 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Mem Inst Oswaldo Cruz, Rio de Janeiro, Vol. 101,Suppl. I, October ,2006, pp. 125-132 Attaining the minimum target of resolution WHA 54.19 for schistosomiasis control in the Rainforest Zone of the state of Pernambuco, Northeastern Brazil Tereza C Favre/+, Ricardo AA Ximenes*, Aline F Galvão, Ana Paula B Pereira, Tereza N Wandereley**, Constança S Barbosa***, Otávio S Pieri Departamento de Biologia, Instituto Oswaldo Cruz-Fiocruz,
Av. Brasil 4365, 21045-900 Rio de Janeiro, RJ, Brasil *Departamento de Medicina
Tropical, Universidade Federal de Pernambuco, Recife, PE, Brasil **Laboratório
de Endemias, Secretaria de Saúde de Pernambuco, Recife, PE, Brasil ***Departamento
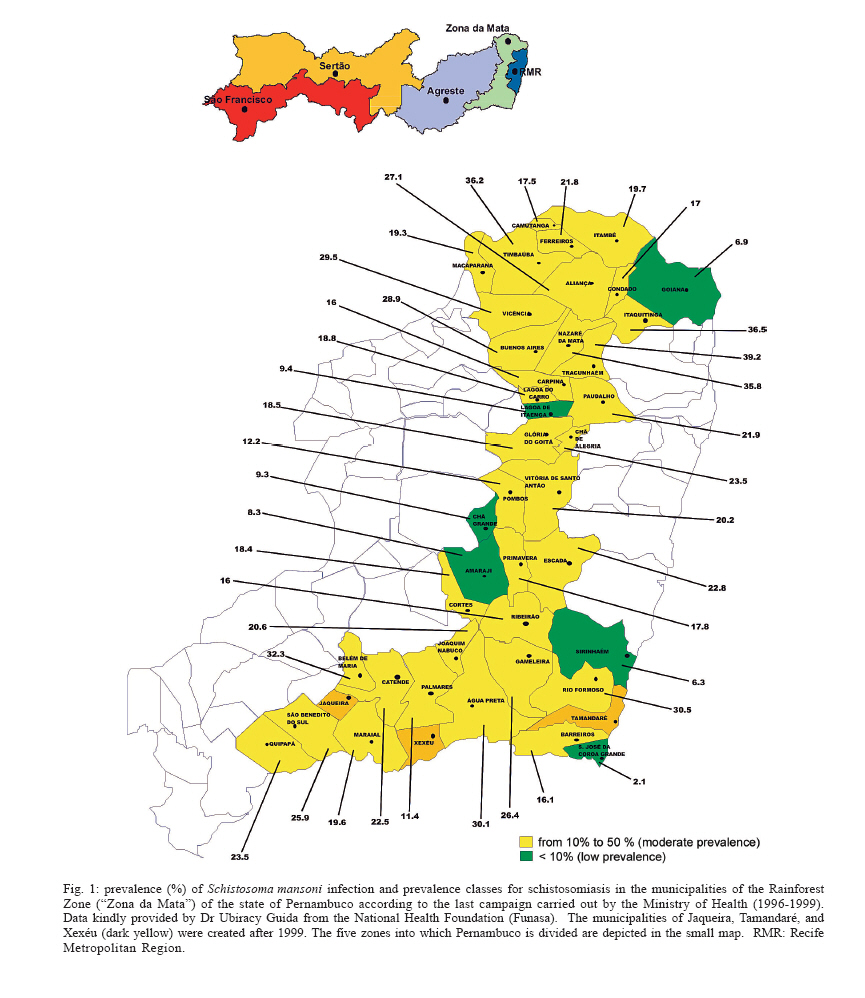
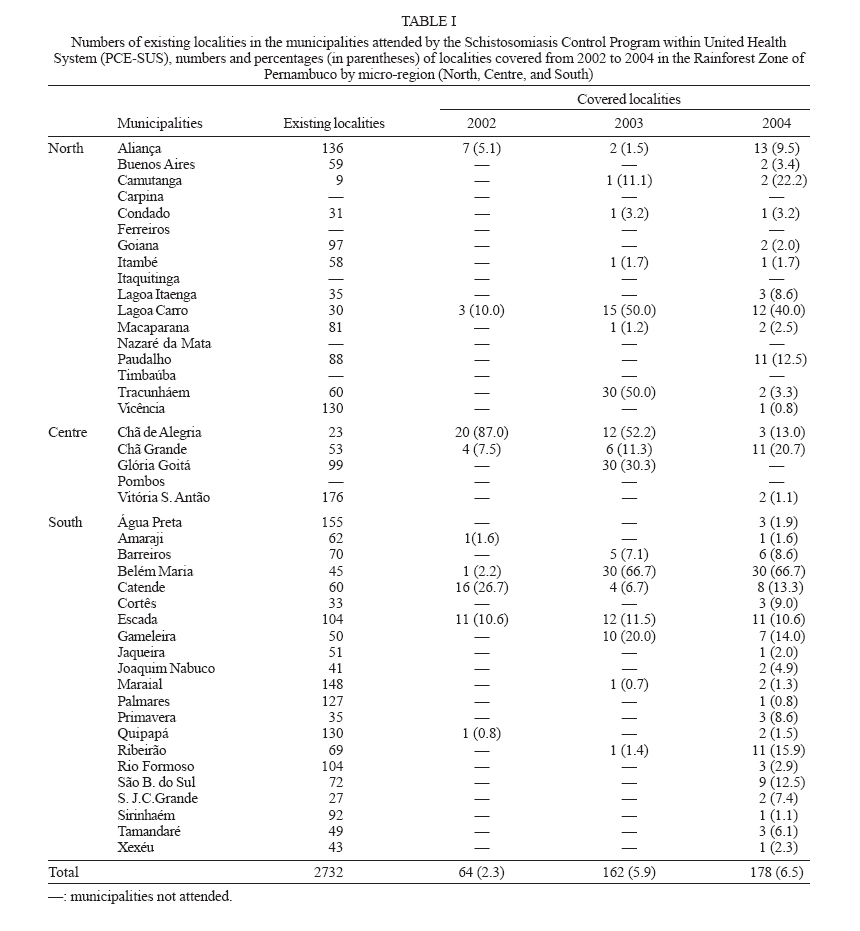
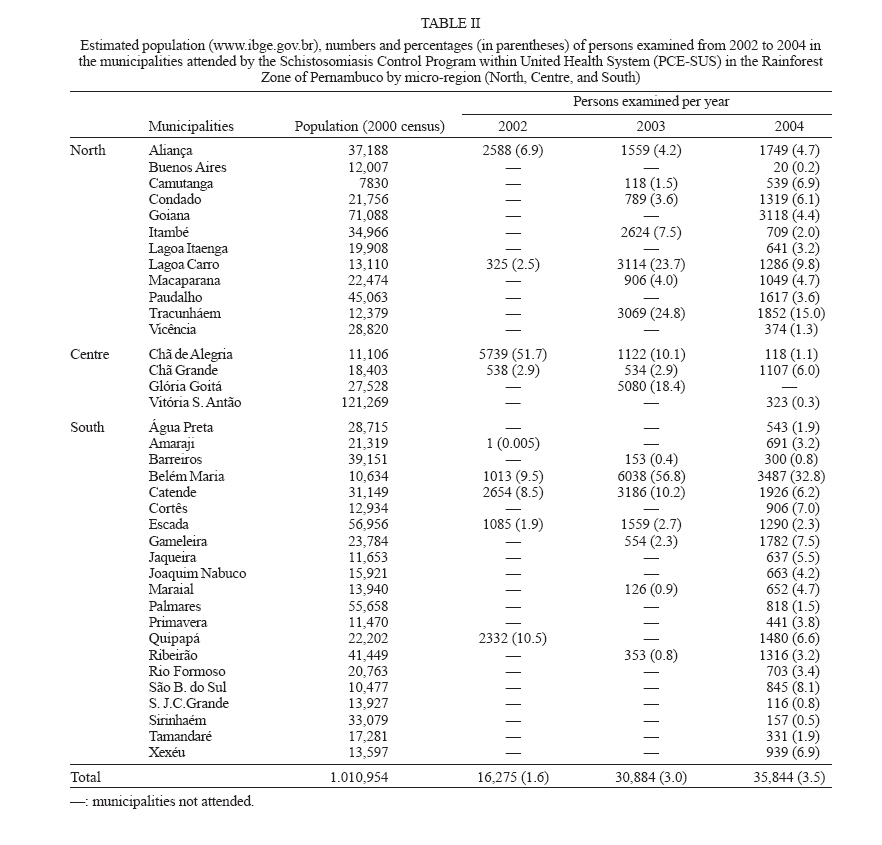
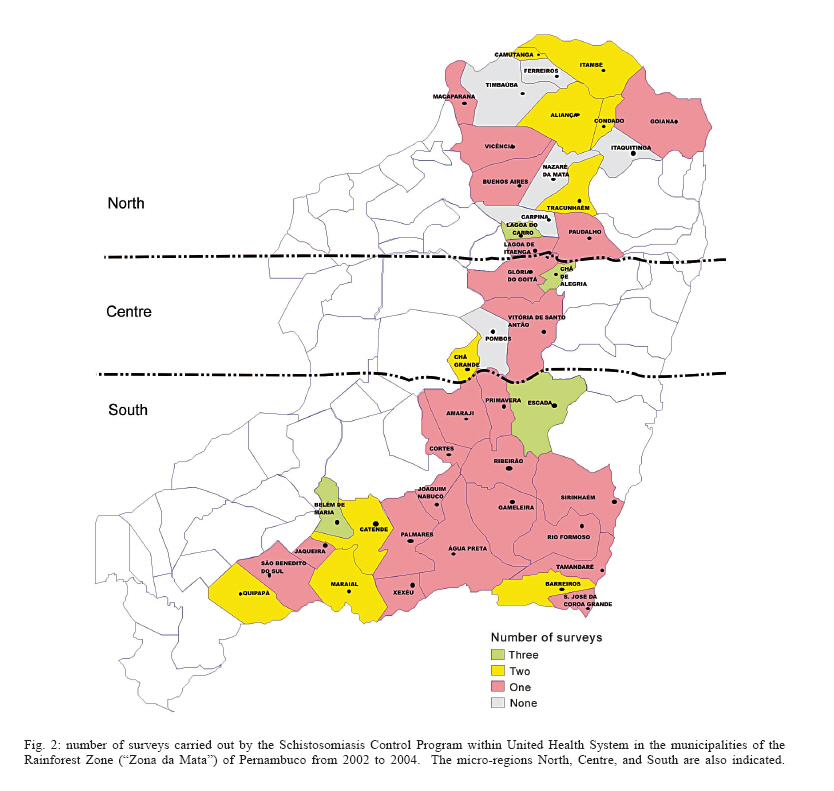
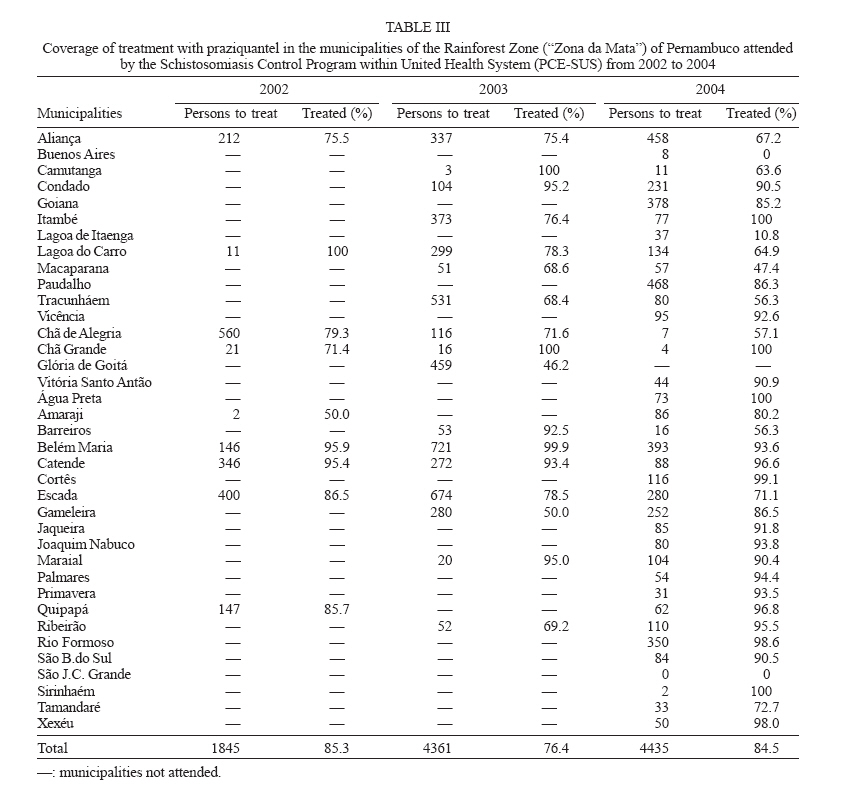
de Parasitologia, Instituto Aggeu Magalhães-Fiocruz, Recife, PE, Brasil Received 25 May 2006 Code Number: oc06178 Resolution 19 of the 54th World Health Assembly (WHA-54.19) urged member nations to promote preventive measures, ensure treatment and mobilize resources for control of schistosomiasis and soil-transmitted helminthiases (STH). The minimum target is to attend 75% of all school-age children at risk by year 2010. The Brazilian Ministry of Health (MoH) recommends biennial surveys of whole communities and treatment of the positives through the Schistosomiasis Control Program within the Unified Health System (PCE-SUS). However, by 2004 the PCE-SUS had covered only 8.4% of the 1.2 million residents in the Rainforest Zone of Pernambuco (ZMP). Six of the 43 municipalities still remained unattended. Only three of the municipalities already surveyed reached coverage of 25% or more. At least 154 thousand children in the 7-14 years old range have to be examined (and treated if positive) within the next five years to attend the minimum target of the WHA 54.19 for the ZMP. To make this target feasible, it is suggested that from 2006 to 2010 the PCE-SUS actions should be complemented with school-based diagnosis and treatment, involving health and educational organs as well as community associations to include both children in schools and non-enrolled school-age children. Key words: schistosomiasis - control - Pernambuco - Brazil Schistosomiasis remains a serious public health problem both at the global (Engels et al. 2002) and national (Coura & Amaral 2004) levels. As regards the endemic area of the state of Pernambuco, a number of studies have identified causal factors in the scope of bio-ecological, cultural, economic, demographic, and behavioural aspects (Barbosa & Barbosa 1998, Freese de Carvalho et al. 1998, Moza et al. 1998, Ximenes et al 2000, 2001, 2003). Those studies make it clear that the provision of both piped water and sewage system connections for most households, increased investments in education and health and socioeconomic changes improving the living conditions of disadvantaged groups might lead to the permanent control of the disease. In May 2001, all member nations of the World Health Organization (WHO) committed themselves with implementing an integrated strategy for prevention and control of schistosomiasis and soil-transmitted helminthiases (STH), through Resolution 54.19 of the World Health Assembly (WHA 54.19). The Assembly recognized that sanitation and safe-water supply are essential. It also reassured that the best measures to reduce morbidity and mortality as well as to improve health and development of the infected communities are the regular treatment of the high-risk groups, specially school-aged children, and the access to drugs through the primary health care services. WHA 54.19 set the minimum target of treating at least 75% of all school-aged children from the endemic areas by year 2010. WHO made a partnership with international agencies, research and education institutions and non-governmental organizations (PPC 2002, WHO 2005a) to implement those recommendations. It also formed an Expert Committee to provide clear and strategic orientation on how to implement the recommendations (WHO 2002). A series of articles were published in internationally recognized periodicals systematizing the most recent technical and scientific information about the control of schistosomiasis and STH (Allen et al. 2002, Savioli et al. 2002, 2004 a, b, 2005, Crompton et al. 2003, Olds 2003, Richter 2003, Colley & Sear 2004). The current strategies for schistosomiasis control recommended by the Ministry of Health (MoH) and the WHO are similar in various important aspects: (i) emphasis on preventive measures such as health education, safe-water supply, and sanitation; (ii) snail control only as an auxiliary measure; (iii) close interaction among the national, regional, and local levels of health organs; (iv) local availability of praziquantel for the cases diagnosed through the health services. However, as regards diagnosis and treatment the two organs have different strategies. The MoH currently recommends (i) identification of infected persons through stool surveys carried out biennially by the municipal health organs in whole communities from the endemic areas and (ii) treatment of the diagnosed cases through the local health services (Funasa 1998). In contrast, the WHO proposes treatment targeted at high-risk groups (school-aged children, adults with occupations requiring frequent contact with transmission foci) instead of whole communities. As MoH's current guidelines were defined prior to resolution WHA 54.19, there is no specific orientation regarding the year 2010 minimum target for the endemic areas of schistosomiasis in Brazil. However, if whole community surveys followed by selective treatment are carried out at two-year intervals as recommended, the minimum target will be easily attained. Therefore, the issue is how effectively those recommendations have been implemented by the municipalities to meet the expectations. The Rainforest Zone ("Zona da Mata") of Pernambuco (ZMP), also known as sugar-cane zone, remains one of the most concerned endemic areas of schistosomiasis in Brazil. It occupies 8456 km2 between coordinates 35°-36° W and 7°-9° S enclosing 43 municipalities. According to the 2000 census (www.ibge.gov.br), the population totaled 1,207,324 inhabitants 31% of which residing in rural areas. The school-aged population (7-14 yrs) added up to 205 thousand children, 17% of the total population. By 2004, there were 187,742 children from that age range enrolled in 1415 schools of elementary education. Between 1977 and 1996 the MoH accomplished four campaigns of diagnosis and treatment in the ZMP, covering an average of 39 municipalities per campaign (Favre et al. 2001). By the end of that period overall prevalence of infection by Schistosoma mansoni had dropped only 9.1 percentage points (pp), from 35.4 to 26.3%. From 1996 to 1999 the MoH carried out its last campaign in that Zone, covering 40 municipalities. This enabled to identify five municipalities in the low prevalence class (less than 10%) and 35 in the moderate prevalence class (between 10 and 50%) according to WHO (2002) classification (Fig. 1). By 1999 the Unified Health System (SUS) took over the Program for Schistosomiasis Control (PCE) in Per-nambuco, making the municipalities responsible for the activities of diagnosis, treatment, and surveillance, as well as the definition of intervention priorities. In the ZMP the PCE-SUS was implemented only by 2001, with the goal of undertaking biennial surveys in all localities and treating the positive through the local health units. The present work intends to evaluate whether the PCE-SUS (i) has followed the current guidelines of the MoH for schistosomiasis diagnosis and treatment by providing adequate population coverage and (ii) is able to attain the minimum target of resolution WHA 54.19 for year 2010 in the municipalities of the ZMP. Preventive, broader control measures such as health education, water supply and sanitation have not been systematically implemented by the PCE-SUS; therefore they will not be considered in this paper. METHODS The 2001-2004 annual reports from the Health Department of Pernambuco State (SES/PE) on schistosomiasis survey and treatment activities were used as source documents for the present work. The data were tabulated by micro-region (north, centre, and south), municipality, year, locality, population, number of persons examined, number of positives for S. mansoni, number of positives treated, number of non-treatment cases (refusal, absence, contra-indication). The data were transferred to a statistical software (Systat 11) for calculating the following indices (Mon-tresor et al. 2002) grouped by micro-region, municipality, year and locality: percentage of examined in the population, percentage of treated and percentage of no-treated due to refusal, absence or contra-indication. The data regarding prevalence of infection will be evaluated in a separate paper (Favre et al. 2006). RESULTS The SES/PE reported for year 2001 only 18,667 exams in five municipalities of the ZMP, with no information about the localities covered. Therefore, they will not be considered here. As regards the period from 2002 to 2004 there are data on 83,003 exams at the locality level, which will be considered as follows. At four years after resolution WHA 54.19, 37 (86%) out of 43 municipalities from ZMP had been attended by the PCE-SUS, leaving six of them without coverage. During the 2002-2004 period only 404 (14.8%) of the 2732 existing localities were surveyed. Nine (20.9%) municipalities in 2002, 17 (39.5%) in 2003, and 36 (83.7%) in 2004 had at least one locality covered. However, less than 10% of the existing localities were attended in 22 municipalities. The situation was particularly critical in four municipalities (Jaqueira, Sirinhaém, Vicência, Xexéu), where only one locality was covered over that period (Table I) Percentages below 10% of persons examined occurred in seven (77.8%) of nine municipalities attended in 2002, 11 (64.7%) of 17 in 2003, and 33 (91.7%) of 36 in 2004. Only three municipalities registered 25% or more persons examined over that period (Table II). Only 77 localities were surveyed more than once from 2002 to 2004. Five localities were surveyed yearly: the municipal centre of Belém de Maria (one out of 36 localities covered), the municipal centre of Lagoa do Carro (one out of 17 localities covered), Sítio Brasil and Sítio Lagoinha (two out of 20 localities covered in the municipality of Chã de Alegria), and Canto Escuro (one out of 28 localities covered in the municipality of Escada). The municipalities with localities surveyed twice were: Aliança (two out of 20 covered), Barreiros (one out of 10), Belém de Maria (25 out of 36), Camutanga (one out of two), Catende (four out of 24), Chã de Alegria (11 out of 20), Chã Grande (six out of 15), Escada (four out of 28), Lagoa do Carro (11 out of 17), and Tracunhaém (two out of 31). In the municipalities of Condado, Itambé, Maca-parana, Maraial, and Quipapá one locality was covered in two surveys. In the remaining 22 municipalities, there was only one survey in the localities covered (Fig. 2). Table IIIshows that treatment coverage over 70% were obtained in eight out of nine municipalities attended in 2002, 12 of 17 in 2003 and 25 of 36 in 2004. Both in 2002 and 2004 compliance was around 85%. Over that period only 1,900 (18.7%) out of 10,644 cases were left untreated. Among the reasons for non-treatment there were 62.1% absences, 35.3% contra-indications, and 2.6% refusal. In five out of seven occurrences in which compliance reached 100%, the average number of infected persons was 7.2. That was the case with seven out of 11 localities covered in the municipality of Paudalho in 2004 and with 13 other localities in different municipalities. DISCUSSION The recommendation made by the MoH that all population from the endemic municipalities should be surveyed biennially for treatment is far from being accomplished in the ZMP. Firstly, the six municipalities not yet reached by the PCE-SUS have left unattended about 200 thousand people under risk of infection. Secondly, only three municipalities achieved coverage of 25% or more in the 2002-2004 period. Assuming that any person was only examined once over that period, the total number of exams would not have exceeded 6.8% of the ZMP population. Considering that the school-aged children in the ZMP are 17% of the total population and taking into account that the PCE-SUS do not give priority to any age group, the surveys carried out from 2002 and 2004 would have attended 14 thousand school-aged children to the utmost. To accomplish the minimum target of year 2010 it is necessary to attend at least 154 thousand school-aged children (75% of the estimated total). This would require the examination of 461 thousand persons from all age groups, according to MoH recommendations. As regards compliance to treatment, the relatively high percentages of absentee may be due to recently adopted guidelines for drug administration by the SES/PE. Before the implementation of PCE-SUS, medication was carried out house to house by the health agents in charge of the stool surveys (Funasa 1998). As a result, the cases of absence were relatively few. At present, praziquantel can only be administered under medical prescription, requiring the attendance of the patient at a health centre. This usually involve many hours of travel and waiting, which may discourage compliance. It is interesting to note that the cases of 100% compliance probably resulted from passive detection through the routine health services and not from active search by the PCE-SUS. With regard to the relatively high percentages of non-treatment due to contra-indication, it should be of interest to evaluate whether the medical staff in charge of prescribing praziquantel in the local health units is unaware of the recent recommendations for the use of this drug. According to WHO (2003), praziquantel can be regarded as the safest among antihelminthic drugs. The risks during pregnancy and lactation are practically none, and all effort should be made to ensure the inclusion of the highly vulnerable group of pregnant and lactating women in any deworming program. The only contra-indication is hypersensitivity to the active component of the formula (Olds & Dasarathy 2000). If an evaluation of knowledge, attitude and practice (KAP) regarding praziquantel prescription would confirm the above hypothesis, the SES/PE could promote short-term update courses based on a recent review about the drug aimed specifically at the clinical practice (Cioli & Pica-Mattoccia 2003). A series of seminars on that subject has been carried out in 2002-2003 to doctors and nurses of the Family Health Program (PSF) from four municipalities in the Recife Metropolitan Region (Jaboatão, Itamaracá, Ipojuca, and Igarassu). Reports on the PCE-SUS activities in other states of the endemic area of schistosomiasis in the Northeastern region indicate contrasting situations regarding the attendance of the recommended biennial goals by the MoH. Thus, the Computerized System of the Schistosomiasis Control Program (SISPCE) (http://dtr2001.saude.gov.br/svs/epi/esquis/esquis00.htm) records a total of 1.5 million persons examined between 1997 and 2004 in Alagoas state, covering 53% of the population of 2.8 million according to the 2000 census (www.ibge.gov.br). For the state of Sergipe, however, the SISPCE informs that only 25% of the population was covered from 1996 to 2004. Therefore, it is mandatory that the PCE-SUS identifies the problems involved in the nonattendance to its own goals and evaluates whether coverage can be improved within the capacity of the municipalities. It is possible that, in face of the context being experienced, the municipalities have already reached their maximum capacity, making it unfeasible to attend to any additional demand. In the ZMP, the main limiting factors are probably the lack of material and human resources for the PCE-SUS activities at the municipal level as well as the overload of duties attributed to the local health services. In both cases, the PCE-SUS should give special attention to the most troubled municipalities and involve local educational organs as well as community associations to overcome the obstacles. The following strategy may be recommended to start now for attaining the minimum target of resolution WHA 54.19, based on the prevalence classes obtained in the last survey carried out by the MoH in 1996-1999 (Fig. 1) as well as the number of surveys carried out by the PCE-SUS in 2002-2004 (Fig. 2): (i) all six municipalities left unattended and 18 of those attended only once by the PCE-SUS had moderate prevalence. They should aim at undertaking stool surveys in all elementary schools and treating the infected school-aged children at a biennial basis. Even considering that school evasion in the ZMP may reach 35% (Condepe 2000), that scheme could provide coverage to 86,385 (65%) out of 132,900 children aged 7-14 yrs living in those municipalities (year 2000 Census). The local educational and health organs could act together with the community associations to include non-enrolled school-aged children; (ii) the 19 municipalities attended more than once by the PCE-SUS should intensify diagnosis and treatment activities at the community level to increase coverage to at least 75% of the population; (iii) those municipalities remaining with prevalence above 10% should implement strategies of Information, Education and Communication (IEC) as well as sanitation and safe-water supply within the Integrated Covenanted Program for Epidemiology and Disease Control (PPI/ECD). The above strategy should not be regarded as an intrusion on the municipal priorities, but as a contribution towards the attainment of the minimum target of resolution WHA 54.19 without compromising the PCE-SUS goals. ACKNOWLEDGEMENTS To Dr Ubiracy Guida (in memoriam), from the National Health Foundation, for kindly providing the prevalence data of the 1996-1999 survey. REFERENCES
Copyright 2006 Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc06178t2.jpg] [oc06178f2.jpg] [oc06178t1.jpg] [oc06178t3.jpg] [oc06178f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}