 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Mem Inst Oswaldo Cruz, Rio de Janeiro, Vol. 101, No. 8, December ,2006, pp.925-928 Concurrent infection with dengue virus type-2 and DENV-3 in a patient from Ceará, Brazil Fernanda Montenegro de Carvalho Araújo, Rita Maria Ribeiro Nogueira*/+, Josélio Maria Galvão de Araújo*, Izabel Letícia Cavalcante Ramalho, Maria Lucia Feitosa de Sá Roriz, Maria Elizabeth Lisboa de Melo, Ivo Castelo Branco Coelho** Laboratório
Central de Saúde Pública do Ceará, Fortaleza,
CE, Brasil *Laboratório de Flavivirus, Instituto Oswaldo
Cruz-Fiocruz, Av. Brasil 4365, 21040-900 Rio de Janeiro, RJ, Brasil
**Universidade Federal do Ceará, Fortaleza, CE, Brasil Financial support: CNPq (501564/03-9), Faperj (E-26/152.490/2002), Funasa Received
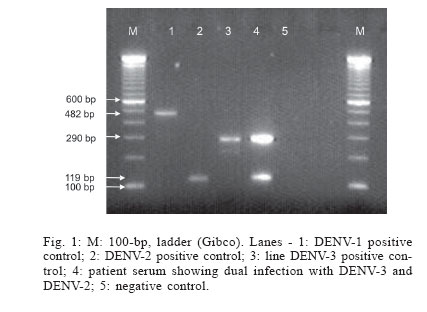
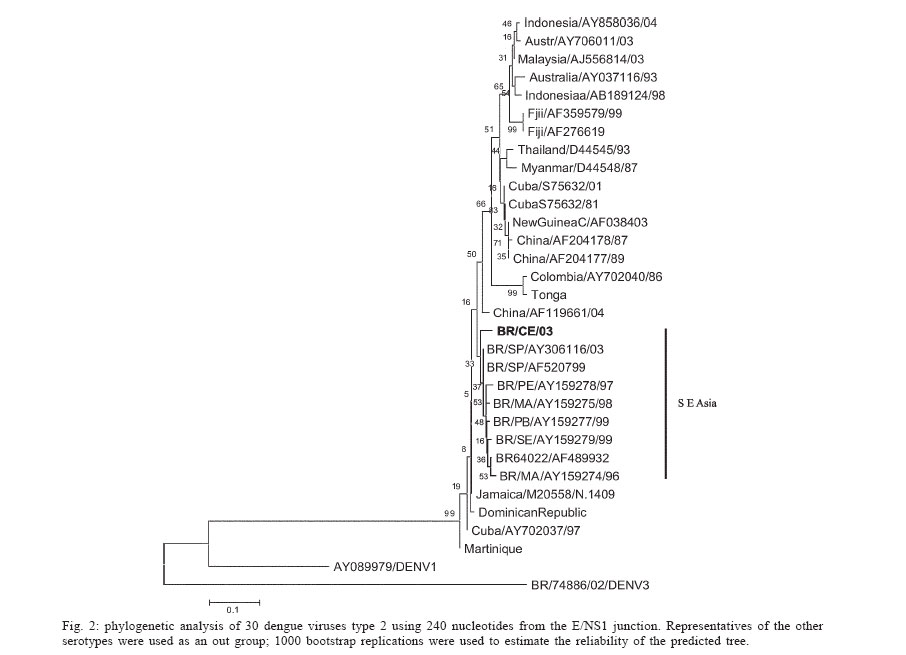
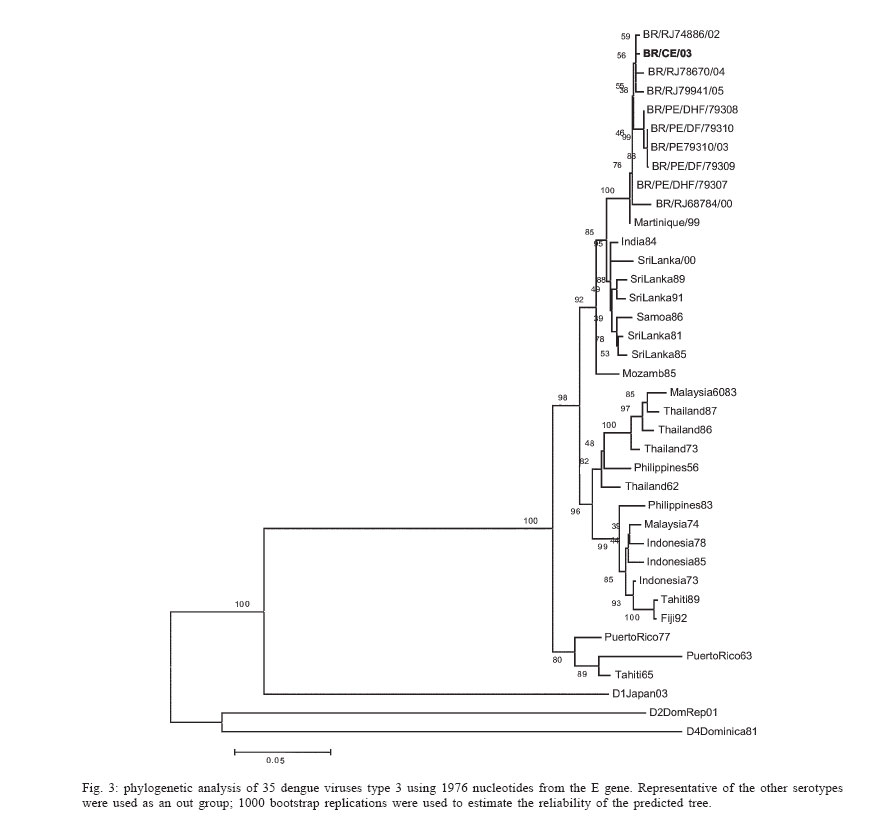
9 June 2006 Code Number: oc06152 Dengue outbreaks have occurred in several regions in Brazil and cocirculating dengue virus type 1 (DENV-1), DENV-2, and DENV-3 have been frequently observed. Dual infection by DENV-2 and DENV-3 was identified by type-specific indirect immunofluorescence assay and confirmed by reverse transcription polymerase chain reaction in a patient in Ceará with a mild disease. This is the first documented case of simultaneous infection with DENV-2 and DENV-3 in Brazil. Sequencing confirmed DENV-2 and DENV-3 (South-East/American) genotype III and (SriLanka/India), genotype III respectively. Key words: dengue - concurrent infection - DEN2 - DENV-3 - Ceará - Brazil Dengue is one of the most important arboviral infections affecting humans, caused by one of the four serotypes of dengue virus (DENV-1, 2, 3, 4). They belong to the genus Flavivirus, family Flaviviridae (Gubler 1998). The prevalence of this disease has grown in recent decades and is now endemic in more than 100 countries in Africa, the Americas, the Eastern Mediterranean, Southeast Asia, and the Western Pacific (Chaturvedi et al. 2004). Since 1986, dengue epidemics have been reported in Brazil, initially involving DENV-1 and after 1990, DENV-2. With the introduction of DENV- 3 in 2000, three serotypes are now circulating in Brazil (Nogueira et al. 2005). With the change in the epidemiological pattern that has occurred in approximately 30 years, the Americas, and more recently Brazil, can be considered a hyperendemic region, with multiple cocirculating serotypes. Since 1986, the state of Ceará began reporting dengue transmission with epidemic peaks in 1987, 1990, 1994, and 2001. Only DENV-1 was in circulation until 1994, when DENV-2 was introduced. This serotype caused a large epidemic with 47,789 notified cases, in which 14 deaths have been reported (Souza et al. 1995). In March 2002, DENV-3 was first isolated in Ceará by the Central Laboratory of Public Heath, thus it became an area of high endemicity with three cocirculating serotypes. Interestingly, in spite of the high or hyperendemicity of dengue viruses in some populations, relatively few cases of double infection have been reported (Gubler et al. 1985, Laille et al. 1991, Maneekarn et al. 1993, Sisouk et al. 1995). More recently two cases were reported in Brazil involving DENV-1 DENV-2 (Santos et al. 2003). Simultaneous infection with DENV-2 and DENV-3 was reported by Kanesa-Thasan et al. (1994), by Wang et al. (2003) during an outbreak in Taiwan in 2000, and more recently by Wenming et al. (2005), who confirmed simultaneous infection with dengue 2 and 3 viruses in a Chinese patient returning from Sri Lanka. A case of concurrent infection due to DENV-2 and DENV-3 was confirmed during an outbreak of dengue in the state of Ceará in the Northeastern region of Brazil in 2003. The patient was a 36 year-old male who lived in Tauá, a town of approximately 52,000 inhabitants, located 337 km far from Fortaleza city, the state capital. The onset of symptoms started on February 2, with high fever, headache, arthralgia, myalgia, retrobulbar pain, and asthenia. No hemorrhagic manifestation and no severe signs were observed, and the patient was fully recovery after one week. A mild disease, in spite of dual infection, has been observed by other authors and does not support the hypothesis that double infection with dengue viruses leads to more severe hemorrhagic disease (Gubler et al. 1985, Santos et al. 2003). Interestingly, DENV-2 and DENV-3 viruses have been well documented in severe cases in Brazil (Nogueira et al. 2001, 2005). The serum was obtained two days after the onset of symptoms and the procedures for virus isolation and virus identification were performed using the protocol previously described by Nogueira et al. (2001) using monoclonal antibodies. Polymerase chain reaction directly from the serum has been suggested in order to avoid selection of a dengue serotype during attempts of virus isolation in tissue culture. The present results show that both serotypes were identified, by the virus isolation process and by molecular method (Fig. 1). For RNA extraction the supernatant of C6/36 was extracted using a QIAmp Viral Mini Kit (Qiagen, US) according to the manufacturer's protocol. Reverse transcription (RT-PCR) for detecting and typing DENV in acute sera and tissue culture fluid were carried out according to Lanciotti et al. (1992). Primers for sequencing DENV-2 and DENV-3 were performed according to Rico-Hesse (1990) and Lanciotti et al. (1994), respectively. Fig. 1 shows gel exhibiting two bands corresponding DENV-2 and DENV-3 viruses. Figs. 2 and 3 show the phylogenetic analysis of isolates corresponding to DENV-2 E/NSI (Rico-Hesse 1990) and DENV-3 prM/M/E gene regions (Lanciotti et al. 1994). The genotypes found corresponded to genotype III (South-East/Asia) and genotype III (Indian Subcontinent) DENV-2 and DENV-3, respectively. Vertical transmission is of great epidemiological importance and suggests that vector mosquitoes may play an important role in the maintenance (Castro et al. 2004) of virus in the environment and mosquitoes may act as reservoirs of these viruses (Joshi et al. 2006). Laboratory data demonstrated that the mosquito Aedes aegypti may be infected with double combinations of different arboviruses and that it is also capable of transmitting these viruses simultaneously. According to Wenming et al. (2005) it is possible to assume that mosquitoes infected with DENV-2 and DENV-3 may transmit them both in areas where two or more serotypes of the virus exists, together with a high prevalence of the vector. In spite of both serotypes involved in this case can lead to severe form of dengue in Brazil, a dual infection did not caused a dengue severe clinical presentation in this patient. Understanding of the DHF pathogenesis is not complete so far and two distinct hypotheses to explain the mechanism of DHF have been suggested. Immune responses and viral virulence have been considered as two major factors responsible for the pathogenesis (Kurane 2001). Serological tests showed a primary infection in this case; therefore it is plausible to admit that this case should be classified as dengue fever, which represents the majority of dengue infection. This is the first documented case of dual infection with DENV-2 and DENV-3 in Brazil. REFERENCES
Copyright 2006 Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc06152f2.jpg] [oc06152f3.jpg] [oc06152f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}