 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Mem Inst Oswaldo Cruz, Rio de Janeiro, Vol. 101,Suppl. I, October ,2006, pp. 279-282 Disagreement between ultrasound and magnetic resonance imaging in the identification of schistosomal periportal fibrosis Luciana CS Silva/+, Ana CF Pereira, Leonardo C Queiroz*, Luciene M Andrade**, Carlos MF Antunes, José R Lambertucci Serviço de Doenças Infecciosas e Parasitárias,
Faculdade de Medicina *Serviço de Radiologia, Hospital das Clínicas,
Universidade Federal de Minas Gerais, Av. Alfredo Balena 190, sala 3035, 30130-100
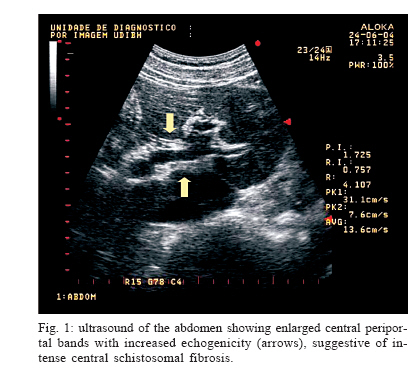
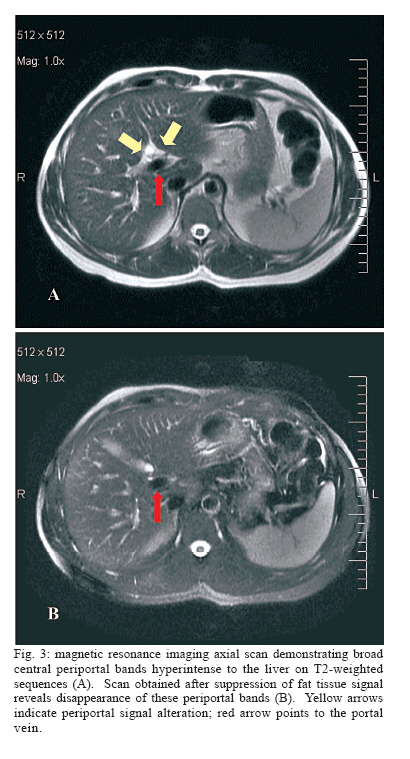
Belo Horizonte, MG, Brasil Partial financial support: CNPq Received 25 May 2006 Code Number: oc06201 Abdominal ultrasound (US) has been widely used in the evaluation of patients with schistosomiasis mansoni. It represents an important indirect method of diagnosis and classification of the disease, and it has also been used as a tool in the evaluation of therapeutic response and regression of fibrosis. We describe the case of a man in whom US showed solid evidence of schistosomal periportal fibrosis and magnetic resonance imaging revealed that periportal signal alteration corresponded to adipose tissue which entered the liver togheter with the portal vein. Key words: schistosomiasis - Schistosoma mansoni - ultrasound - magnetic resonance imaging Abdominal ultrasound (US) has been widely used in the evaluation of patients with schistosomiasis mansoni. It represents an important indirect method of diagnosis and classification of the disease (Abdel-Latif et al. 1981, Hussain et al. 1984, Fataar et al. 1984, Cerri et al. 1984, Homeida et al. 1988a, b, Abdel-Wahab et al. 1989, Pinto-Silva et al. 1994, Gerspacher-Lara et al. 1998, Gerspacher-Lara 1999, Niamey Working Group 2000, Ritcher et al. 2001, Lambertucci et al. 2001). US has also been used as a tool in the evaluation of therapeutic response and regression of fibrosis in schistosomiasis (Massoud et al. 1986, Homeida et al. 1988c, Homeida et al. 1991, Doehring-Schwerdtfeger et al. 1992, Boisier et al. 1998, Frenzel et al. 1999, De Jesus et al. 2000, Cota et al. 2006). Ultra-sonographic examination of subjects with hepatosplenic schistosomiasis has detected a characteristic pattern of abnormalities, quite different from the aspects observed in liver cirrhosis (Homeida et al. 1988a, Abdel-Wahab et al. 1989) and in acute schistosomiasis (Barata et al. 1999, Lambertucci et al. 1994, 1997). The most important finding was echogenic thickening of the walls of the portal vein and its branches. Field studies in endemic areas have shown that the sum of total thickening of three peripheral branches of the portal vein, thickening of gall-bladder wall, enlargement of the left lobe of the liver, and thickening of the portal vein in its bifurcation are the best variables for ultrasonographic diagnosis of schistosomiasis mansoni (Gerspacher-Lara 1999). Magnetic resonance imaging (MRI) has been described in four cases of hepatosplenic schistosomiasis mansoni (Patel et al. 1993, Willemsen et al. 1995, Lambertucci et al. 2002, 2004). The first two studies used US, computed tomography (CT) and MRI in the evaluation of a patient with hepatosplenic schistosomiasis mansoni. The findings of the different methods were in agreement in both studies. Periportal echogenic thickening on US, suggestive of fibrosis, and low attenuation bands about the portal vessels, which markedly enhanced with contrast CT were described. MRI demonstrated the same periportal bands that were seen on liver US and CT scans. These bands showed hiperintense signal on T2-weighted sequences, and were isointense in T1-weighted sequences, with enhancement after contrast administration. The studies of Lambertucci et al. (2002, 2004) evaluated patients with advanced forms of hepatosplenic schistosomiasis by US and MRI. Both methods were again in agreement with respect to the presence of intense periportal fibrosis. Once more, MRI demonstrated broad periportal bands hypointense to the liver on T1-weighted sequences, while they had increased signal on T2-weighted images. Thickening of the gallbladder wall, enlargement of spleen, splenic and portal veins and collateral vessels were detected. After contrast administration, T1-weighted images revealed enhancement of the gallbladder wall and periportal space. We describe the case of a man in whom the results of US and MRI were not in agreement with respect to the identification of periportal fibrosis. PATIENTS AND METHODS A 59-year-old man was referred to the Hospital of the Federal University of Minas Gerais, in Brazil, for the evaluation of schistosomal periportal fibrosis, suggested by an abdominal US performed elsewhere. He was a resident of Belo Horizonte, a city where schistosomiasis is not endemic, but informed previous contact with stream waters in areas were transmission of the disease is known to occur. Examination of nine stool samples did not disclose eggs of Schistosoma mansoni, and no eggs or granulomas were detected by a rectal biopsy. The patient denied previous episodes of digestive bleeding, ascitis or jaundice, as well as chronic prescribed drugs use or alcohol abuse. His clinical examination revealed no abnormalities: liver and spleen were non palpable, and no signs of portal hypertension of hepatic dysfunction were found. Blood counts also revealed no alterations: 6.28 x 106 red cells/mm3, hemoglobin 16.7 g/dl, 149 x 103 platelets/mm3, 6.1 x 103 white cells/mm3. Serological investigation for hepatitis B and C were negative and blood chemistry and coagulation were unremarkable (albumin 4.5 g/dl, ASAT 29 g/dl, ALAT 39 g/dl, GGT 31 g/dl). A new US examination of the abdomen was performed using real-time ALOKA SSD 1700 device (Japan) with electronic linear 3.5 MHz transducers. Additional imaging was obtained using a GE 1.5 T Sigma unit (General Eletric, New Jersey, US). Axial and coronal 5 mm slice thickness images were performed in T1 and T2-weighted sequences, before and after contrast administration. RESULTS US of the abdomen showed enlarged central periportal bands with increased echogenicity, suggesting intense central fibrosis (Fig. 1). Echogenic thickening of the gallbladder wall was also detected (Fig. 2). The image pattern was characteristic of hepatic fibrosis produced by S. mansoni. No evidence of portal hypertension, such as portal vein or spleen enlargement and collateral veins, was noticed. MRI demonstrated broad central periportal bands hypointense to the liver on T1-weighted sequences, and with increased signal on T2-weighted images. However, after suppression of fat tissue signal, these periportal bands disappeared (Fig. 3). This finding shows that US periportal thickening suggestive of schistosomal fibrosis corresponded in fact to adipose tissue. Like US, MRI did not detect any evidence of portal hypertension. DISCUSSION MRI was decisive to put away the diagnosis of schistosomal periportal fibrosis suggested by US in the patient described above. All clinical and laboratory aspects of the case reported suggested absence of schistosomiasis, and there were no evidences of the hepatosplenic form of the disease. However, US images in this patient showed solid evidence of schistosomal periportal fibrosis, since characteristic periportal thickening was observed. The hypothesis of schistosomiasis was then made, since periportal fibrosis can occur without enlarged liver or spleen, or without portal hypertension. Surprisingly MRI revealed that periportal signal alteration corresponded to adipose tissue which entered the liver surrounding the portal vein. Up to 20 years ago, field studies would distinguish hepatosplenic schistosomiasis from other chronic forms of the disease by detecting a palpable spleen on physical examination (Kloetzel 1962, Barreto et al. 1985, Lambertucci & Barravieira 1994, Prata 2002). Liver and spleen enlargement in a person eliminating S. mansoni eggs in stool was indicative of Symmers fibrosis in both epidemiological studies and in those involving hospitalized patients. In the last two decades, studies comparing spleen palpation with more accurate methods for detecting spleen enlargement, such as ultrasound, have shown serious limitations on abdominal physical examination (Sullivan & Williams 1976, Barkun et al. 1991). These studies have established that some spleens of normal size are palpable, and have confirmed that many enlarged spleens are non palpable. Studies comparing abdominal physical examination with US have established that spleen palpation is not precise for the diagnosis of spleen enlargement and for the identification of severe cases in endemic areas of schistosomiasis (Homeida et al. 1988b, Abdel-Wahab et al. 1992, Lambertucci et al. 1996, Gerspacher-Lara et al. 1998). Lambertucci et al. (2001) have studied 741 subjects with schistosomiasis in an endemic area of Minas Gerais. US examination identified 15 patients (2%) with intense periportal thickening without spleen enlargement, showing that intense periportal fibrosis can occur without splenomegaly, and that subjects with severe forms of the disease could have not been included in previous studies evaluating morbidity. Symmers fibrosis in patients without spleen enlargement has also been described previously by one US study in Africa (Homeida et al. 1988b) and by one autopsy study in Brazil (Prata & Andrade 1963). These are examples of how new techniques allow us to better access and comprehend the morbidity in schistosomiasis (Barbosa et al. 1996). MRI has been established as a very sensitive image method in various diseases and, different from US, is not a dynamic study and can be less examiner-dependent. Disagreement between US and MRI (in favor of the second) in the identification of schistosomal periportal fibrosis was found in this case. Studies of series of cases are necessary to compare these image methods and to define the role of MRI in the diagnosis and evaluation of morbidity in schistosomiasis mansoni. REFEREENCES
The following images related to this document are available:Photo images[oc06201f3.jpg] [oc06201f1.jpg] [oc06201f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}