 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memórias do Instituto Oswaldo Cruz, Vol. 101, No. 5, August, 2006, pp. 551-553 Protection against hepatitis B by the Butang® recombinant vaccine in newborn children in South Brazil Aline Paula Isolani, Catia Silene Sversuti, Ana Maria Sell, Ricardo Alberto Moliterno+ Departamento de
Análises Clínicas, Universidade Estadual de Maringá,
Av. Colombo 5790, 87020-900 Maringá, PR Brasil Received 9 February
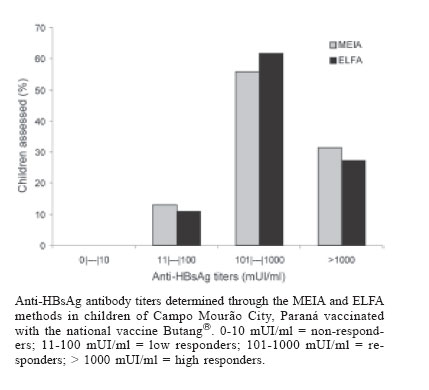
2006 Code Number: oc06093 The prevention of hepatitis B by vaccination is one of the most efficient tools to avoid the transmission of the virus. This study evaluated the immunogenicity of the national vaccine Butang® in children born in Campo Mourão City, state of Paraná, Brazil, aged 7 to 12 months, by determining the anti-HBsAg antibodies levels after completion of the National Immunization Program Protocol for hepatitis B. All 70 children evaluated by the MEIA method (immune-enzymatic micro particles) showed seroconversion to the Butang® vaccine. Nine children (12.9%) presented a low response, with anti-HBs titers between 11 and 100 mUI/ml; 39 children (55.7%) showed a good response to the vaccine, with titers between 101 and 1000 mUI/ml; and 22 children (31.4%) showed antibodies titers higher than 1000 mUI/ml. The mean titer of the anti-HBs antibody titers was 1408.1 ± 2870.26 mUI/ml (15.7 to 19560.0 mUI/ml). The levels of antibodies produced by the prematurely-born children were not statistically different from those found in the newborns. Fifty-five children were also evaluated through the ELFA method (ELISA with a final detection in fluorescence), which presented similar results. The results obtained in our study corroborated the effectiveness of the national vaccine Butang® in newborn children of Campo Mourão City, Paraná, even if they were premature. Key words: Butang® - hepatitis B - vaccine - anti-HBsAg The infection by the hepatitis B virus (HBV) appears under different forms of evolution, ranging from the asymptomatic and self-limited infection to the chronic state, which can develop into chronic hepatitis, cirrhosis and hepatic-cellular carcinoma (Moradpour & Wands, 1995). The World Health Organization (WHO 2005) esteems that about two billion people already had contact with the hepatitis B virus (HBV), and that 5% of the world population are chronic carrier of this virus; there are between 6 and 12 million in Latin America, 60% of them in South America. In Brazil, it is believed that 15% of the population has come into contact with HBV, according to a survey carried out by Ministry of Health (Ministério da Saúde 2003). The prevention of hepatitis B by vaccination is one of the most efficient tools to avoid the transmission of the virus. Two recombinant vaccines derived of yeasts were licensed in 1987. They contain the largest surface protein of the hepatitis B virus (protein S, HBsAg), and were produced by Merck Sharp Dohme and Smith Kline Beecham, respectively (Granovski 1997). The National Immunization Program (PNI) recommends that newborns, weighing more than two kilograms, receive a vaccination outline composed of three doses: one at birth, the second at one month, and the third at six months of age (0, 1, 6). In newborns with less than two kilograms or in those prematurely born, a four-doses-outline is recommended (0, 1, 2, 6). The vaccine shall be administered in the deep intramuscular, and the thigh's muscle is the choice muscle in children with less than two years of age. The Instituto Butantan developed and is producing the Butang® vaccine against hepatitis B through genetic engineering techniques, using the Hansenulla poly-morpha yeast. The advantage of this system when compared to any other, such as the Saccharomyces cerevisiae, is that its expression is 4 to 10 times larger, reducing the production costs (Hieu et al 2002). However, further studies are still necessary to prove the efficacy of the vaccination protocols in Brazilian children. Moreover, the knowledge of the degree of immunological responses produced by the vaccine (none, low, intermediate or high) allows us to determine if the vaccinated children are protected or not to the infection by the HBV, what can help in the development of new prevention strategies against hepatitis B in the susceptible groups. MATERIALS AND METHODS The study was carried out in 70 children (from 7 to 12 months-old) vaccinated against hepatitis B in Health Care Units in the city of Campo Mourão. These children received the 3 doses of 10 µg of the Butang® vaccine (0, 1 and 6 months), as established by the PNI. The median interval between vaccination and anti-HBsAg evaluation was 113 ± 56.2 days. We collected 5 ml of peripheral blood, whose serum was stored at -20ºC until carrying out the analyses. The participation in the study was voluntary. The children's parents or their responsible signed an authorization term, which was approved by the Research Ethics Committee of Maringá State University. An epidemiological inquiry was also accomplished with information about gender, age, weight at birth and gestational weeks. Children born before 37 gestational weeks were considered premature. We carried out the determination of anti-HBsAg antibody levels through the immuno-enzymatic microparticles method (MEIA) in sera of 70 children. Sera from 55 children were also tested by ELISA with a final detection in fluorescence (ELFA), in order to confirm the antibodies titers. The tests were performed in the IMx (Abbott reagents) and in the MiniVIDAS (BioMerieux reagents) equipments, following the manufacturers' instructions, both with 1000 mUI/ml as detection limit. MEIA sera titers equal to 1000 mUI/ml were retested after dilution to find the end-point titers. The vaccinated children were classified in four groups: 0-10 mMUI/ml = non-responders; 11-100 mUI/ml = low responders; 101-1000 mUI/ml = responders; > 1000 mUI/ml = high responders (West & Calandra 1996, Losonsky et al 1999). The geometric mean titer of the anti-HBS antibody titers (GMT) for the MEIA method was also determined. The statistical analysis was carried out using the SAS - Statistical Analysis System Program (SAS Institute Inc. 1986). We also carried out a frequency analysis of the epidemiological data. RESULTS The participants' average age was of 9.78 months (± 1.89). There were 40 male (57.1%) and 30 female (42.9%). The average weight among the newborn children (n = 60 was 3.31 (± 0.37) kg; the average weight among the prematurely born (n = 10) was 2.69 (± 0.69) kg. According to the mothers' report, there were no adverse reactions to the vaccine. All 70 children evaluated by the MEIA method showed seroconversion to the Butang® vaccine. Nine children (12.9%) presented a low response, with anti-HBs titers between 11 and 100 mUI/ml; 39 children (55.7%) showed a good response to the vaccine, with titers between 101 and 1000 mUI/ml; and 22 children (31.4%) showed antibodies titers higher than 1000 mUI/ml (Figure). The GMT was 1408.1 ± 2870.26 mUI/ml (15.7 to 19560.0 mUI/ml). The ELFA methodology also showed a 100% sero-conversion rate in the 55 children tested. Six children (10.9%) showed anti-HBs titers between 11 and 100 mUI/ml; 34 children (61.8%) had titers between 101 and 1000 mUI/ml; and 15 children (27.3%) presented antibodies titers higher than 1000 mUI/ml (Figure). We also observed that the levels of antibodies produced by the prematurely-born children were not statistically different from those found in the full term newborns (GMT = 680.3 ± 648.28 mUI/ml vs 1529.4 ± 3076.67 mUI/ml, respectively, p = 0.43). DISCUSSION The discovery of an effective vaccine in the prevention of the infection by the hepatitis B virus allowed an important reduction in both the morbidity and mortality rates attributed to this infection (Blumberg 1997). A study with the North American vaccine Recombivax® (5 µg/dose) in Brazilian children demonstrated a 100% sero-conversion rate in full term, and of 92.7% seroconversion in premature born babies (Sadeck & Ramos 2004). Another study with the North American vaccine Engerix-B® in Brazilian infants vaccinated in the first week of life showed 98.2% seroconversion in full term infants, and a 77.4% seroconversion in preterm infants weighting 1.8 kg or less, with GMTs of 537.5 mUI/ml and 186.6 mUI/ ml, respectively (Motta et al 2002). The GMTs of the full term and preterm infants vaccinated with Butang® in our study were higher, although none of the preterm infants weighted less than 1.9 kg. In pre-licensing studies, the national vaccine Butang® showed low reaction and good immunogenicity in adults. In these individuals, Butang® had titers ranging from 17.5 to 29.500 mUI/ml, and a seroconversion rate of 95.3% (Costa et al 1997). In another study, the seroconversion rates grouped by age group varied from 70 to 100%, while the GMTs ranged from 46.5 to 124 mUI/ml (Ioshimoto et al 1999). Similar results were found by Baldy et al (2004), in a comparative study between the Brazilian vaccine Butang® and the Korean vaccines Euvax® and Hepavax-gene®, which used 3 doses of 10 µg (half of the usual dose) in adolescents between 17 and 19 years. They obtained seroconversion rates of 96.2, 98.6 and 96.5%, and GMTs of 727.8, 2009.1 and 1729.8 mUI/ml, respectively. Another study comparing the vaccine Butang® with Engerix B® in Brazilian newborns demonstrated that, after 3 doses, the seroconversion rates were of 93.7% and 97.5%, respectively, with GMTs of 351.1 and 1530.6, respectively (Martins et al 2004). The results obtained in our study corroborated the effectiveness of the national vaccine in newborn children of Campo Mourão city, Paraná. All children who received the 3 doses of the Butang® vaccine produced anti-HBs levels above those considered protecting (10 mUI/ml), even if they were premature. Also, the GMTs of the preterm and full term infants in this study were equal to or higher than those described in the literature. We also observed that the MEIA and ELFA methods are equivalent in determining antibody titers against HBsAg. We concluded, therefore, that the national recombinant vaccine for hepatitis B, Butang®, produced by the Butantan Institute, presents a good performance in its clinical screening, supporting its administration in newborn children. REFERENCES
Copyright 2006 Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc06093f1.jpg] |
| |||||||||

{kind=link}