 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memórias do Instituto Oswaldo Cruz, Vol. 102, No. 4, 2007, pp. 501-508 Abnormal humoral immune response to influenza vaccination in pediatric type-1 human immunodeficiency virus infected patients receiving highly active antiretroviral therapy Carlos J Montoya/+, Maria F Toro*, Carlos Aguirre**, Alberto Bustamante**, Mariluz Hernandez**, Liliana P Arango***, Marta Echeverry**, Ana E Arango*, Maria C Prada**, Herminia del P Alarcon**, Mauricio Rojas*** Group of Immunovirology-Biogenesis *Department of Microbiology and Parasitology **Department of Pediatrics ***Flow Cytometry Unit Escuela de Medicina, Universidad de Antioquia, Medellin, Colombia Financial support: Aventis Pasteur Laboratories, Colombia, the Committee for the Development of Investigation (CODI), Universudad de Antioquia, Medellin +Corresponding author: cjmonto@une.net.co Received
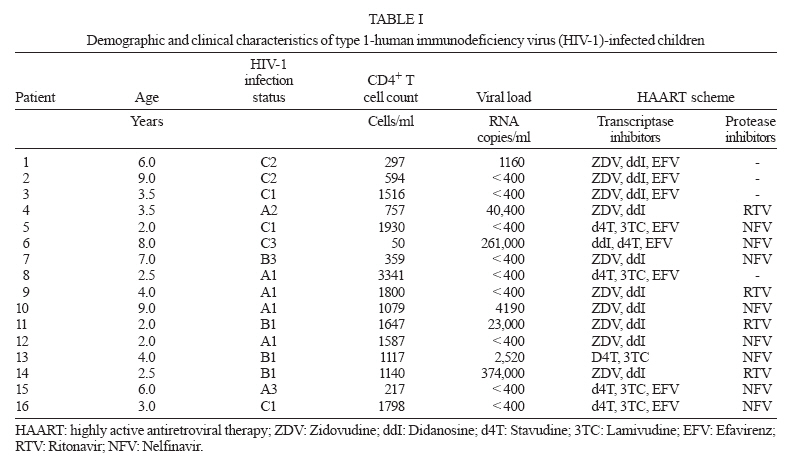
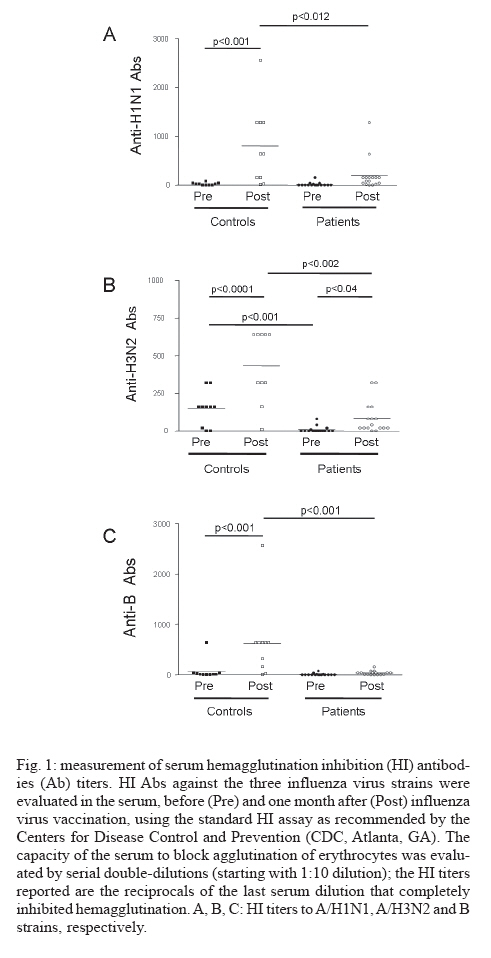
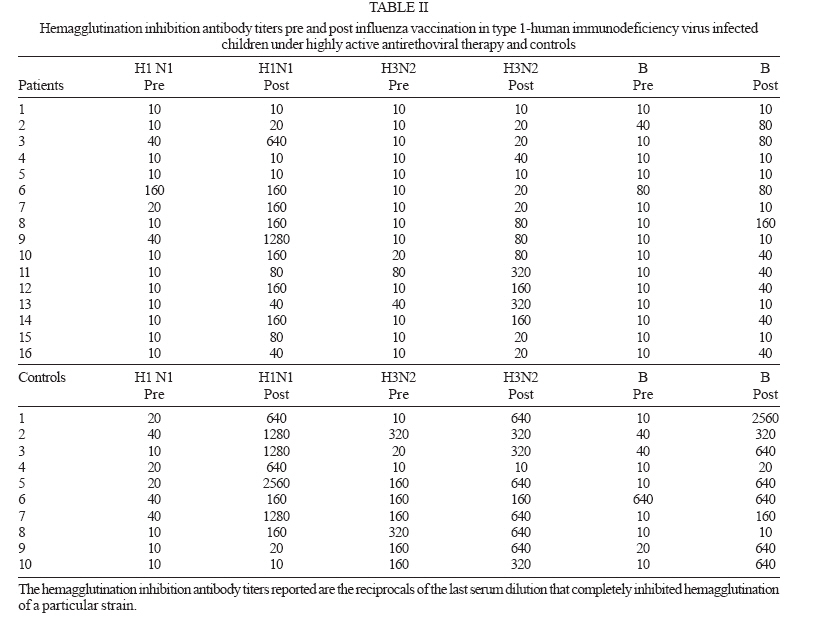
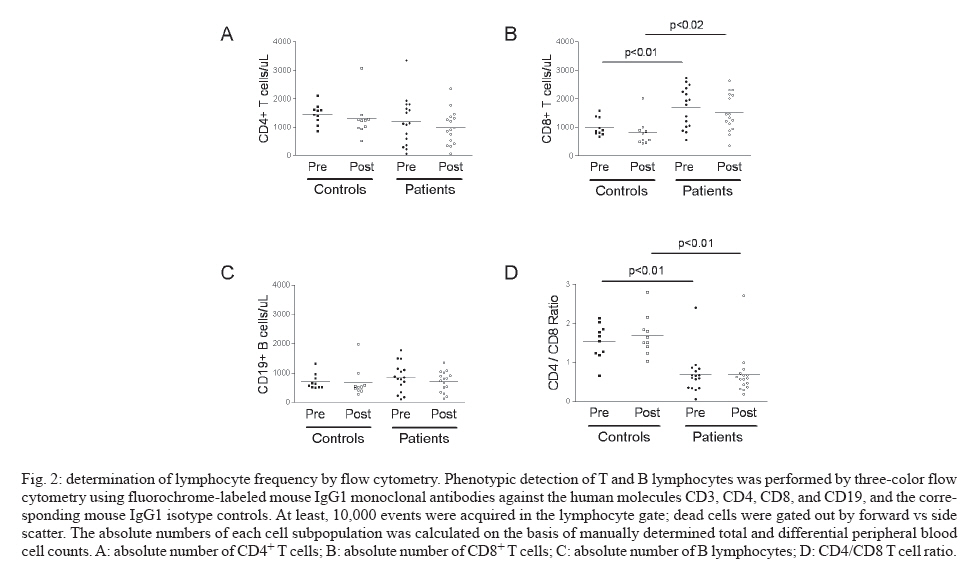
29 November 2006 Code Number: oc07079 Given that highly active antiretroviral therapy (HAART) has been demonstrated useful to restore immune competence in type-1 human immunodeficiency virus (HIV-1)-infected subjects, we evaluated the specific antibody response to influenza vaccine in a cohort of HIV-1-infected children on HAART so as to analyze the quality of this immune response in patients under antiretroviral therapy. Sixteen HIV-1-infected children and 10 HIV-1 seronegative controls were immunized with a commercially available trivalent inactivated influenza vaccine containing the strains A/H1N1, A/H3N2, and B. Serum hemagglutinin inhibition (HI) antibody titers were determined for the three viral strains at the time of vaccination and 1 month later. Immunization induced a significantly increased humoral response against the three influenza virus strains in controls, and only against A/H3N2 in HIV-1-infected children. The comparison of post-vaccination HI titers between HIV-1+ patients and HIV-1 negative controls showed significantly higher HI titers against the three strains in controls. In addition, post vaccination protective HI titers (defined as equal to or higher than 1:40) against the strains A/H3N2 and B were observed in a lower proportion of HIV-1+ children than in controls, while a similar proportion of individuals from each group achieved protective HI titers against the A/H1N1 strain. The CD4+ T cell count, CD4/CD8 T cells ratio, and serum viral load were not affected by influenza virus vaccination when pre- vs post-vaccination values were compared. These findings suggest that despite the fact that HAART is efficient in controlling HIV-1 replication and in increasing CD4+ T cell count in HIV-1-infected children, restoration of immune competence and response to cognate antigens remain incomplete, indicating that additional therapeutic strategies are required to achieve a full reconstitution of immune functions. Key words: pediatric type-1 human immunodeficiency virus infection - congenital cardiopathy - influenza vaccine - anti-influenza antibodies - hemagglutination inhibition titers Currently, infection by type-1 human immunodeficiency virus (HIV-1) is among the most important public health problems worldwide: at the end of 2005, there were more than 40 million people infected (of which 2.3 million were children below 15 years), and during this year almost 5 million new cases were diagnosed and 3.1 million HIV-1-infected individuals died (0.57 million deaths among children) as a consequence of HIV-1-derived clinical complications (UNAIDS & WHO 2005). HIV-1 infection is characterized by progressive loss of CD4+ T cells associated with other quantitative and qualitative alterations of the immune response (Letvin & Walker 2003). The dysregulation of the immune response appears early during HIV-1 infection when individuals gradually lose their T lymphocytic-proliferative responses to recall antigens, alloantigens and mitogens, before severe reduction in CD4 T-cell count appears. In addition, HIV-1 replication may impair immune function directly through the immunosuppressive effect of viral proteins and by a state of uncontrolled immune activation that leads to immunosuppression and accelerated immune cell death. All these abnormalities result in severe immunodeficiency, which predisposes HIV-1-infected individuals to infections, malignant tumors, and autoimmune disorders (Letvin & Walker 2003). Compared to HIV-1-infected adults, survival is considerably shorter among children who acquire the virus perinatally or during infancy; factors contributing to accelerated disease progression in children are poorly understood but may include relative immunological immaturity, thymic HIV-mediated destruction, and sharing of HLA class I between mother and infant (Chakraborty 2005). The current treatment for pediatric HIV-1 infection is the highly active antiretroviral therapy (HAART), which induces a decrease in plasma HIV-1 RNA levels and increases the CD4 T-cell count leading to a decrease in the incidence of opportunistic infections and mortality (Luzuriaga & Sullivan 2002). Despite these beneficial effects of HAART, contradictory results have been reported regarding the improvement of the immunological function in HIV-1-infected individuals receiving this regimen (Valdez 2002). Beside its virological effects, HAART enhances the immunological function in vitro in patients with advanced, moderate, and early HIV-1 disease, as demonstrated by improved in vitro responses to recall antigens and polyclonal mitogenic stimuli (Valdez 2002). However, in vivo responses to immunization are heterogeneous among HAART-treated patients, even when the CD4+ T-cell counts are comparable. HAART does not normalize all the parameters of the immune system, such as CD4+ and CD8+ T cell hyper-activation; also, it is not clear if HAART leads to recovery of the CD4+ and CD8+ T-cell repertoire, and it is likely that this is a delayed and incomplete process (Lederman et al. 2003). As HAART administered during several years is unable to efficiently eliminate HIV-1 tissue reservoirs, it is unclear if this therapy leads to full recovery in vivo of the immune response, since immune reconstitution achieved during antiretroviral therapy should not only increase CD4 numbers and reduce T cell activation, but should also lead to the production of functional T cells. Influenza is an acute respiratory illness caused by infection with influenza virus, and outbreaks of the illness of variable severity occur nearly every year. Influenza results in significant morbidity in the general population and in increased mortality rates among certain high-risk patients such as those affected by chronic cardiovascular and/or pulmonary diseases and immunosuppressed individuals, such as HIV-1-infected patients (Kempe et al. 1989, Couch et al. 1997). Vaccination with inactivated influenza virus vaccine has been recommended for adult and pediatric HIV-1-infected individuals (CDC 2002). Several reports have established the quality of specific humoral immune responses against influenza virus strains after immunization of HIV-1-infected children and adults, with some controversial findings (Chadwick et al. 1994, Lyall et al. 1997, Ionita et al. 1998, Zuccotti et al. 2004, Tanzi et al. 2006). Considering that the immune reconstitution achieved by HAART has not been clearly established in pediatric HIV-1-infected patients and that influenza virus vaccine is recommended in these children, the specific antibody response that follows immunization with a commercially available inactivated influenza virus vaccine was evaluated in a cohort of HIV-1+ children receiving HAART. PATIENTS AND METHODS Study population - The study involved 16 HIV-1-infected children (15 infected by mother-to-child transmission, and a patient with HIV-1 infection of unknown origin) periodically evaluated in the Outpatient Pediatric Infectious Diseases Service of the Hospital San Vicente de Paul, Medellin, Colombia. All these patients received HAART since their HIV infection was diagnosed (see demographic and clinic information, Table I). Ten children with non-cyanotic congenital cardiopathy chronically evaluated in the Outpatient Pediatric Cardiology Service of the same Hospital served as controls; patients with congenital cardiopathies associated to immune response abnormalities, such as Down syndrome, were not enrolled in this investigation. The absence of HIV-1 infection was corroborated by serum ELISA tests; during the duration of this study, no infectious diseases were diagnosed and no pharmacological therapy was administered to the individuals of the HIV-1 negative control group. This study was approved by the Ethical Committees of the Hospital San Vicente de Paul and of the Medical Research Center of the University of Antioquia; the informed consent was obtained from the parents of each child enrolled in this investigation. Influenza virus vaccination is recommended in children affected by HIV-1 infection or congenital cardiopathies (CDC 2002). Influenza virus vaccination - All the children studied were vaccinated with a commercially available inactivated influenza virus vaccine kindly donated by Pasteur Merieux, Colombia (Imovax Gripe®). This trivalent vaccine included the formaldehyde-inactivated influenza virus strains A/New Caledonia/20/99 (H1N1), A/Moscú/10/99 (H3N2), and B/Sichuan/379/99; a dose of 0.5 ml contains 15 mg of each virus strain. In children younger than 3 years old, two doses of 0.25 ml were administered, while children older than 3 years received two doses of 0.5 ml; the interval between each dose was one month. Possible adverse reactions were monitored during the first hour following vaccination and then on a continuous basis by the parents. This vaccination was well tolerated and did not produce any abnormal adverse reaction or event among the children. Determination of serum anti-influenza antibodies - Antibodies (Abs) against the three vaccine antigens were evaluated in the serum, before and one month after influenza virus vaccination, using the standard hemagglutination inhibition (HI) test as recommended by the Centers for Disease Control and Prevention (CDC, Atlanta, GA) (Fuller et al. 1999); the reagents required to perform this assay were kindly provided by the CDC. Briefly, to remove all the non-specific inhibitors of hemagglutination, the sera were previously incubated with the Vibrio cholerae enzyme RDE (Fuller et al. 1999); the capability of each serum to block agglutination of erythrocytes was then evaluated by serial double-dilutions (starting with a 1:10 dilution) incubated with the influenza virus strains A/New Caledonia/20/99 (H1N1), A/Panamá/2007/99 (H3N2), and B/Beijing/184/93 (B). The HI titers reported are the reciprocals of the last serum dilution that completely inhibited hemagglutination of a particular strain. A four-fold or greater increase from the baseline level after vaccination was considered a clinically significant humoral immune response, while an HI titer equal to or higher than 1:40 was considered a protective response (Fuller et al. 1999). Analysis of lymphocyte populations by flow cyto-metry - Peripheral blood was drawn in EDTA-containing tubes the same day as influenza virus vaccination and one month later. Phenotypic detection of T and B cells was performed by three-color flow cytometry; to stain cell surface molecules, 100 ml of anti-coagulated blood were incubated for 20 min at room temperature (RT) in the dark with fluorochrome-labeled mouse IgG1 monoclonal Abs against the human molecules CD3 (PE-Cy5, clone UCHT1), CD4 (FITC, clone 13B8.2), CD8 (PE, clone B9.11), and CD19 (PE, clone J4.119), and the corresponding mouse IgG1 isotype controls, all from Coulter Immunotech (Marseille, France). The erythrocytes were then lysed and the leukocytes fixed by incubating for 10 min at RT with 100 ml of Cal-Lyse solution (Caltag Laboratories, Burlingame, CA). For the analysis of T and B cell subpopulations, 10,000 events were acquired in the lymphocytes' gate, using a Coulter Epics flow cytometer (Epics XL, Coulter, Hialeah, Florida). Dead cells were gated out by forward vs side scatter. The absolute number of the different leukocyte subpopulations was calculated on the basis of manually-determined total and differential peripheral blood cell counts. Statistical analysis - Data from absolute HI antibody titers and the percentages of lymphocyte subsets in pre- and post-vaccination samples are presented as the mean ± standard error (SE); these data were compared between HIV-1+ and HIV-1 negative children using the Two Ways ANOVA test. To compare the mean ranges, a post-test based on Poisson´s distribution was used. These analyses were performed with the software Statgraphics Plus 2 (Statgraphics Corp., Rockville, MD), while the graphics were designed using GraphPad Prism version 4.0 (GraphPad Software Inc, San Diego, CA). On the other hand, to compare the proportion of subjects from each group who achieved a four-fold increase in the HI Ab level or a protective HI Ab level, we made a contingency table and analyzed the data by the Fisher's Exact Test using EPI-INFO. A p < 0.05 was considered significant as critical value. RESULTS To test the capacity of HIV-1-infected children on HAART to develop specific humoral immune responses, 16 pediatric HIV-1+ patients were immunized with a trivalent, inactivated influenza virus vaccine (44% female and 56% male; mean age: 4.6 ± 2.5 years, mean CD4+ T cell count 1202 ± 844 cell/ml). All patients were receiving at least three antiretroviral medications during the last year (Table I; mean time on HAART: 2.3 ± 2.2 years; mean time between diagnosis and start of HAART: 3 ± 2 months). In 56% of them (9/16; mean age: 4.3 ± 2.5 years; mean CD4+ T cell count: 1460 ± 969 cells/ml), there was controlled viral replication and all presented a viral load (VL) lower than 400 HIV-1 RNA copies/ml of plasma, while the remaining 44% (7/16; mean age: 4.8 ± 2.9 years; mean CD4+ T cell count: 870 ± 547 cells/ml) exhibited active HIV-1 replication and detectable VL in plasma despite HAART (mean VL: 191525 ± 186952 copies/ml). As control, 10 patients with congenital cardiopathy were evaluated (50% female and 50% male; mean age: 6.5 ± 2.1 years; mean CD4+ T cell count 1454 ± 351 cell/ml), who were otherwise healthy. Vaccination was well tolerated with only a few mild, transient symptoms. Specific anti-influenza humoral immune response - Serum HI Ab titers were determined for the three influenza virus strains at the time of vaccination and 1 month later (Fig. 1). When the pre-vaccination HI titers were analyzed, both HIV-1+ patients as well as controls exhibited very low levels of HI Ab titers, except for anti-A/H3N2 HI Abs which were significantly higher in controls than in patients (146 ± 37 vs 9 ± 5, respectively; p < 0.001). In response to vaccination, significantly higher HI titers against the three viral strains were observed in the sera of controls (anti-A/H1N1: pre-vaccination 22 ± 8 vs post-vaccination 803 ± 256, p < 0.001; anti-A/H3N2: 146 ± 37 vs 433 ± 75, p < 0.001; anti-B: 77 ± 63 vs 626 ± 231, p < 0.001). In HIV-1+ children this immunization significantly increased the HI titers only for the A/H3N2 strain (9 ± 5 vs 85 ± 26, p < 0.04), but neither for the A/H1N1 (16 ± 10 vs 197 ± 82, p > 0.05) nor the B (9 ± 5 vs 37 ± 10, p > 0.05) strains. When post-vaccination HI Ab titers in both groups were compared, the controls exhibited significantly higher titers for the three strains than HIV-1-infected children (anti-A/H1N1: 803 ± 256 vs 197 ± 82, p < 0.012; anti-A/H3N2: 433 ± 75 vs 85 ± 26, p < 0.002; anti-B: 626 ± 231 vs 37 ± 10, p < 0.001; Fig. 1). Four-fold increase and protective HI titers after influenza virus vaccination - The specific immune response after influenza virus vaccine was also determined in terms of the proportion of individuals from each group (HIV-1+ patients and controls) that achieved a clinically significant humoral immune response in HI Ab titers for each viral strain (parameter defined as a four-fold increase in the HI Ab level), and the proportion that exhibited protective Ab levels against each strain (parameter defined as an HI Ab titer after vaccination equal to or higher than 1:40, considering only those individuals without protective pre-vaccination HI titers). As observed in Table II, a similar proportion of HIV-1+ children and controls exhibited a four-fold increase in HI titers against the A/H1N1 and A/H3N2 strains: 11/16 vs 7/10 (69 vs 70%) and 8/16 vs 5/10 (50 vs 50%), respectively. In addition, there was no significant difference between the proportion of HIV-1+ children and controls that achieved a four-fold increase in HI titers against influenza virus strain B: 7/16 vs 7/10 (44 vs 70%), respectively (p = 0.1842). Regarding the protective HI Ab titers, controls exhibited a higher proportion of individuals with pre-vaccination protective HI titers than HIV-1+ children (Table II): against A/H1N1: 3/10 vs 3/16 (30 vs 19%); A/H3N2: 7/10 vs 2/16 (70 vs 13%); B: 3/10 vs 2/16 (30 vs 13%). When individuals without protective pre-vaccination HI titers were considered, the proportion of individuals with post-vaccination protective HI titers against the A/H1N1 strain was comparable in HIV-1+ patients and controls: 9/13 vs 5/7 (69 vs 71%), respectively (Table II); regarding the A/H3N2 and B influenza virus strains, there were no significant differences between the proportions of HIV-1+ patients and controls that achieved protective Ab levels: 6/14 vs 2/3 (43 vs 67%, p = 0.4529) and 7/14 vs 5/7 (50 vs 71%, p = 0.3235), respectively. The influenza virus specific humoral immune response in HIV-1+ children was compared regarding their serum VL (lower or higher than 400 copies/ml). Patients with controlled viral replication (VL < 400 copies/ml, n = 9) as well as patients with uncontrolled replication (VL > 400 copies/ml, n = 7) exhibited similar HI Ab titers pre- and post-vaccination against the three influenza virus strains. Moreover, both groups of HIV-1+ patients (with or without controlled VL) exhibited a similar proportion of individuals that, in response to vaccination, achieved a four-fold increase in HI titers and protective HI levels against the viral strains studied (data not shown). These findings indicate that the deficient humoral immune response to influenza virus vaccine observed in these HIV-1+ patients was not associated to the level of viral replication control achieved with HAART. Lymphocyte subpopulation and VL behaviour in relation to vaccination - The number of CD4+ and CD8+ T cells and B lymphocytes in the peripheral blood was determined by flow cytometry. As shown in Figs 2A, C, the number of pre-vaccination CD4+ T cells and B lymphocytes was similar in HIV-1+ children and controls (1202 ± 211 vs 1454 ± 111, and 844 ± 122 vs 700 ± 83, respectively), while there was a significantly higher pre-vaccination number of CD8+ T cells in HIV-1+ children (1700 ± 177 vs 1004 ± 99, respectively; p < 0.01; Fig. 2B). The same pattern of lymphocyte subpopulations was observed one month after vaccination, with no significant differences between pre- and post-vaccination peripheral blood count of CD4+ and CD8+ T cells and B lymphocytes in patients or controls; the post-immunization counts of CD4+ T cells and B lymphocytes were similar in patients and controls (987 ± 150 vs 1291 ± 213, and 707 ± 88 vs 670 ± 157, respectively; Figs 2 A, C), and again HIV-1+ patients exhibited a significantly higher number of CD8+ T cells than controls (1517 ± 165 vs 808 ± 150, respectively; p < 0.02, Fig. 2B). The pre-vaccination CD4/CD8 T cell ratio was significantly lower in HIV-1+ children than in controls (0.7 ± 0.1 vs 1.5 ± 0.1, respectively; p < 0.01; Fig. 2D); the same difference was observed after vaccination (0.7 ± 0.17 vs 1.7 ± 0.2; p < 0.01; Fig. 2D). However, no significant variation in this ratio was observed when comparing pre- vs post-vaccination values in patients or in controls. Additionally, when pre- and post-vaccination data were compared, no significant differences in the peripheral blood count of leukocytes, lymphocytes and total CD3+ cells in patients or controls were detected (data not shown). On the other hand, the serum VL in HIV-1+ children was not significantly increased by the stimulation induced by influenza virus vaccination; rather, there was a non-significant decrease in the mean value of VL one month after vaccination (VL pre-vaccination: 109614 ± 167070 vs VL post-vaccination: 47275 ± vs 112333). In HIV-1+ children no correlation was detected between the HI Ab titers and either the CD4+ T cell count, the CD4/CD8 ratio or the serum VL (data not shown). DISCUSSION ACKNOWLEDGEMENTS To the collaboration of the Hospital San Vicente de Paul, Medellin, Colombia, to the Centers for Disease Control and Prevention, Atlanta, GA REFERENCES Copyright 2007 Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc07079t2.jpg] [oc07079f2.jpg] [oc07079f1.jpg] [oc07079t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}