 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memórias do Instituto Oswaldo Cruz, Vol. 102, No.1, February 2007, pp. 29-33 Slime production and antibiotic susceptibility in staphylococci isolated from clinical samples Seza Arslan+, Fatma Özkarde Department of Biology,
Faculty of Arts and Sciences, Abant Izzet Baysal University, 14280, Gölköy/Bolu,
Turkey Received 29 May
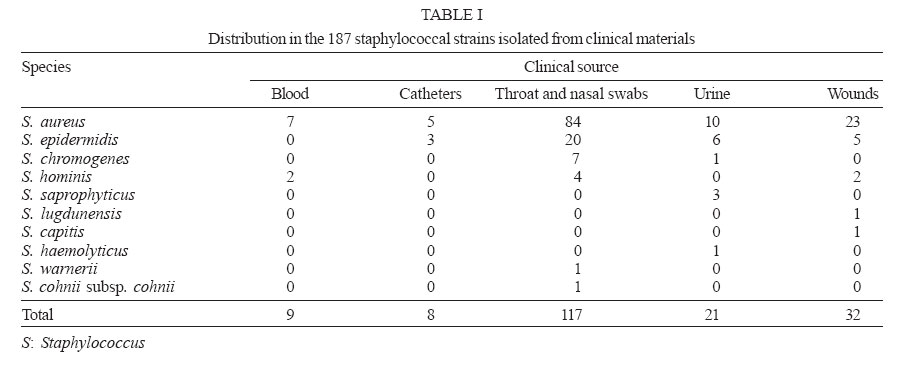
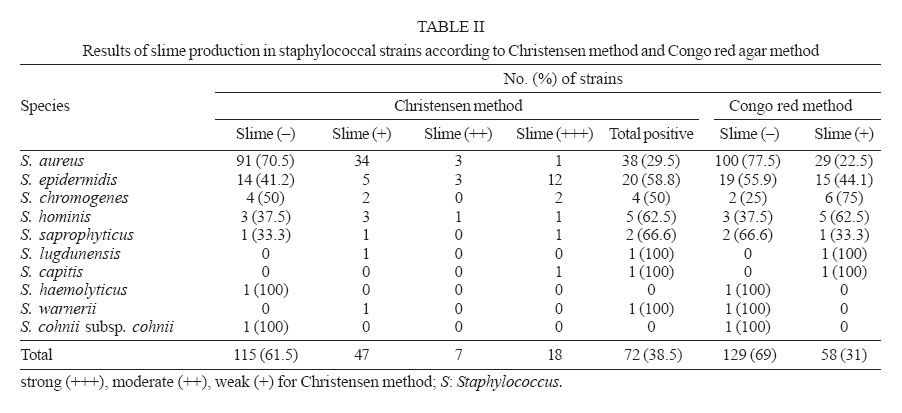
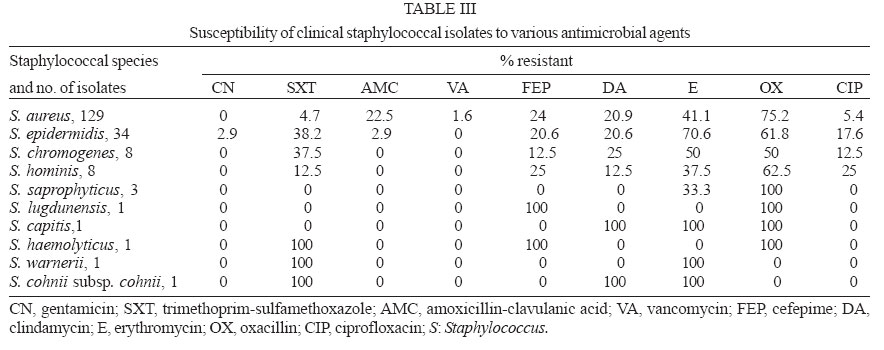
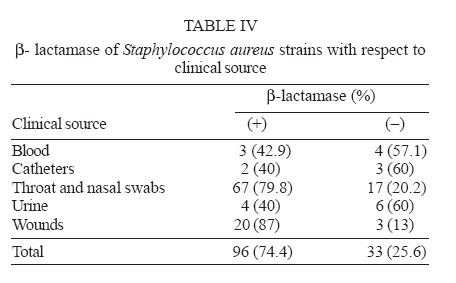
2006 Code Number: oc07004 A total of 187 isolates from several clinical specimens were identified to species level as 129 Staphylococcus aureus strains and 58 coagulase-negative staphylococci (CNS) strains by the API Staph System (Biomerieux). Slime production was detected both by the conventional Christensen's method as well as by the Congo red agar method. Seventy-two strains of staphylococci isolates (38.5%) were found to be slime producers by Christensen's test tube method whereas 58 strains (31%) were slime positive with Congo red agar method. There was no statistically significant difference between the two methods for the detection of slime production (P > 0.05). Susceptibility of isolates against antimicrobial agents was tested by the disk diffusion method. Staphylococcal species had resistance to one or more antibiotics. Among the various antimicrobial agents, oxacillin (71.1%) and erythromycin (47.1%) showed higher resistance than most of the agents used against all isolates. Oxacillin resistant S. aureus (ORSA) and oxacillin resistant coagulase-negative staphylococci (ORCNS), 97 (75.2%) and 36 (62.1%) respectively were frequently observed in strains isolated from clinical materials. Among the ORSA strains, two strains were resistant to vancomycin. Moreover, 96 (74.4%) of 129 S. aureus strains were positive for β-lactamase enzyme. However, 78 (81.25%) of 96 β-lactamase positive S. aureus strains were β-lactamase positive ORSA isolates, but none of them had vancomycin resistance. Key words: Staphylococcus sp. - slime - antimicrobial susceptibility - β-lactamase - clinical isolates Slime production is considered to be a significant virulence factor for some strains of staphylococci (Christensen et al. 1982, Davenport et al. 1986, Kleeman et al. 1993, Ammendolia et al. 1999, Mack et al. 2000). In coagulase-negative staphylococci (CNS), a loosely bound exopolysaccharides layer (slime) has been found in addition to capsule, and it has been associated with sepsis, including intravenous-catheter-related bacteremia and other prosthetic device infections (Ishak et al. 1985, Diaz-Mitoma et al. 1987, Etienne et al. 1988, Rupp & Archer 1994). Similarly, Staphylococcus aureus strains have bacterial capsules, which are closely associated with the bacterial cell wall. These strains may also have an extracapsular and labile extrapolysaccharidic structure (Caputy & Costerton 1982). Formerly slime production of S. aureus has never been considered as a virulence factor. Recently, some investigators reported that slime-producing S. aureus strains had a higher colonization capacity than its non-slime-producing variants did. Therefore, S. aureus slime may play a role in the establishment of infection (Baselga et al. 1993, Ammendolia et al. 1999). The importance of the role played by slime is further increased by its frequent association to reduced antibiotic susceptibility (Kloos & Bannerman 1994). The difficulty in eradicating a chronic infection associated with slime formation has been reported, and slime-producing bacteria has been shown to resist higher antibiotic concentrations than non-slime-producing bacteria (Gristina et al. 1987). Moreover, detection of resistance to oxacillin in staphylococci is important to guide the therapy and prevent the patient from being unnecessarily treated with vancomycin, which is an antimicrobial agent that presents therapeutic complications, high costs, and may lead to the selection of resistant mutants (Marshall et al. 1999). In this study, we wanted to evaluate the occurrence of slime production among clinical isolates of both CNS and S. aureus by comparing different methods. To assess the relationship between slime and pathogenicity, we investigated the susceptibility to certain antimicrobial agents, particularly oxacillin. MATERIALS AND METHODS Bacterial isolates - One hundred eighty seven staphylococcal isolates, provided by hospital laboratory, were obtained from culture of several specimens; 117 isolated from throat and nasal swabs, 32 from wounds, 21 from urine, 9 from blood, and 8 from catheters. Table I shows distribution of species and clinical samples in the 187 staphylococcal strains. These staphylococcal strains, specifically 115 S. aureus strains, 34 S. epidermidis strains, eight S. chromogenes strains, eight S. hominis strains, three S. saprophyticus strains, one S. lugdunensis strain, one S. capitis strain, one S. haemolyticus strain, one S. warneri strain, one S. cohnii subsp. cohnii strain, isolated from diverse clinical sources were studied. Isolates were characterized at the species level by the API Staph system (Biomerieux, France) according to the instructions of the manufacturers. The organims were stored in Trypticase soy broth (TSB), to which 15% sterile glycerol was added, at -20°C. Slime production - Slime production of all isolates was evaluated by two different methods, Christensen method (Tube adherence) and Congo red agar method. Briefly, a loop of isolates from a blood agar plate was inoculated into a glass tube containing 5 ml of TSB and incubated at 37°C for 48 h. The contents of the tubes were removed and then stained with 0.25% safranin. An adherent film on the surface of the glass tube was taken as evidence of slime formation. The absence of a film or the mere presence of a ring at the liquid-air interface was interpreted as a negative result (-). In the study, positive results were recorded as strong (+++), moderate (++), weak (+). Each test was interpreted by two different observers (Christensen et al. 1982). In Congo red test, the medium was prepared with 37 g/l brain heart infusion broth, 50 g/l sucrose, 10 g/l agar, and 0.8 g/l Congo red. Congo red stain was prepared as a concentrated aqueous solution and autoclaved at 121°C for 15 min and separately from the other medium constituents, and was then added when the agar had cooled to 55°C. Plates were inoculated and incubated at 37°C for 24 h. A positive result was indicated by black colonies on the surface. Non-slime producing strains developed red colonies. Each plate was interpreted by two different observers (Freeman et al. 1989). Antibiotic susceptibility - Susceptibility to antibiotics was determined by the disk diffusion method on Mueller-Hinton agar plates (NCCLS 1997). Nine antibiotics were chosen for the study according to their common use in research, especially human medicine. They belonged to the following groups: penicillins (oxacillin), cephalosporins (cefepime), beta-lactamase inhibitors (amoxicillin-clavulanic acid), aminoglycosides (gentamicin), macrolides (erythromycin), quinolones (ciprofloxacin), glycopeptides (vancomycin), and miscellaneous (clindamycin and trimethoprim-sulfa-methoxazole). β-lactamase test- β-lactamase strips (Fluka, Germany) for the acidimetric detection of the β-lactamase activity of all S. aureus strains were used. The test strips were inserted into test tube with prepared bacterial suspension in saline. A positive result was indicated by the appearance of a yellow color. Negative reaction remained red color. Statistical analysis - Differences between two methods used for the detection of the slime production were evaluated by the Chi-square analysis. P values of less than 0.05 were considered significant. RESULTS Slime production was detected by Christensen method and Congo red agar method. Table II shows the results of slime production by different staphylococcal species by both methods in details. In Christensen method, slime production was found in 72 (38.5%) of 187 staphylococcal isolates whereas 115 (61.5%) strains of staphylococcal isolates were not slime producers. All staphylococcal species isolated from clinical samples had one or more of slime producer strains according to tube adherence test, except S. haemolyticus and S. cohnii subsp. cohnii. Fifty eight (31%) of staphylococcal strains were slime positive and 129 (69%) strains were slime negative by Congo red agar method. In this test, species of S. haemolyticus, S. warnerii, and S. cohnii subsp. cohnii had no any slime producer strains. Positive cases in the tube adherence test in staphylococcal isolates were more frequently observed in the Christensen's method than in the Congo red agar method, but there was no statistically significant difference between two methods used for detection of the slime production (P > 0.05). Table III shows the correlation between the results of antibiotic susceptibility assays for detection of antibiotic resistance and distribution among them staphylococci. Resistance to antibacterial agents has increased among many species of bacterial pathogens. All the isolates were susceptible to gentamicin and vancomycin, except for two strains of S. aureus and one strain of S. epidermidis. Among the various antimicrobial agents, oxacillin (71.1%) and erythromycin (47.1%) had higher resistance than most of the agents used against all isolates. Oxacillin resistant S. aureus (ORSA) and oxacillin resistant coagulase-negative staphylococci (ORCNS), 97 (75.2%) and 36 (62.1%) respectively were frequently observed in strains isolated from clinical materials. Among the ORSA strains, two strains were resistant to vancomycin. β-lactamase was produced by 96 (74.4%) of 129 S. aureus strains with statistically significant difference among the strains from each clinical source (P < 0.05). β-lactamase positive strains and their clinical sources are shown in Table IV. However, 78 (81.25%) of 96 ORSA strains were b-lactamase positive ORSA isolates, but none of them had vancomycin resistant. DISCUSSION In recent years, the most common infectious agents have been Staphylococcus sp. They are frequently isolated from clinical specimens, where they may be only a contaminant or the cause of infections. S. aureus is known as a major pathogen, especially in nosocomial infections (Tenover & Gaynes 2000, Kluytmans & Wertheim 2005). Coagulase-negative staphylococci (CNS) are a group of microorganisms that are increasingly implicated as a cause of significant infection (Gemmel 1986, Khatib et al. 1995, Fux et al. 2005). In this study, we isolated several staphylococcal strains from different clinical samples. The staphylococcal clinical species most commonly isolated were S. aureus, S. epidermidis, and S. hominis, a distribution similar to those found by other authors (Ammendolia et al. 1999, Urdez-Hernandez et al. 1999). S. lugdunensis, S. capitis, S. warnerii, and S. cohnii subsp. cohnii were less frequent although these strains have also been isolated from several clinical specimens (Kleeman et al. 1993, Urdez-Hernandez et al. 1999). S. epidermidis was the most prevalent species isolated among clinical strains of CNS. This finding confirms that of a recent study (Ammendolia et al. 1999). On the other hand, slime production plays an important role in the pathogenesis of infections caused by different microorganisms, especially staphylococci. Except for S. haemolyticus and S. cohnii subsp. cohnii, slime production was by both methods in all staphylococci species (Table II). The data reported here indicate an important role of slime production as a virulence marker for clinically significant S. epidermidis isolates. Its occurrence among a majority of clinical CNS isolates and its association with the strains' ability to produce thicker biofilms may suggest a role of slime in pathogenesis (Table II). The results are similar to those reported by other authors (Ishak et al. 1985, Muller et al. 1993, Rupp & Archer1994, Ammendolia et al. 1999), who found that S. epidermidis frequently causes nosocomial septicemia, and infects indwelling medical devices like intravascular catheters and prosthetic valves. However, the findings of the present study showed that slime formation was not more prominent in S. aureus strains isolated from various clinical samples than in clinical CNS strains isolated (Table II). Among the resistant pathogens, methicillin-(oxacillin) resistant S. aureus (MRSA) is one of the most important causes of nosocomial infections worldwide and can cause outbreaks that are difficult to control (Boyce 1990, Gold & Moellering 1996, Salmenlinna 2002). Hsueh et al. (2004) reported that a rapid emergence of nosocomical methicillin-resistant S. aureus infection from 26.3% in 1986 to 77% in 2001 was found at a hospital. According to our results, S. aureus strains isolated from clinical materials showed the highest resistance to antibiotic oxacillin in all antimicrobials. Of the 129 S. aureus isolates, 97 isolates (75.2%) was ORSA strains. In general, multidrug resistance (resistance to three or more antibiotics) was observed in S. aureus clinical strains against antimicrobial agents (Table III). CNS tend to be more resistant to antimicrobial agents than S. aureus, especially to methicillin (Hussain et al. 2000). Currently, more than 70% of the CNS isolates worldwide are resistant to methicillin or oxacillin. In addition, those CNS strains acquired in hospitals have become resistant to various other antimicrobial agents (Diekema et al. 2001). In the present study, we found that CNS clinical isolates were resistant to oxacillin in 62.1%. Surprisingly CNS had somewhat high resistance against erythromycin (60.3%). However, resistance of CNS to other antimicrobial agents tested were frequently observed (Table III). In addition, all clinical staphylococcal S. aureus strains were tested for β-lactamase production. β-lactamase was produced by 96 (74.4%) of 129 S. aureus strains with statistically significant difference among the strains from each clinical source (P < 0.05). The results are shown in Table IV. However, 78 (81.25%) of 96 β-lactamase positive S. aureus strains were β-lactamase positive ORSA isolates, but none of them had vancomycin resistance. Some authors reported that clinical infections of both community and nosocomial origins caused by ORSA strains continue to be major therapeutic and infection control challenges (Sorrell et al. 1982, Hackbarth & Chambers 1989). Recently, the vast majority of ORSA have been shown to produce β-lactamases (Massanari et al. 1988, Montanari et al. 1990), and vancomycin has been generally thought to be the agent of choice for invasive ORSA infections (Sorrell et al. 1982). Our results are consistent with data obtained from previous studies. In conclusion, we found that clinical CNS isolates had a high frequency of slime production and drug resistance, particularly S. epidermidis strains. Also, all staphylococcal strains isolated from clinical samples showed resistance against various antimicrobial agents (one or more agents), especially human medicine used. The findings of present study may be advantageous in the appropriate use of antibiotics for the successful treatment of infections caused by staphylococci. REFERENCES
Copyright 2007 Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc07004t1.jpg] [oc07004t2.jpg] [oc07004t4.jpg] [oc07004t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}