 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Mem Inst Oswaldo Cruz, Rio de Janeiro, Vol. 101, No. 8, December ,2006, pp.881-885 Human
immunodeficiency virus type Valéria P Cabral, Carla B Cunha, Eneida FL Magalhaes, Lauro F Pinto-Neto*, José Carlos Couto-Fernandez**, Reynaldo Dietze, Mariza G Morgado**, Rodrigo Ribeiro-Rodrigues/+ Laboratório
de Imunologia Celular e Molecular, Núcleo de Doenças
Infecciosas, Universidade Federal do Espírito Santo, Av.
Marechal Campos 1468, 29040-091 Vitória, ES, Brasil *Santa
Casa de Misericórdia de Vitória, Vitória, ES,
Brasil **Laboratório de AIDS & Imunologia Molecular,
IOC-Fiocruz, Rio de Janeiro, RJ, Brasil Financial partial support: Facitec Received
13 June 2006 Code Number: oc06145 Genetic
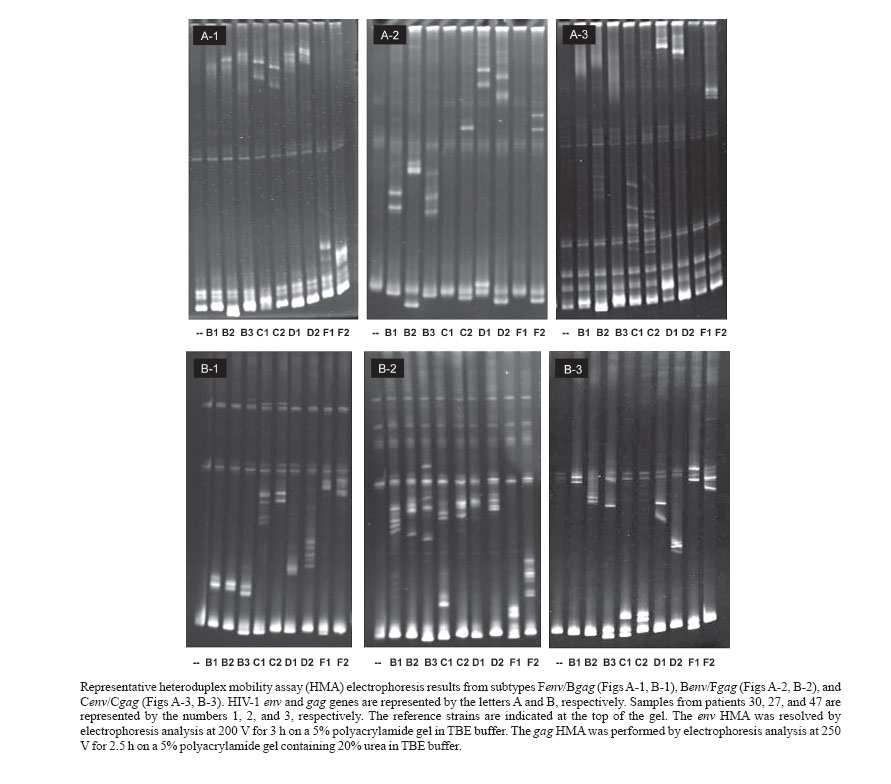
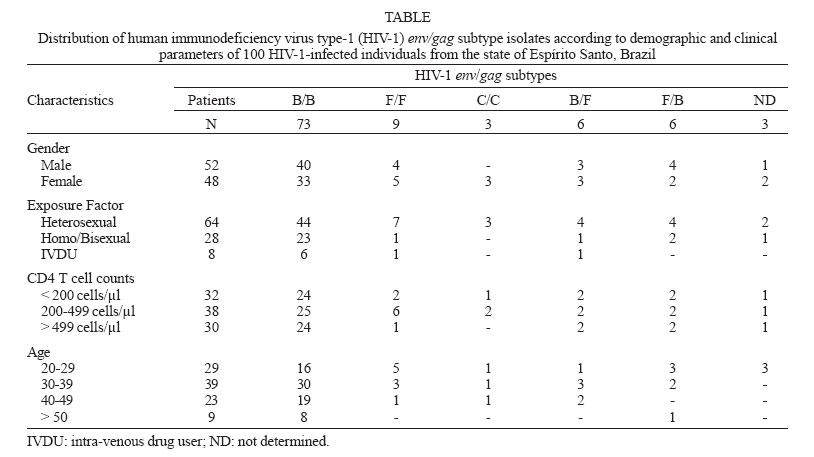
variability of human immunodeficiency virus type Key words: human immunodeficiency virus type 1 (HIV-1) - subtype - Espírito Santo - Brazil Human immunodeficiency virus (HIV) is charac-terized by a high degree of genetic variability, which is due to the high error rate of reverse transcriptase enzyme, the fast turn-over of virions in HIV-infected individuals, the possibility of recombination and changes in viral fitness (Cornelissen et al. 1996). HIV-1 is clustered into three genetic groups: major (M), outlier (O), and non-major-non-outlier (N). At least 9 circulating genetic subtypes (A-D, F-H, J, K) and at least 16 circulating recombinant forms (CRFs), namely CRF01-CRF16, have been identified so far within group M, which accounts for more than 90% of reported HIV/AIDS cases (Vidal et al. 2000, Join United Nations Program on HIV/AIDS 2005). This broad genetic variability has implications for testing, treatment and vaccine development (Moore et al. 2001). Although it has also been hypothesized that distinct subtypes or CRFs may present differences in transmission efficiency and pathogenesis, no consistent evidence has been published to date (van Harmelen et al. 1997, Hu et al. 1999). Even though previous data suggest that all HIV subtypes display a similar sensitivity to antiretroviral drugs, viruses from certain subtypes or geographical regions may occasionally develop resistance to antiretroviral drugs faster than other viral variants (Wainberg 2004). The heteroduplex mobility assay (HMA) has been widely used in Brazil for monitoring subtype distribution. Considering that inter-subtype recombination is an important source of HIV-1 genetic variation, subtype identification using the HMA based on both env and gag genes proved to be a useful tool (Heyndrickx et al. 2000). Identification of HIV subtypes through a constant surveillance is a potent epidemiological tool for monitoring the fast expansion of the HIV pandemic. In Brazil the great majority of HIV isolates are identified as viruses belonging to subtype B. Recently however, the number of non-B and recombinant HIV isolates reported increased significantly (reviewed by Morgado et al. 2002). Most studies conducted in Brazil to evaluate the HIV diversity have been carried out using samples from the Southeastern region, mainly from the states of Rio de Janeiro and São Paulo. In contrast, there is so far no information regarding HIV subtypes circulation in Espírito Santo, another Brazilian Southeastern state, even though 5332 AIDS cases have been reported in this area between 1980 and 2005 (Ministério da Saúde 2005). The city of Vitória, the state capital, has an intense harbor activity, with dozens of ships from different parts of the world docking everyday, creating a favorable condition for the introduction of HIV-1 subtypes and CRFs. In the present study, we evaluated HIV-1 genetic diversity from Espírito Santo in infected individuals using HMA for env and gag genes. MATERIALS AND METHODS Study population - One hundred HIV-1 positive patients attending the HIV/AIDS outpatient clinic at Santa Casa de Misericórdia de Vitória, Espírito Santo, Brazil, were invited to participate in the current study. This study was submitted and approved by the Ethical Committee at Santa Casa de Misericórdia de Vitória, Espírito Santo, prior to patient enrollment. After signing an informed consent, patients had 5 ml of blood drawn by venipuncture in sterile EDTA K3 treated blood collection tubes (Vacuntainer, Becton-Dickinson, CA, US). CD4+ T cell counts were determined by flow cytometry (Facscount, Becton-Dickinson) as described by the manufacturer at the Laboratório Central de Saúde Pública (Lacen-ES). Blood samples were sent to the Cellular and Molecular Immunology Laboratory, Núcleo de Doenças Infecciosas, Universidade Federal do Espírito Santo, within 4 h of collection for viral load determination and DNA extraction. DNA extraction - Proviral DNA was isolated from peripheral blood samples (buffy coat) using the QIAmpâ DNA Mini Kit (QIAGEN, Valencia, US) following the manufacturer's instructions provided with the kit. Purified DNA was aliquoted and stored at 20ºC until use. Polymerase chain reaction (PCR) amplification of HIV env and gag sequences - Proviral DNA samples were amplified using a nested-PCR protocol as described elsewhere (Delwart et al. 1993, Heyndrickx et al. 2000). HMA - The HMA technique was used to identify the HIV subtype present in DNA samples isolated from patients' buffy coats. PCR conditions and HMA subtyping were performed as previously described (Delwart at al. 1993, Heyndrickx et al. 2000). Plasmids containing the subtype reference sequences were provided by the NIH's AIDS Research and Reference Reagent Program. Restriction fragment length polymorphism (RFLP) determination to identify B" subtypes - RFLP to identify B" subtypes among B subtype-positive samples for the env gene followed described techniques (Morgado et al. 1998a, Covas et al. 1998). Statistical analysis - The χ2 test was used to evaluate the relationship between HIV-1 subtype genetic variants and demographic and clinical variables such as gender, clinical status and CD4+ T cell counts. These analyses were performed using Epi Info 2000, version 1.0 for Windows, and results with p < 0.05 were considered statistically significant. We also used 95% confidence intervals (calculated using the exact binomial method) to determine the consistency of our study population with patients in the state AIDS database. These analyses were performed using STATA version 9.0 (STATA Corporation, College Station, TX, US). HIV-1 subtype identification - HIV-1 subtype iden-tification was accomplished in 97 (97%) blood samples from HIV-1 positive patients. In the studied population, subtypes B, C, and F and recombinant B/F HIV isolates were identified (Figure). Subtype B was the most prevalent subtype identified in 73 out of 97 samples (75.3%, 95%CI: 66.7-83.8). Twenty-four out of 97 (24.7%) samples cor-responded to non-B and recombinant virus as follows: subtype F (9.3%, 95%CI: 3.5-15.0), subtype C (3.1%, 95%CI: 0-6.5), and recombinant B/F subtypes (12.4%). Two distinct B/F recombinant genomes were identified among the HIV-1 isolates that were grouped as Benv/Fgag (6.2%, 95%CI: 1.4-11.0) and Fenv/Bgag (6.2%, 95%CI: 1.4-11.0) subtypes. The identification of the Brazilian subtype B variant, known as subtype B", was achieved by Fok I RFLP assay. Twenty-two (27.8%) out of 79 subtype Benv HIV isolates were identified as Brazilian subtype B" (data not shown). Correlation between HIV-1 subtype and demographic or clinical variables - Socio-demographic, clinical and laboratorial data are summarized in the Table. No significant association between a given HIV-1 subtype and demo-graphic or clinical variables was encountered in the studied population. Although the HIV genetic diversity is well documented for the states of São Paulo and Rio de Janeiro, data for the remaining Southeastern states (Minas Gerais and Espírito Santo) are either incomplete or based on small sample sizes. To our knowledge, this is the first study designed to evaluate the genetic diversity of HIV isolates in Espírito Santo. HIV-1 subtypes B, F, and C as well as B/F recombinant genomes were identified by HMA and their frequency was determined. Subtype B (75.3%) was the most prevalent subtype followed by subtype F (9.3%) and subtype C (3.1%). Recombinance between B/F subtypes represented 12.4% of all isolates tested. Despite the fact that the state of Espírito Santo has three important harbors (Vitória, Tubarão, and Capuaba), with an intense shipping activity, which could facilitate the introduction of new HIV subtypes from other regions of the world, data presented here show that the observed subtype distribution was similar to those previously reported for other Southeastern states (Rio de Janeiro and São Paulo), with a predominance of the B subtype (Morgado et al. 2002). Subtype B is the most prevalent subtype in the Southeastern, Northeastern and Central-Western part of Brazil (Morgado et al. 1998b, Stefani et al. 2000, Gadelha et al. 2003). Different patterns of HIV-1 subtype distribution are frequently observed in Brazil, varying according to the geographical region (Morgado et al. 2002). In the present work, HIV-1 subtype C isolates were found in 3% of studied samples, what concurs with literature data for other Southeastern states (Brazilian Network for HIV Isolation and Characterization 2000). This finding also agrees with the hypothesis that subtype C has been disseminated in the country following a South-North gradient pattern. Interestingly, although reported previously in Rio de Janeiro (Janini et al. 1996, Couto-Fernandez et al. 2006), subtype D was not identified in our study. Although the observed frequency of subtype F (9.3%) in our study was similar to other Southeastern states' observations, Couto-Fernandez et al. (2005) reported a lower frequency (4.9%) of subtype F among samples from Rio de Janeiro HIV patients. It is known that most subtype F characterized by either partial sequencing or HMA based only on the env gene turned out to be B/F recombinant isolates when re-analyzed by either full sequencing or HMA on gag and env genes, with the occurrence of a "pure" F subtype isolate being rare (Carr et al. 2001). Therefore, our results support previous findings showing that B and F (env/gag) recombinants are present at high frequencies within HIV-1 infected populations in different regions in Brazil (Guimarães et al. 2002). We were neither able to confirm nor establish a significant correlation between the HIV-1 subtypes circulating in Espírito Santo with either clinical or epidemiological parameters. The lack of correlation between subtypes and clinical/epidemiological data has also been reported by other authors in Brazil (Guimarães et al. 2001, Turchi et al. 2002). It has been estimated that 10% of all HIV isolates circulating in the world are recombinant virus (McCutchan et al. 2000). Indeed, we found that 12.4% of all studied samples were from recombinant isolates from subtypes B and F (6.2% Benv/Fgag and 6.2% Fenv/Bgag). Although the HMA technique is accurate and suitable for subtype identification, these B and F samples should be considered only as potentially recombinants. For a sample to be regarded as a true recombinant, breakpoints between the studied regions need to be detected, what is achieved by nucleotide sequencing. A subtype-B variant, known as the Brazilian subtype B (subtype B"), which differs from the traditional subtype B by the presence of a sequence GWGR instead of the conserved sequence GPGR at the top of the V3 loop in the viral envelope, was identified in 27.8% of samples in our study. Previous studies using the same metho-dological approach found B" subtype frequencies ranging from 30 to 57%, depending on the geographic origin of the studied population (Covas et al. 1998, Morgado et al. 1998a, Gadelha et al. 2003). As before, no associations between B" and the different patient exposure categories were found. Although the importance of the Brazilian subtype B in the AIDS epidemic is not fully understood, its high prevalence could be an important molecular epide-miological parameter of the HIV pandemic and therefore relevant to be monitored for future vaccine development and testing in Brazil.
Copyright 2006 Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc06145t1.jpg] [oc06145f1.jpg] |
| |||||||||

{kind=link}
{kind=link}