free control tube did not show any colour change and remained the same, the remaining tubes were further incubated, and the procedure repeated on days 10 and 14 respectively. MTT assay - The MTT assay was done as described by Caviedes et al. (2002). Briefly, to prepare the inoculum, the bacterial suspension adjusted to equal the density of a 1 McFarland standard was diluted 1:25 with 7H9-S broth and 100 µl was used as an inoculum. Two hundred microliters volume of sterile water was added to all outer wells of sterile 96-well plates (Cellstar, Griener Bio-one, Frickenhausen, Germany). One hundred microliters volume of 7H9-S broth was added in each well and serial two-fold dilutions of each drug were prepared directly on the plate by adding 100 µl of the drug working solutions (prepared at four-fold the highest concentration tested on the plates). The final drug concentration ranges were as follows: 0.125 to 32 µg/ml for INH, 0.062 to 16 µg/ml for RIF, 0.5 to 128 µg/ml for EMB and 0.125 to 32 µg/ml for SM. One hundred microliters of the inoculum was added to the wells. Six growth controls containing no antibiotic were included for each isolate. The plates were sealed, placed in plastic bags and incubated at 37ºC at normal atmosphere. On day-5, 50 µl of the tetrazolium-Tween 80 mixture {1.5 ml of tetrazolium[3-(4,5-dimethylthiazol-2-yl)-2,5diphenyl-tetrazolium bromide] [ICN Biomedicals, Aurora, Oh, US] at a dilution of 1 mg/ml in absolute ethanol and 1.5ml of 10% Tween 80} was added to one growth control and the plate was then incubated at 37ºC for 24 h. If this well turned purple, the tetrazolium-Tween 80 mixture was added to all wells and the colour was recorded at 24 h. Otherwise, if the growth control well remained yellow the plate was then incubated at 37ºC for 24 h, after which tetrazolium-Tween 80 mixture was added to another control before the plate was incubated for another 24 h. If this well remained yellow, incubation was continued and tetrazolium-Tween 80 solution was added to each of the remaining four controls on days 9, 11, 13, and 15. The minimal inhibitory concentration (MIC) was defined as the lowest concentration of each drug that prevented the colour change and the strains were considered susceptible to each drug, if their MICs were below or equal to the critical concentration reported by Montoro et al. (2005); INH, 0.25 µg/ml; RIF, 0.25 µg/ml; EMB, 4 µg/ml; SM, 1 µg/ml. BMM assay - This assay was performed in sterile 96-well plates (Cellstar) as described by Leite el al. (2000) with minor modifications. Briefly, to prepare the inoculum, the bacterial suspension adjusted to equal the density of a 0.5 McFarland standard was diluted 1:25 with 7H9-S broth and 100 µl was used as an inoculum. One hundred microliters volume of 7H9-S broth was added in each well and serial two-fold dilutions of each drug were prepared directly on the plate by adding 100 µl of the drug working solutions (prepared at four-fold the highest concentration tested on the plates). The final drug concentrations obtained were the same as described before for MTT. One hundred microliters of the inoculum was added to the wells. A well without antimycobacterial agent was also inoculated with 10-2 dilution of the inoculum as growth control. The plates were sealed, placed in plastic bags and incubated at 37ºC for 28 days in normal atmosphere. MIC was defined as the lowest drug concentration that exhibited no growth by visual reading, and the strains were considered susceptible to each drug, if their MICs were below or equal to the critical concentration reported by Wallace et al. (1986); INH, 1 µg/ml; RIF, 1 µg/ml; EMB, 8 µg/ml; SM, 2 µg/ml. Costs - All costs were calculated using recent purchase records. Costs for labor were not included. Data analysis - The performances of the MGIT, MODS, BMM, MTT, and NRA methods in comparison with the PM were evaluated in terms of sensitivity (ability to detect true resistance) and specificity (ability to detect true susceptibility). The agreement between the above mentioned assays and the PM was estimated by the Kappa statistic. The kappa value, a measure of a test reliability, was interpreted as follows: < 0.2, poor; 0.21 to 0.4, fair; 0.41 to 0.6, moderate; 0.61 to 0.8, good; > 0.81, excellent (Altman 1999). RESULTS Patterns of susceptibility to INH, RIF, EMB, and SM for 64 M. tuberculosis isolates were determined by PM. Out of 64 cultures, 26 (40%) were resistant to INH, 25 (39%) to RIF, 19 (30%) to SM, and 8 (13%) to EMB. Twenty nine cultures were fully drug-susceptible, 7 were monoresistant, 16 were resistant to two drugs and 9 to three drugs. Susceptibility testing results Isoniazid - The PM results with INH were compared with those obtained by the MGIT, NRA, MODS0.4µg/ml, MODS0.1µg/ml, MTT, and BMM methods (Table I). As regards susceptible cultures, only MGIT and MODS0.1µg/ml assays, which use a lower INH critical concentration (0.1 µg/ml) than that employs by the reference PM (0.2 µg/ml), misidentified as resistant one of the 38 susceptible cultures (the same isolate in both methods). Out of 26 INH resistant cultures, three (12%) were susceptible with MODS0.4µg/ml assay; of these three isolates, the MICs by MTT for two isolates were 0.5 µg/ml (one dilution (twofold) higher than the MTT-cutoff value) and the MIC for one isolate was 0.25 µg/ml (at the MTT-cutoff value). Thus, when 0.1 µg/ml was used as critical concentration in MODS method, the agreement was 100%. The NRA, MTT, and BMM assays failed to detect 2, 1, and 3 resistant strains, respectively, whereas MGIT gave 100% agreement; these discordant results were found in only 3 isolates (the same as in the MODS0.4µg/ml); although the BMM showed the poorest sensitivity, the MICs of the three discordant strains were only at or one (twofold) dilution lower than the cutoff value. Sensitivity values for MGIT, NR, MODS0.4µg/ml, MODS0.1µg/ml, MTT, and BM methods were 100, 92, 88, 100, 96, and 88%, respectively, and specificity values were 97, 100, 100, 97, 100, and 100%, respectively. Rifampicin - Complete agreement was found between the results found with the MGIT, NRA, MODS1µg/ml, MODS0.5µg/ml, MTT, and BMM methods compared with those obtained with the PM (Table II). Ethambutol - The PM results with EMB were compared with those obtained by the NRA, MODS3.75µg/ml, MODS2.5µg/ml, MTT, and BMM methods (Table III). Specificity values were high in all methods (98, 98, 98, 96, and 100% by NR, MODS3.75µg/ml, MODS2.5µg/ml, MTT, and BM methods, respectively). However, low sensitivities were obtained with most of the tests, with values of 75, 62, 75, 87, and 62% by the NRA, MODS3.75µg/ml, MODS2.5µg/ml, MTT, and BMM methods, respectively. The two discordant results designated resistant by the PM and susceptible by the NRA were found in cultures with only a very small proportion of their bacterial population (between 1 to 10%) that was detected to be EMB-resistant by the PM (cultures designated as borderline; Siddiqi et al. 1985). The MICs of most of the discordant results (2 of the 3 isolates) designated resistant by the PM and susceptible by BMM were found to be at the cutoff value. The same cultures were associated with the discordant results obtained with MTT and MODS assays. Streptomycin - The PM results with SM were compared with those obtained by the NRA, MODS6µg/ml, MODS2µg/ml, MTT, and BMM methods (Table IV). As regards susceptible isolates, only MTT and BMM methods misidentified as resistant three and two cultures, respectively. None of the isolates classified as susceptible by the PM were highly resistant by MTT and BMM methods; their corresponding MICs by MTT and BMM methods were only one (twofold) dilution higher than the cutoff value of each method. Out of the 19 SM-resistant cultures, six (32%) were misidentified as susceptible by MODS6µg/ml. Of these six isolates with discordant results, the MICs by MTT for one isolate was 0.5 µg/ml (one dilution lower than the MTT-cutoff value), for two isolates were 2 µg/ml (one dilution off the MTT-cutoff value), for two isolates were 4 mg/ml and for the remaining isolate was 8 µg/ml. Furthermore, when 2 µg/ml was used in MODS method, the percentage of discordant results decreased to 10% (2 from 19). For NRA, 3 of the 19 resistant isolates were found susceptible, giving a low level of sensitivity (84%). Overall, sensitivity values for the NRA, MODS6µg/ml, MODS2µg/ml, MTT, and BMM methods were 84, 68, 89, 95, and 100%, respectively, whereas the specificity values were 100, 100, 100, 93, and 96%, respectively. Costs - Table V shows the estimated costs per strain for susceptibility testing. Costs were calculated for two first-line anti-TB drugs (INH and RIF), and for four first-line drugs (INH, RIF, EMB, SM). Items included in cost analysis are noted below the Table. Turnaround time (TAT) - The average time required to obtain a susceptibility result by the MGIT, NRA, MODS, and MTT methods was 6.4 days (range, 3 to 13), 9 days (range, 7 to 14), 7 days (range, 4 to 14) and 7.7 days (range, 7 to 17), respectively. As regards BMM, MICs could be read when organisms had reached good macroscopic growth in control wells, generally after 14-17 days, but the reading was repeated every two days up to day 28 of incubation. More than half of the strains had no change in the MIC value from day 14 to 20 of incubation; almost 75% of changes involving only one dilution. None of the strains had change in MICs after day 20 of incubation. Furthermore, considering some authorsx concerns on the fact that early readings might result in false susceptibility if a heterogeneous population of resistance was present, we chose to use the 20-day reading time (Wallace et al. 1986). DISCUSSION Recently, new methods for rapid determination of M. tuberculosis DST have been described, viz MGIT, NRA, MODS, MTT, and BMM assays. In practice, these methods vary greatly, especially in the type of medium used and in the drug concentration in the medium. Each method has been successfully tested in previous studies (Rusch-Gerdes et al. 1999, Leite el al. 2000, Caviedes et al. 2000, 2002, Angeby et al. 2002, Park et al. 2002), showing that results can be obtained faster than with the PM, but, to the best of our knowledge, they have never been compared together. Our data demonstrated that the evaluated methods have an excellent test performance for INH and RIF (sensitivity and specificity values higher than 90% with most of the tests). Results with the other first line anti-tuberculosis drugs, SM and EMB, but especially with EMB, showed some discrepancies. Some of the important factors, which may have contributed to these discrepancies, are: (i) a low proportion of drug resistant organisms in the test population of a culture, (ii) substantial differences in the medium used by the methods, and (iii) different periods of incubation, which may be associated with different degrees of degradation of the antimicrobial agent. In quantitative tests like MTT and BMM methods, the cutoff value is considered the drug concentration that would separate susceptible from resistant isolates. In these tests, this value could be interpreted as the critical concentration used for other DST methods to distinguish susceptible from resistant strains (Heifets 2000). Nevertheless, care should be taken when interpreting MIC values close the critical concentration, since like in some other studies evaluating quantitative DST methods (Franzblau et al. 1998, Luna Herrera et al. 2003), in our work, most discrepancies among the PM and MTT or BMM were seen with isolates whose MICs fell at or one dilution (twofold) higher or lower than the cutoff value. Based on these observations, some authors (Heifets et al. 1990, Franzblau et al. 1998, Luna-Herrera et al. 2003) have suggested the use of a partially resistant range that is close to the cutoff value, proposing the existence of three categories of susceptibility: susceptible, partially resistant (isolates with borderline MICs) and resistant. The use of these categories would allow the identification of TB due to low-level resistant strains, making possible the use of a drug up to near the maximum concentration that it could reach in the human body. In this respect, some evidences indicate that the use of high-dose isoniazid in TB retreatment regimens, in spite of the acquired isoniazid resistance, could improve therapeutic results, if all or part of the organisms were resistant to only a low concentration of that drug (Moulding 1981). Similarly, the use of double drug critical concentration with MODS test allowed the identification of 11% (3 of 26) INH-resistant strains and 21% (4 of 19) SM-resistant strains, that grew in low but not in high concentration of drugs; their corresponding MICs determined by MTT fell into the INH and SM partially resistant ranges proposed by Franzblaw et al. (1998) (between 0.25 and 0.5 µg/ml for INH and between 2 and 8 µg/ml for SM). Therefore, and taking into account these authors' notion of three categories of susceptibility, these strains could be considered low-level resistant strains. Twenty five percent (2 out of 8) EMB-resistant strains were misidentified as susceptible by NRA. Interestingly, among the eight true EMB-resistant strains, these two cultures were the only ones with a very small from 1 to 10% - proportion of the bacterial population showing to be resistant by the PM (cultures designated as borderline; Siddiqi et al. 1985). The NRA was standardized to consider a strain "resistant" when the drug-containing tube inoculated with an undiluted suspension of bacilli exhibited a nitrate reductase (NR) activity greater than that appearing in the 1:10 diluted growth control (where about 10% of the original inoculum was added). In "borderline" strains, it would be expected that only about less than 10% of the organisms could grow in the EMB-containing tube, so that it is probable that the NR activity exhibited by the drug-containing tube was lower than that obtained in the 1:10 diluted growth control tube. Furthermore, some authors have shown that these "borderline" cultures, more frequently associated with EMB resistance, have classically caused problems in the interpretation of EMB DST (Siddiqi et al. 1985), adversely affecting the assays overall performance. On the other hand, for SM, a low level of sensitivity was obtained. Similar results were reported by Martin et al. (2005) in their multicenter evaluation of the NRA. A possible interaction between the drugs and the potassium nitrate was speculated as a cause of this discrepancy. The turnaround time (TAT) is important in order for the patient to receive an appropriate treatment. The results obtained with MGIT, MODS, NRA, and MTT were available on an average of less than 10 days as with the reference method BACTEC-460. The BMM, although consuming more time than the other four evaluated tests, could be still reported faster (about 20 days) than the PM (28-40 days). Caviedes et al. (2000), in their evaluation of MODS assay for DST, defined a "resistant strain" whenever the growth in the presence of drug is microscopically observed on the same day when the growth in control wells is detected; suggesting that the wells have to be microscopically examined every one or two days. This high frequency of checking obviously yielded the fastest results, and at first, one could anticipate that it would prevent that true susceptible strains could be misidentified as resistant, if the time between the appearance of "any growth in the drug-containing wells" of susceptible cultures and "that in the control wells" were too short. In our study, we tested that this period was about 10 days minimum (during the 28-day incubation period, about 90% of susceptible strains showed no growth in the drug-containing wells), allowing, if necessary, to perform the microscopic observation at intervals suitable to the laboratory workload, thus adding an operational advantage to this method. RIF resistance is considered to be a strong predictor of the presence of multidrug-resistant tuberculosis, especially in countries with high prevalence of drug resistance (Rossau et al. 1997). Therefore, the complete agreement in RIF-susceptibility results found for all the methods studied in this work indicates the potential of any of this simple and inexpensive assays for control programs in countries with high levels of tuberculosis endemicity. In accordance with previous studies, this work showed that MGIT system is a reliable, rapid and convenient method for performing INH and RIF susceptibility tests, but too expensive to implement in low-resources countries. Indeed, cost was the factor that prohibited us its evaluation with EMB and SM. This study showed that using low-costs "in house" assays for rapid detection of susceptibility, good or excellent levels of agreement with the PM were obtained. The NRA seems to be the most inexpensive method; the medium used is the classical LJ with the same concentration of antimicrobial drugs that is used for the PM; it is easy to perform without changing the organization of the routine laboratory performing DST. However NRA gives only qualitative results. On the other hand, both microdilution susceptibility tests (MTT and BMM) and MODS assay offer the advantage of identifying partial resistance but have the disadvantage from the point of view of biosafety because manipulation of plates could generate aerosols. Placement of the plate in a transparent plastic bag, appropriately secured, adds an element of biosafety. In this regard, results obtained by MODS and BMM, which are methods based on the direct microscopic or macroscopic growth observation, do not require the addition of any reagent (like in MTT), thus the sealed plates should not be opened and, consequently, the biohazard potential might be reduced in the case that the plate is mishandled. REFERENCES
Copyright 2006 Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc06090t1.jpg] [oc06090t3.jpg] [oc06090t2.jpg] [oc06090t5.jpg] [oc06090f1.jpg] [oc06090f4.jpg] [oc06090t4.jpg] [oc06090f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}