 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memórias do Instituto Oswaldo Cruz, Vol. 101, No. 5, August, 2006, pp. 559-563 Diagnosis of Streptococcus pneumoniae meningitis by polymerase chain reaction amplification of the gene for pneumolysin Juliana de A Matos/*, Danielle J Madureira, Maria C Rebelo**, Cristina B Hofer*, David E Barroso/+ Departamento de Bacteriologia, Instituto Oswaldo Cruz-Fiocruz, Av. Brasil 4365, 21040-900 Rio de Janeiro, RJ, Brasil *Serviço de Doenças Infecciosas e Parasitárias, Hospital Universitário Clementino Fraga Filho, Universidade Federal do Rio de Janeiro, Rio de Janeiro, RJ, Brasil **Instituto Estadual de Infectologia São Sebastião, Rio de Janeiro, RJ, Brasil +Corresponding author: barroso@ioc.fiocruz.br Received 20 February
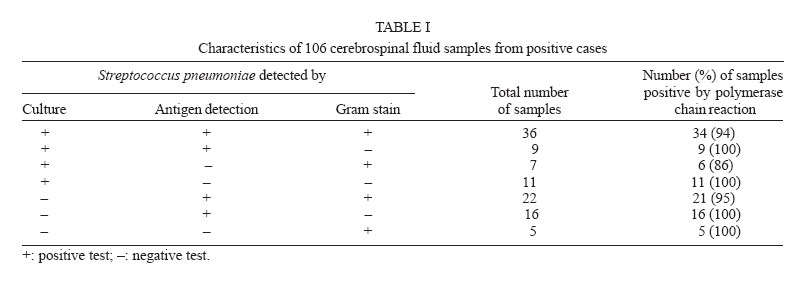
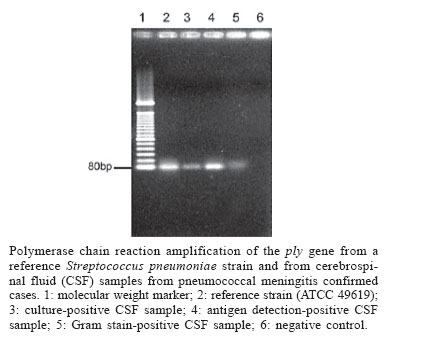
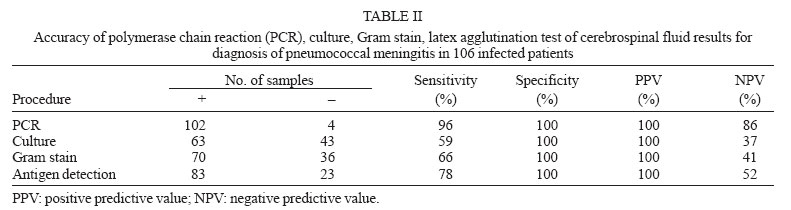
2006 Code Number: oc06095 Diagnosis of bacterial meningitis has long been based on classical methods of Gram stain, serological tests, and culture of cerebrospinal fluid (CSF). The performance of these methods, especially culture and direct smear, is thwarted by failure to detect bacteria following administration of antimicrobial agents and reluctance to performance lumbar punctures at admission. Indeed, patients with meningitis frequently receive antibiotics orally or by injection before the diagnosis is suspected or established. Thus an alternative method has become necessary to help clinicians and epidemiologists to management and control of bacterial meningitis. We evaluate the application of a polymerase chain reaction-based (PCR) assay for amplification of pneumolysin gene (ply) to diagnosis of Streptococcus pneumoniae meningitis. The PCR assay sensitivity for CSF was 96% (95% confidence interval, CI, 90-99%) compared to a sensitivity of 59% for culture (95% CI 49-69%), 66% for Gram stain (95% CI 56-74%), and 78% for latex agglutination test (95% CI 69-86%); PCR specificity was 100% (95% CI 83-100%). PCR results were available within 4 h of the start of the assay. This molecular approach proved to be reliable and useful to identify this bacterium compared with other classical laboratory methods for identification of bacterial meningitis pathogens. Key words: Streptococcus pneumoniae - meningitis - polymerase chain reaction - pneumolysin ply gene Community-acquired bacterial meningitis is one of the most dramatic medical emergencies, which is seen as a public health challenge world-wide. The disease is dreaded by parents and health care workers alike for its acute onset in previously healthy individuals and the difficulty in obtaining a timely and accurate diagnosis. Although the two main agents of acute bacterial meningitis in the community, Neisseria meningitidis and Streptococcus pneu-moniae, are responsive to antibiotic therapy, these diagnosis challenges of the disease pose a particular problem for treatment (Ragunathan et al. 2000, Heyderman et al. 2003, Makwana et al. 2004). S. pneumoniae meningitis is associated with a poor outcome due to a greater case-fatality rate and a higher probability of survivals develop permanent neurological sequelae when compared to other agents (Crook & Spratt 1998, Heyderman et al. 2003, Parent du Chatelet et al. 2005). An additional problem is an increase in the incidence of multiple antibiotic resistance in S. pneumoniae and recent emergence of strains with potential to cause epidemic of meningitis resembling N. meningitidis epidemics into the African meningitis belt (Crook & Spratt 1998, Leimkugel et al. 2005, Parent du Chatelet et al. 2005). The Haemophilus influenzae type b (Hib) conjugated vaccine was introduced in the public immunization program in 1999 by the State Health Department, which expanded vaccine coverage to all the population living in Rio de Janeiro, Southeast of Brazil. A dramatic reduction in Hib meningitis cases has been documented during the following years; consequently N. meningitidis and S. pneumoniae became the two major causes of bacterial meningitis beyond the neonatal period notified to local health authorities. Since the beginning of the XXI century, S. pneumoniae is the etiology of about 60 new confirmed cases of meningitis annually in the city of Rio de Janeiro, a rate of 1.2/100,000 population; 22 (37%) of these cases die and the number of survivals who develop permanent neurological sequelae is unknown (Rio de Janeiro City Health Department). Preadmission parenteral antibiotic has been widely recommended as a significant strategy to improve patient prognosis whenever the diagnosis of bacterial meningitis is suspected, particularly if lumbar puncture is not thought safe (Cartwright et al. 1992, Riordan & Cant 2002). The recommendation of early antibiotic therapy has been strongly advised to assistant physicians during the 1990s for suspected cases of meningococcal disease or acute bacterial meningitis (Heyderman et al. 2003, Makwana & Riordan 2004); thus a reduction in the proportion of confirmed cases by culture, direct smear or latex agglutination test was expected (Dalton & Allison 1968, Feldman 1978, Kanegaye et al. 2001, Nigrovic et al. 2004). The consequence has significant medical, epidemiological, and diagnostic implications. Since the mid of the 1990s local consultants in communicable diseases have reported an increase on the number of non-culture proven bacterial meningitis cases (Rio de Janeiro City Health Department). The increasing practice of preadmission administration of parenteral antibiotic therapy and reluctance to perform lumbar punctures at admission are pointed out to contribute to a decrease of confirmed cases in several countries, especially by the failure to isolate bacteria (Cartwright et al. 1992, Ragunathan et al. 2000, Corless et al. 2001, Kanegaye et al. 2001, Riordan & Cant 2002, Nigrovic et al. 2004). An alternative approach is nucleic acid amplification assays because antibiotics do not act as an inhibitor of the reaction (Cartwright et al. 1992, Borrow et al. 1997, Ragunathan et al. 2000, Rintamäki et al. 2002, Clarke & Edwards 2003). Target pneumolysin (ply) gene was investigated for identification of S. pneumoniae in clinical specimens from infected patients with otitis media, pneumonia or meningitis (Virolaine et al. 1994, Salo et al. 1995, Rintamäki et al. 2002, Corless et al. 2001, Clarke & Edwards 2003). Pneumolysin is a species-specific sulfhydryl-activated protein toxin produced intracellularly by all S. pneumoniae isolated from clinical samples, regardless the capsule antigen (serotype) (Walker et al. 1987). This pore-forming cytolysin discovered 100 years ago can be thought of as a key virulence factor following pneumococcal invasive infection (Libman 1905, Hirst et al. 2004). These features of pneumolysin turn the ply gene to be an attractive target for molecular diagnosis of S. pneumoniae invasive disease (Hirst et al. 2004, Messmer et al. 2004). The aim of this article is to assess the use and effectiveness of a polymerase chain reaction (PCR) assay to detect S. pneumoniae in cerebrospinal fluid (CSF) samples from meningitis patients collected and transported using the local field conditions, compared with other classical laboratory diagnostic methods for the identification of bacterial meningitis pathogens. MATERIALS AND METHODS Setting, study design, and case definition - This study took place at the Instituto Oswaldo Cruz, in the city of Rio de Janeiro, between 2004 and 2005. We conducted this study to evaluate the PCR assay to diagnosis S. pneu-moniae in CSF from patients with clinically diagnosed bacterial meningitis with etiologic source identified by a traditional laboratory method. In this study cases were defined by the presence of one of the following criteria: (i) isolation of S. pneumoniae from CSF; (ii) detection of pneumococcal capsule antigens in CSF by means of latex agglutination test; or (iii) identification of Gram-positive diplococci in a Gram stain CSF smear. Samples - All samples of CSF were processed for culture, cytological examination, biochemical reaction, latex agglutination test, Gram stain, and stored at 20°C in the Reference Laboratory of the State Meningitis Reference Centre, Instituto Estadual de Infectologia São Sebastião (IEISS), in the city of Rio de Janeiro, the Capital of the state of Rio de Janeiro. The reference laboratory obtains the samples, collected inside sterile glass vials, from patients admitted in the IEISS and it also receives them from other hospitals, mainly in the Rio de Janeiro metropolitan area. Sample delivery to the reference laboratory seldom is in adequate conditions at 4°C (on wet ice or chilly pad) from other hospitals. Frequently CSF samples come at room temperature (Th) in the first 24 h or even 1-2 days after lumbar puncture is done. So the PCR assay has to prove to work satisfactorily without ideal conditions of storage and transport before it reaches the reference laboratory. We have received 106 CSF samples from S. pneumoniae confirmed meningitis patients by one of the criteria for case definition presented above. The characteristics of these CSF samples studied are shown in Table I. CSF samples from patients with clinically diagnosed bacterial meningitis caused by other bacteria, identified as S. agalactiae (n = 6), M. tuberculosis (n = 4), L. mono-cytogenes (n = 2), S. aureus (n = 1), A. baumanii (n = 2), H. influenzae type b (n = 1), and N. meningitidis serogroups B, C, W135 or Y (n = 4) were used as controls. The bacterial DNA from the CSF sample was isolated with the use of DNeasy Tissue Kit (QIAGEN) according to the manufacturer's protocol for DNA purification from Gram-positive bacteria. PCR assay - To identify S. pneumoniae was performed a PCR amplification of the ply gene with specific oligonucleotide primers (Forward: TGCAGAGCGTCC TTTGGTCTAT; Reverse: CTCTTACTCGTGGTTT CCAACTTGA) designed by Corless et al. (2001) based on previously published gene sequences (Walker et al. 1987), for which the amplicon size was 80 bp. PCR reaction mixture (50 µl) contained 0.6 µM of each oligonucleotide primer (Invitrogen), 200 µM dNTPs, 1X PCR buffer, 3 mM MgCl2, 1U Platinun Taq DNA polymerase (Invitrogen), and 10 µl of DNA target. The PCR assays were performed in a DNA thermal cycler (GeneAmp PCR System 9700, PE Applied Biosystems) with the following conditions: 94°C for 3 min, 55°C for 30 s, 72°C for 20 s (initial cycle); followed by subsequent 35 cycles of 92°C for 40 s; 55°C for 30 s, 72°C for 20 s (denaturation, annealing, and polymerization, respectively); and 72°C for 10 min (final cycle of polymerization). Amplicons were analyzed by electrophoresis on a standard 2% agarose gel under UV fluorescence following staining with ethidium bromide. It was included in each assay the DNA from S. pneumoniae (ATCC 49619) as positive control and the reaction mixture without DNA target as negative control. Accuracy of test result - Sensitivity, specificity, positive predictive value, and negative predictive value were calculated using a two-way table (Epi InfoTM, Version 3.3.2, CDC). The chi-square with Yates correction was used to analysis the differences between proportions. Exact binomial 95% confidence intervals (CI) were estimated. The sensitivity of the PCR was determined using CSF from positive cases (culture or antigen detection or direct smear) corresponded to criteria i (n = 63), ii (n = 83), and iii (n = 70). To determine the specificity, amplification reactions were carried out using genomic DNA extracted (DNeasy Tissue Kit, Quiagen) from N. meningitidis (ATCC 13090), H. influenzae (ATCC 49766), H. influenzaae type b (ATCC 10211), S. aureus (ATCC 29213), S. agalactiae (clinical isolate), and E. faecalis (clinical isolate). It was also examined CSF samples from patients corresponded to bacterial meningitis other than pneumococcal (n = 20). RESULTS Of the 106 patients with pneumococcal meningitis, 25% were infants (mean of 5 months) and 16% were over 50 years. The median age was 30 years (range, 1 month to 75 years). Sixty-one (58%) patients were female and 45 (42%) were male (χ2 = 4.8, P = 0.03). The mean of CSF white blood cell count was 3756/mm3 (range, 1 to 48,800/mm3); 23% had less than 100/mm3 and 9% less than 15/mm3. Of the total, 102 samples from positive cases were correctly identified by means of PCR, whereas antigen detection was positive in 83, direct smear revealed organisms in 70, and only 63 isolates cultured from CSF. The amplicon of ply gene amplified from positive control (ATCC 49619) and three CSF samples from each positive case assigned only to one of the valid criteria in this study (culture, antigen detection, and direct smear) are shown in Fig. 1. PCR failed to amplify the ply target in three culture proven-cases and one non-culture proven-case solely based on antigen detection and Gram stain. There was no false-positive result. All CSF samples from bacterial meningitis other than pneumococcal were negative by PCR for the presence of S. pneumoniae DNA. The specificity of the assay was tested with DNA purified from four standard strains and two clinical isolates. No products were amplified from these genomics DNA but amplification of gene target was successful with DNA from S. pneumoniae standard strain. The sensitivity of the nucleic acid based amplification assay was evaluated with data from positive cases (culture or antigen detection or Gram stain). Sensitivity (96, 95 CI 90-99%), specificity (100, 95 CI 83-100%), positive predictive value (100, 95 CI 96-100%), and negative predictive value (86, 95 CI 67-96%) were calculated and compared with results obtained with classical laboratory diagnostic methods (Table II). DISCUSSION Diagnosis of bacterial meningitis is formerly founded on a suggestive clinical scenario, although it is the CSF white blood cell count that establishes the definitive diagnosis. The identification of bacterial meningitis etiologies is based on traditional laboratory diagnostic methods of culture, Gram stain, and serological tests (Ragu-nathan et al. 2000). All these diagnosis steps are hindered by the alteration of CSF findings, the failure to isolate bacteria, and a reduced identification of the organism on Gram stain CSF smear following administration of antibiotics (Dalton & Allison 1968, Ragunathan et al. 2000, Kanegaye et al. 2001, Riordan & Cant 2002, Nigrovic et al. 2004). Truly, a small but perplexing group of patients with bacterial meningitis in whom preliminary antibiotic therapy alters the CSF findings to the degree that is difficult to distinguish acute bacterial meningitis from viral aseptic meningitis or encephalitis, enhancing the possibility of diagnostic error. The reduction in bacterial concentration following preliminary antibiotic treatment for S. pneu-moniae decreases the diagnostic effectiveness of the Gram stain and CSF culture (Feldman 1978, Ragunathan et al. 2000, Kanegaye et al. 2001). The results expected by means of latex agglutination test do not alter after the parenteral administration of antibiotics, but in some instance a decrease in the sensitivity of this test can be explained by the time relationship between onset of the specific treatment and when the lumbar puncture is done (Nigrovic et al. 2004). Lumbar puncture is commonly postponed at admission in the most severe cases or prior brain image evaluation in immunocompromised patient or in the presence of specific neurological signals (Riordan & Cant 2002). Nevertheless, CSF samples obtained at a delayed lumbar puncture, because patient conditions are unstable, can be assayed by means of PCR to properly detect gene target with good sensitivity (Borrow et al. 1997, Riordan & Cant 2002). In one study it could be demonstrated the detection of bacterial DNA by PCR in CSF samples taken up to 72 h after commencement of antibiotics (Ragunathan et al. 2000). In this report the PCR has demonstrated a highly specific and sensitive approach to identify S. pneumoniae in infected patients through the detection of ply target compared with culture, Gram stain and latex agglutination test. PCR-based assays have provided useful epidemiological information on the detection and characterization of bacterial meningitis pathogens with a greater sensitivity than culture or direct smear, with excellent specificity (Borrow et al. 1997, Clarke & Edwards 2003). The application of the PCR protocol presented in this study has been effective in the detection of S. pneumoniae from CSF and represents an efficient approach to enhanced surveillance of bacterial meningitis. Although the ply PCR alone may appear sufficient as a screening assay and supports the diagnosis, it is considered prudent to take into account the possibility of discrepant results. PCR like any sampling technique does not solve all diagnostic problems such as the negative results in four positive cases. The failure of PCR in these CSF samples possibly is due to the presence of a substance inhibitory for the reaction. Although less likely, another possible explanation for this result would be inadequate conditions of collection and transport. The presence of PCR inhibitory factors could be greatly reduced when bacterial DNA is isolated upon receipt and it also concentrates the DNA present in the sample (Clarke & Edwards 2003). The PCR assays have been applied with success to enhance surveillance of bacterial meningitis in remote areas in Africa, where conditions of collection and transport is not always adequate (Sidikou et al. 2003, Parent du Chatelet et al. 2005). The absence of reliable laboratories for culture and strain identification of the most common etiologic sources of bacterial meningitis into the vast territory of Brazil, impede microbiological surveillance outside the urban areas. It should be pointed out that in several remote areas like the Amazon region, even in the capitals poor transport infrastructure, human resources, and lack of microbiology laboratories are critical problems for community health. It is possible to store unclotted blood samples at room Th for 1 to 5 days when PCR assay is desired without loss of sensitivity (Kaczmarski & Cartwright 1995). In this study, we validated the ply PCR with CSF specimens kept at room Th for a while or refrigerated at 4°C for some days with compared sensitivity and specificity of results obtained in ideal conditions of collection and transport (Rintamäki et al. 2002, Clrake & Edwards 2003, Messmer et al. 2004). Once this point can be overcome the benefits of PCR-based surveillance of bacterial meningitis in Brazil is clear. The conditions to collect and store fresh CSF specimens are simple and can be implemented at a low cost through a coordination of the Ministry of Health. Despite advances in real-time PCR technology, this method is expensive and its routine use is restricted (Corless et al. 2001); thus the introduction of such technique in local public heath laboratories in Brazil seems to be remote. The PCR assay presented here appears as a satisfactory solution to be implemented at a central level into the reference laboratories (Lacen) located in each state, where the laboratory diagnostic procedures for most infectious diseases are concentrated. The method is simple, easy to carry out, and able to provide specific strain identification in a few hours. Once the DNA is ready to use, the PCR protocol described in this article can be performed rapidly with a turnaround time of 4 h of the start of the assays. The time from the initiation of DNA extraction to the issuing of a report can be shortened when samples are subjected to freeze-thaw, 100°C heat, and then centrifugation to obtain non-purified DNA for PCR. The accuracy of the test compared with the three other laboratory procedures provided evidences the PCR assay has a better diagnostic performance, with which the surveillance of bacterial meningitis can be improved. Nucleic acid based amplification methods have inherent high sensitivity and it plays an important part in the non-culture diagnosis of bacterial meningitis due to its ability to detect DNA from non-culturable bacteria killed by physical or antimicrobial agents. Consequently, the PCR technique should be considered the diagnostic gold standard for positive cases, based on the data presented in this study and those previously published (Virolainen et al. 1994, Salo et al. 1995, Ragunathan et al. 2000, Corless et al. 2001, Rintamäki et al. 2002, Sidikou et al. 2003, Clarke & Edwards 2003, Messmer et al. 2004, Parent du Chatelet et al. 2005). The routine use of this molecular diagnostic technique shall increase laboratory-confirmed cases of meningitis-causing S. pneumoniae over that with culture. It has been proved in countries without reliable microbiology laboratories the introduction of PCR-based assays demonstrated pneumococcal meningitis cases had been underestimated (Parent du Chatelet et al. 2005). It is import to point out, that according the guidance for meningitis surveillance provided by the Brazilian Ministry of Health, the presence of Gram-positive diplococci in a Gram stain CSF smear alone is not a valid criteria for case definition of pneumococcal meningitis (G00.1, ISCD-10), and the use of PCR in this scenario would enhance the surveillance of this pathogen (Fundação Nacional de Saúde 2002). Nevertheless nucleic acid based amplification assays should not be developed as an alternative approach to culture as it gives information on antibiotic resistance and serotype. REFERENCES
Copyright 2006 Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc06095t2.jpg] [oc06095t1.jpg] [oc06095f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}