 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
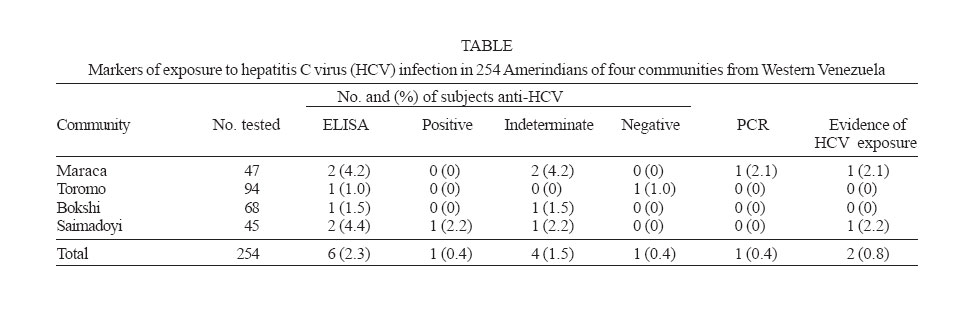
Memórias do Instituto Oswaldo Cruz, Vol. 102, No.1, February 2007, pp. 107-110 Low prevalence of hepatitis C virus infection in Amerindians from Western Venezuela Francisca Monsalve-Castillo/+, Leonor Chacín-Bonilla*, Ricardo J Atencio**, Leticia Porto Espinoza**, Luciana Costa-León**, José M Echevarría*** Cátedra
de Virología, Escuela de Bioanálisis, Av. 16, Maracaibo, Estado
Zulia, Venezuela *Post-grado de Inmunología e Instituto de
Investigaciones Clínicas **Laboratorio Regional de Referencia Virológica,
Facultad de Medicina, Universidad del Zulia, Maracaibo, Venezuela ***Centro
Nacional de Microbiología, Instituto de Salud Carlos III, Majadahonda,
Madrid, España Financial support: Consejo de Desarrollo Científico y Humanístico, Universidad del Zulia Received 29 June
2006 Code Number: oc07018 Previous studies have not found hepatitis C virus (HCV) infection in Amerindians from Western Venezuela. A survey of 254 Bari and Yukpa natives aged 10-60 years (mean ± SD age = 35 ± 5.4 years) from four communities, two Bari and two Yukpa, in this area were studied to assess the prevalence of antibodies to HCV (anti-HCV) and HCV RNA among these indigenous populations. Serum samples were examined initially for anti-HCV by a four generation enzyme-linked immunosorbent assay (ELISA). Reactive samples were then tested using a third generation recombinant immunoblot assay (RIBA-3). Viral RNA was investigated in all immunoblot-reactive samples by a nested polymerase chain reaction (PCR) method. Six (2.3%) of 254 natives were positive by ELISA, one (2.2%) of these reactive samples were positive by RIBA, and four (1.5%) were indeterminate. Only two (0.8%) were positive by PCR, corresponding to 1 (2.1%) of 47 inhabitants of a Yukpa community and to 1 (2.2%) of 45 subjects of a Bari community. Iatrogenic is thought to play a role in acquisition of the infection. The findings indicate a HCV focus of low endemicity and are compatible with a low degree of exposures of the natives to the virus. Studies are necessary to assess the risk factors for infection in these Amerindians. Key words: hepatitis C virus prevalence Amerindians - Venezuela Hepatitis C virus (HCV) infection is recognized as a public health problem worldwide. In industrialized nations, parenteral transmission is the main route for virus spreading via intravenous drug use and contaminated blood transfusions or blood products (Di Bisceglie 1998). Homosexuality and multiple heterosexual partners have been implicated in the spread of the infection (Rooney & Gilson 1998). In developing countries, the epidemiology of HCV is less understood. Although the infection has been associated to injection drug in recent years (Saha et al. 2000) there is a growing body of data that indicates that the epidemiology of HCV in these countries is highly influenced by iatrogenic transmission factors (Sanchez et al. 2000). Studies on the epidemiology of the virus in Latin America are particularly scarce, especially those conducted among population-based samples. Almost nothing is known concerning the infection in Amerindian populations. In this area low prevalence rates from 0 to 2.3% have been reported (Blitz-Dorfman. et al. 1996, De Paula et al. 2000, Aguilar et al. 2001, 2002). In Venezuela, high prevalence rates have been confined to high-risk populations, such as hemophiliacs and hemodialysis patients (Pujol et al. 1996), with very low seropositivity rates (0.7-1.1%) in urban and rural populations and in Amerindians from the Western area of the country (2.1%) (Aguilar et al. 2001). However, no evidence of infection has been found among Yukpa and Bari Indians from the Western region (Blitz-Dorfman et al. 1996). This finding contrasts with the high infection rates of hepatitis B and D viruses (HBV, HDV) in these populations (Blitz-Dorfman et al. 1996) since HCV shares with these agents the parenteral route of transmission. As these natives have increasing contact with the modern Venezuelan citizens, a study was conducted to assess the prevalence of HCV infection among Amerindians from Western Venezuela. The Baris and Yukpas live in isolated sylvatic communities in the Sierra of Perijá, Zulia State, Western Venezuela. Maraca, Toromo, Bokshi, and Saimadoyi settings were chosen for epidemiologic surveys for their representative features: geography, population size, and degree of contact with non-Amerindian citizens. The first two belong to the Yukpa ethnic and the remainder to the Bari ethnic. Maraca and Toromo are situated in a lowland area, 20 m below sea level, and Bokshi and Saimadoyi are located in a mountain region at 800 m above sea level. The average annual temperature and rainfall for both areas are 28ºC and 1400 mm and 24ºC and 2000 mm, respectively. The Yukpas and Baris continue to live in their traditional manner; they remain isolated and have adopted a sedentary lifestyle under the influence of missionaries since the 1960s. Sexual activity begins at an early age and multiple partners are common. Ritual percutaneous practices exist but intravenous drugs are not used. They exhibit little evidence of genetic admixture with non-Amerindian citizens. However, they are relatively acculturated and have contact with these citizens. Their lands grow progressively smaller as a result of the establishment of farms and cattle ranches, the exploitation of petroleum deposits in the lowlands and the presence of drug dealers and guerrilla in the frontier area with Colombia. In recent years, a group of 160 Yukpas established in Maracaibo, the capital city of Zulia State. Thus, they have increasing contact with the modern Venezuelan society. In September 2002, representative samples of 47, 94, 68, and 45 subjects were studied in Maraca, Toromo, Bokshi, and Saimadoyi, respectively. The total populations of these communities consisted of 110, 150, 130, and 334 inhabitants. Overall, 254 subjects participated in the study. They were 10-60 years old (mean ± SD age = 35 ± 5.4 years); 132 were males and 122 were females. The aim of the study was explained to the householders and their consent was obtained before enrollment in the study. The ethical aspect of the study was approved by the Consejo de Desarrollo Humanístico y Científico of the Universidad del Zulia. Participants were asked about demographic features and risk factors for HCV infection such as, intravenous drug use, sexual behaviour, health care visits, previous hospitalizations, blood transfusions, and medical injections. Ten milliliters of venous blood were obtained from each subject and the sera were separated, transported in dry ice to the laboratory, and stored a 20ºC until tested. All samples were examined initially for anti-HCV by a four generation enzyme-linked immunosorbent assay (ELISA-4) (Innotest HCV Ab IV, Innogenetics NV, Antwerp, Belgium) according to the manufacturer's instructions. Samples that showed a reading above the test's cut-off value were then tested using a third generation recombinant immunoblot assay (RIBA-3) (Inno-Lia, HCV Ab III, Innogenetics) according to the man-ufacturer's instructions. The RIBA-3 test results were interpreted positive if two or more bands were detected at an intensity ≥ 1+, indeterminate if only one band was observed, and negative if no bands were obtained. Viral ribonucleic acid was investigated in all immunoblot-reactive samples by a nested polymerase chain reaction (PCR) method (HCV-Fast, Pharmagene S.A., Madrid, Spain), according to the manufacturer's instructions. Table I shows the antibody status and PCR test results of the studied communities. Six of the 254 sera were initially reactive for anti-HCV with the ELISA-4. Of these reactive sera, one was positive, one negative, and four were indeterminate by the RIBA-3 test. The overall RIBA-3 confirmed seroprevalence of HCV infection in this population was 16.7% (1/6). Excluding the RIBA-3 indeterminate group, the predictive value of a positive HCV ELISA-4 test result and the false positive rate in this population was 50% (1/2). Investigation for the presence of HCV RNA in RIBA-3 positive and indeterminate samples revealed viral RNA only in one of the four indeterminate sera. Therefore only two positives cases were detected; one corresponded to 1 (2.1%) of the 47 Yukpas surveyed from Maraca and the other to 1 (2.2%) of the 45 Baris from Saimadoyi. The first was a 27 year-old woman with a history of blood transfusion 3 years ago and a HCV PCR positive that suggest she had an ongoing infection. The second was a 38 year old-man without history of risk factors that could be related to the acquisition of the infection. The negative PCR test in this case suggests a past resolving infection. This study is among the first in South America conducted in community-based samples and to determine carriage of HCV RNA. The results provide evidence, for the first time, of the occurrence of infection in Yukpa and Bari Amerindian populations from Western Venezuela. The prevalences of anti-HCV in Yukpas from Maraca (2.1%, 1/47), in Baris from Saimadoyi (2.2%, 1/45), and in the overall population (0.8%, 2/254) appear relatively low. These figures are similar to those reported in the general population from industrialized nations (0.5-2%) (Di Bisceglie 1998) and from South America (0-2.3%) (Blitz-Dorfman et al. 1996, De Paula et al. 2000, Aguilar et al. 2001, 2002). The prevalence rates are also similar to those previously reported from Venezuela in the general population (0.7-1.5%) and in Amerindians from the eastern area (2.1%) (Aguilar et al. 2001). HCV infection appears to be absent in two of the studied communities. The high false-reactivity with ELISA systems found by us has been reported in other studies and might result from cross-reactivity with tropical pathogens or the presence of interfering substances (Aceti et al. 1990, Tibbs et al. 1991). Malaria is highly endemic among these Amerindians (Pérez & Bracho 1993). In previous studies of Bari and Yukpa ethnics, no evidence of HCV infection was found (Blitz-Dorfman et al. 1996). It is uncertain if the virus had not penetrated these isolated populations by then or it was not detected for its low endemicity. However, the presence of anti-HCV in half of the studied settings and the low infection rates, suggest that the virus has not yet penetrated all the native villages and a low degree of exposure of these Indians to the virus. The small seropositivity rate for HCV in this study prevented statistical analysis of risk factors for infection. However, the virus was not related to intravenous drug use since it appears to be non existent among these natives, according to the questionnaires, missionaries, and leaders of the communities. Sexual intercourse with multiple partners is common among Baris and Yukpas but there is a small risk of sexual transmission of HCV (Rooney & Gilson 1998). Ritual percutaneous practices by using sharing cutting instruments occur in these populations. However, percutaneous exposure could not be associated with HDV infections in Amerindian populations, including those from eastern Venezuela. (Perez & Bracho 1993). Iatrogenic transmission might play a role in the penetration of the virus in these isolated communities. The anti-HCV PCR+ Yukpa woman had a history of blood transfusion. In Venezuela, implementation of universal donor screening for anti-HCV have also been in effect in blood banks. However, blood transfusion remains a potential current risk for HCV infection since anti-HCV screening is limited by technical and financial factors. Besides, it is possible that HCV transmission may occur in transfusion units because of faulty implementation of infection control practices, such as the sharing of medication vials and supplies (Echevarría & León 2003). In Brazil, although a significant decline of hepatitis C infection in hemodialysis patients have been noted (Carneiro 2005), blood transfusions have been correlated with the infection in these patients (Busek et al. 2002, Carneiro et al. 2005). There is a growing body of evidences that indicates that iatrogenic transmission of HCV is highly significant in developing countries (Frank et al. 2000, Sanchez et al. 2000). In Venezuela, it has been proposed that the absence of HCV infection in Baris and Yukpas until recent years was due to their margination in health care services (Blitz-Dorfman et al. 1996) and that the introduction and spread of the HDV in Yanomami Indians could be the result of a health-care programmer with iatrogenic transmission of the virus (Perez & Bracho 1993). The harmful effects of the process of acculturation on the health of Bari and Yukpa Amerindians are well documented. Recent epidemics of severe B and delta hepatitis that decimated these populations (Aguilar et al. 2002) and high endemicity of infectious agents have been reported (Chacín-Bonilla & Sanchez 2000). Likewise the presence of HCV infection in these natives may be a reflection of their cultural assimilation and increasing contact with the modern Venezuelan citizens and health care services since this virus is not considered autochthonous to South America due to the absence or low prevalence of HCV in Amerindians from this region and the distribution of genotypes (Soares et al. 1994) that are similar to those found in North America, Western Europe, an other countries of South America (De Paula et al. 2000). In conclusion, there is a HCV focus of low endemicity in Bari and Yukpa populations compatible with a low degree of exposure to the virus. However, the infected persons represent a high risk for the spread of the virus in the region and emphasize the urgent need to develop preventive measures. Further studies are needed to better assess the risk factors for infection in these Amerin-dians. This study provides new information on the epidemiology of HCV and reflects the harmful effects of the acculturation process on the health of these natives. ACKNOWLEDGMENTS To Marina Garcia, Braulio Fuenmayor, and Yackeline Fuen-mayor for their assistance in this study. REFERENCES
Copyright 2007 Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc07018t1.jpg] |
| |||||||||

{kind=link}