 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memórias do Instituto Oswaldo Cruz, Vol. 102, No. 4, 2007, pp. 497-500 Sensitivity and specificity of polymerase chain reaction in Giemsa-stained slides for diagnosis of visceral leishmaniasis in children Yvone Maia Brustoloni/+ , Rosimar Batista Lima* , Rivaldo Venâncio da Cunha**, Maria Elizabeth Dorval***, Elisa Teruya Oshiro***, Ana Lúcia Lyrio de Oliveira, Claude Pirmez* Departamento de Pediatria **Departamento de Clínica Médica ***Departamento de Patologia, Universidade Federal de Mato Grosso do Sul, Caixa Postal 102, 79080-190 Campo Grande, MS, Brasil *Laboratório de Imunopatologia, Instituto Oswaldo Cruz- Fiocruz, Rio de Janeiro, RJ, Brasil + Corresponding author: brustoloni@uol.com.br Received
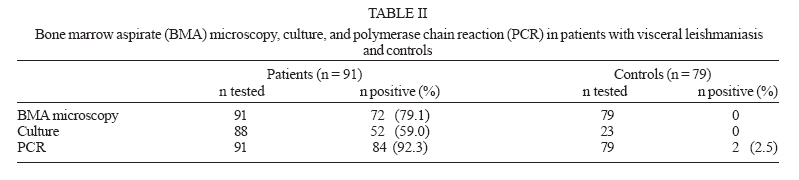
24 November 2006 Code Number: oc07078 The aim of this study was to evaluate the sensitivity and specificity of polymerase chain reaction (PCR) in the detection of Leishmania DNA in archived Giemsa-stained bone marrow slides for diagnosis of visceral leishmaniasis (VL), and to compare PCR with conventional diagnostic techniques, like direct microscopy and parasite culture. Specimens of archived Giemsa-stained bone marrow slides from 91 patients with VL and from 79 controls with other diseases or conditions were studied. PCR showed the highest sensitivity (92.3%) and had good specificity (97.5%). Direct examination detected 79.1% and culture 59% of positive samples. In addition, PCR was able to detect VL in 16 of 19 patients (84.2%) with negative microscopy. PCR in Giemsa-stained bone marrow slides is a suitable tool for confirming diagnosis in patients with VL and may be useful in the diagnosis of difficult cases. Slide smears are easily stored, do not require special storage conditions such as low temperatures, and can be easily mailed to centers where PCR is available, making it an excellent option for diagnosis in the field. Key words: visceral leishmaniasis - polymerase chain reaction - diagnosis Conventional methods for diagnosis of visceral leishmaniasis (VL), such as parasitological or serological tests, still have limitations in their use (Sundar 2003, da Silva et al. 2005). The identification of the causal agent of human leishmaniasis by these tests is difficult even in a well-equipped hospital and improved tools for this purpose are needed. Polymerase chain reaction (PCR) has now revolutionized contemporaneous etiologic diagnosis of infectious diseases. The description of species-specific kinetoplast DNA minicircles sequences (kDNA) (Kennedy 1984), with the possibility of amplification by PCR, made viable the utilization of the method for diagnosis of leishmaniasis in the early 1990s (Rodgers et al. 1990, Smyth et al. 1992). Currently, PCR techniques have been employed with a high level of accuracy by several researchers (Salotra et al. 2001, Cortes et al. 2004, De Doncker et al. 2005, Stark et al. 2006). Various biological samples have been used for diagnosis of visceral or cutaneous leishmaniasis by PCR: bone marrow (Piarroux et al. 1994, Osman et al. 1997, Cortes et al. 2004), human (Lachaud et al. 2001, Cascio et al. 2002) and canine blood (Lachaud et al. 2002a), lymph nodes (Lachaud et al. 2002b), buffy coat (Lachaud et al. 2001), canine conjunctival or dermal scrapings (Lachaud et al. 2002b), and skin or mucosal biopsies (Pirmez et al. 1999, Stark et al. 2006). Moreover, PCR has made possible the use of dried or old materials: Leishmania DNA has been extracted and amplified from blood or bone marrow aspirates spotted on filter paper (Cortes et al. 2004, da Silva et al. 2004), paraffin-embedded tissues (Lanús et al. 2005), Giemsa-stained slides (Motazedian et al. 2002), and museum specimens (Costa 1998). In Mato Grosso do Sul, Center-West region of Brazil, the Federal University Hospital (NHU-UFMS) situated in the capital Campo Grande is a reference center for diagnosis and treatment of VL, receiving patients from various cities of the state for diagnostic confirmation or exclusion. The aim of this study was to evaluate the use of PCR in VL diagnosis using archived Giemsa-stained bone marrow aspirate (BMA) slides, establishing its sensitivity and specificity, and to compare the performance of this retrospective diagnosis with direct microscopy and culture. Ninety-one children from the state of Mato Grosso do Sul, admitted for diagnosis and treatment of VL at the NHU-UFMS from January 1998 to September 2004 were studied. Diagnosis of VL was based on a suggestive clinical presentation, associated with a positive BMA direct microscopy or culture or serology by indirect immunofluorescence antibody test (IFAT) > 1:40; children with a suggestive clinical picture whose laboratorial tests were negative but who responded to a therapeutic trial with antimonials were included too. Controls consisted of 79 children or adults who had a BMA performed for diagnostic purposes and who did not have a confirmed leishmaniasis diagnosis but other diseases or conditions were detected. Table I shows the characteristics of the children with VL and of controls. BMAs were collected for occasion of admission, by sternal puncture or more rarely from the posterior iliac crest. Four Giemsa-stained slides for each patient were analyzed by direct microscopic examination with a 10X eyepiece and a 100X oil objective. More than 1000 microscopic fields were examined, when necessary; before deciding for a negative result, the entire slides were viewed. The slides were then archived at room temperature in the sectors of Parasitology or Hematology. Cultures were performed with Novy-MacNeal-Nicolle (NNN) with Schneider's insect medium, incubated at 24°C, and weekly examined by microscopy for the presence of parasites until eight weeks. IFAT, when possible, was performed with a commercial kit for the diagnosis of human leishmaniasis (Bio-Manguinhos-Fiocruz). For DNA extraction archived Giemsa-stained bone marrow slides were cleaned with tissue paper, wetted with sterile water, and scraped with a sterile scalpel. The material was added to 300 ml of sterile water, and a GenomicPrepTM Blood DNA Isolation Kit (Amersham Pharmacia Biotech) was used, according to the manufacturer's instructions, except that the final elution volume was reduced to 20 ml. The DNA target for PCR amplification was the conserved region of the minicircle molecule (kinetoplastid mitochondrial DNA; kDNA), using a "hot-start" PCR technique. Briefly, each reaction contained 5 ml of 10X buffer (Promega), 100 ng of 5' and 3' oligonucleotide primers (primer A: 5'-(G/C)(G/C)(C/G)CC(A/C) CTAT(A/T)TTACACCCACCCC-3'; primer B: 5'-GGGGTAGGGGCGTTCTGCGAA-3'), 200 mM of each deoxynucleoside triphosphate (Promega), 1.5-mM MgCl2, 2.5 U of Taq polymerase (Perkin Elmer), sterile water, and 2 ml of the DNA sample. PCR was performed in a total reaction volume of 50 ml, under the following conditions: a first heating step of 4 min at 94°C, followed by 30 cycles of 30 s, each consisting of denaturation at 94°C, annealing at 50°C, and extension at 72°C, with a final elongation at 72°C for 10 min. A negative control without DNA in the mixture and a positive control containing 80fg of Leishmania DNA were included in each experiment. Ten microliters of the amplified products were analyzed by electrophoresis in a 2% agarose gel stained with ethidium bromide (0.5 mg/ml) and visualized under UV. A 50-bp or 100-bp DNA ladder (Promega) was used as a marker. Samples were considered as positive when a PCR of 120 bp could be detected. PCR and direct microscopy were performed in all patients with VL and controls. Cultures were obtained in 88 children with VL and were just performed for those controls with splenomegaly, bacterial infections, normal bone marrow, or other conditions (n = 23), but not for those who had a confirmed diagnosis of hematological disease. Serology was possible to be obtained in 58 children with VL. For the 91 patients, diagnosis was based on positive direct examination (n = 72), culture (n = 5), serology (n = 7) or response to therapy with antimonies (n = 7). The study was conducted upon approval by the Ethics Committee of the Federal University of Mato Grosso do Sul and was in agreement with the regulations of the Brazilian Ministry of Health. Table II describes the results of the diagnostic methods employed. Among the 91 children with a diagnosis of VL, PCR was positive in 84, yielding a sensitivity of 92.3% (84.3-96.6, 95% CI). PCR specificity was 97.5% (90.3-99.6, 95% CI), since two out of the 79 patients with other diseases, in the control group, were positive to VL. Positive and negative predictive values were 97.7% (91.1-99.6, 95% CI) and 91.7% (83.0-96.3, 95% CI), respectively. The present experiment suggests that it is possible to reach a retrospective diagnosis of visceral leishmaniasis from stored Giemsa-stained bone marrow slides. PCR allowed the retrieval of archival cases, since the test showed a high sensitivity and specificity. The inclusion of patients in the absence of a gold-standard diagnosis may have important consequences when the sensitivity of a method is being evaluated. Analyzing only those children with a positive parasitological test (direct examination or culture: n = 77), PCR was positive in 73, thus increasing its sensitivity to 94.8% (86.5-98.3, 95% CI). Considering that we used dried, old materials for the extraction of DNA, some of them archived for as long as six years, the sensitivity achieved was highly satisfactory. The good performance of the assay was reflected too in its ability to detect DNA of the parasite in 16 of 19 patients (84.2%) for whom direct microscopy was negative. Moreover, in the seven patients whose diagnoses were based only on clinical criteria and a favorable response to antimony (with no positive parasitological or serological proof), PCR was positive in four (57%), showing that the method may be helpful in the diagnosis of difficult cases. Negative PCR results have been reported in a few patients with positive parasitological proof (Piarroux et al. 1994, Cortes et al. 2004). Similarly, four of our patients with a positive microscopic examination had a negative PCR, which can be explained by the fact that we used slides that had been stored for many years, and DNA in these smears may have suffered some damage. In the control group we included a great number of patients whose differential diagnosis with VL is frequently required; PCR was positive in two patients without VL. The possibility of asymptomatic carriers has been suggested in such situations (Salotra et al. 2001). Although the occurrence of false positives because of contamination is unlikely, it cannot be ruled out too. DNA extraction and amplification of Leishmania by PCR in Giemsa-stained slides archived for up to four years was attempted with success for the diagnosis of cutaneous leishmaniasis (Motazedian et al. 2002), showing the feasibility of establishing a new strategy for studying archived materials. Similarly to specimens collected on filter paper, slides can be easily stored, do not require low-temperature facilities for conservation, and can be easily mailed to reference centers for diagnostic confirmation or exclusion. The possibility of elucidating cases of VL for which no previous diagnostic proof is available is an encouraging step towards the inclusion of PCR in the current diagnosis of the disease. REFERENCES
Copyright 2007 Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc07078t1.jpg] [oc07078f1.jpg] [oc07078t2.jpg] |
| |||||||||

{kind=link}
{kind=link}