 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memórias do Instituto Oswaldo Cruz, Vol. 102, No. 6, 2007, pp. 773-775 Recognition of the epidemiological significance of Neisseria meningitidis capsular serogroup W135 in the Rio de Janeiro region, Brazil David E Barroso/+, Maria C Rebelo* Laboratório de Enterovírus, Grupo de Doenças Virais, Rickettsioses e Febres Hemorrágicas, Instituto Oswaldo Cruz-Fiocruz, Av. Brasil 4365, 21040-900 Rio de Janeiro, RJ, Brasil *Laboratório de Referência Estadual para Meningites, Instituto Estadual de Infectologia São Sebastião,
Rio
de
Janeiro,
RJ,
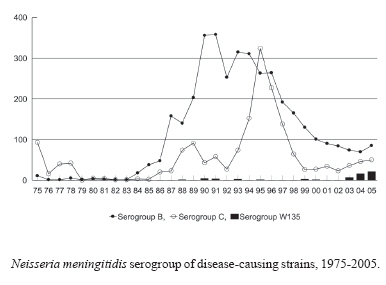
Brasil Received 13 February 2007 Accepted 4 September 2007 Code Number: oc07124 Neisseria meningitidis retains its ability to cause endemic and hiperendemic disease in human population living in any environment, as well as localized outbreaks and massive epidemics in civilians and military personnel. In Rio de Janeiro it has been reported in the 1990s as prolonged outbreak of serogroup B and at least one epidemic of serogroup C was well defined, both demanding quick action by the Public Health authorities. We report here the emergence of serogroup W135 meningococcal disease causing endemic and case cluster in Rio de Janeiro during the first years of this new century. Key words: Neisseria meningitidis - meningococcal disease - serogroup W135 Neisseria meningitidis is a human pathogen with potential to cause life-threatening disease of abrupt onset in susceptible individuals, which can be rapidly progressive. Among the 12 capsular serogroups, more than 90% of the reported cases are caused by serogoups A, B, and C (WHO 1998). Other serogroups are seldom isolated from patients with invasive disease, especially in previously normal individuals in regard to immune mechanisms against invasive infection. Nevertheless, serogroups such as X and W135, considered as rare until recently, emerged during the second half of the 1990s as a cause of sporadic cases, localized outbreaks, and epidemic in Africa and Arabian Peninsula, followed by observations of intercontinental spread of some clones bearing one of this capsular serogroups (Report of a WHO Consultation 2001, Djibo et al. 2003, Pollard et al. 2004). In 1990 to 2001, strains of N. meningitidis serogroups B (67%) and, to lesser extent, C (30%) predominated in cases diagnosed in the vast territory of Brazil. It is important to take notice of only 2% of cases were caused by serogroup W135, 0.5% by serogroups other than these three, and 0.5% by isolates designated as nongroupable (Lemos et al. 2006). Epidemic of meningococcal disease is a recurrent public health issue since the enlightenment of an outbreak in military personnel by Olympio da Fonseca in the city of Rio de Janeiro in 1842 (Almeida 1921); before this century due to N. meningitidis capsular serogroups A, B, and C (Barroso 1998). Truly, the last massive epidemic in civilian living in the state of Rio de Janeiro was in the first half of the 1970s (Doença Meningocócica no Estado da Guanabara 1974). During the last epidemics waves of disease, the reported incidence increase and decrease slowly over several years and seldom reach more than 10 cases per 100,000 population (Barroso et al. 1996, 2002). Meningococcal disease due to serogroup B emerged as a serious threat in the 1970s in Europe (Caugant 1998) and it has affected the population of Rio de Janeiro since 1988 (Figure). The incidence of the disease increased and after the epidemic peak in 1991 it did not return to the level recorded before this event; then it remained as hiperendemic disease 5-10 cases/100,000/year (Barroso et al. 2002). The serogroup B strains isolated from patients were of phenotype 4,7:P1.19,15 or 4,7:P1.7,1 belonging to the epidemic clones of the ET-5 complex, which had been spread to countries outside Europe (Barroso 1998). In 1993 the number of cases of serogroup C disease began to increase and in 1995 the epidemic peaked with 10 cases/100,000 population; a shift in the age-distribution of the disease was observed. The epidemic strain was characterized as C:2b:P1.10 belonging genetically to the cluster A4 (Barroso et al. 1996) associated with epidemic disease in the Americas and Europe (Caugant 1998). A few strains of the serogroup W135 were assigned to new electrophoretic types (Barroso et al. 1996). An increase of meningococcal disease was recently reported in Rio de Janeiro (Pedro et al. 2007). In 2003 to 2005, 1244 cases were notified to the Rio de Janeiro State Department of Health, accompanied by a lethality of 22%. In the meantime, 67% (831) were included as suspected cases (clinically diagnosed bacterial meningitis with a suggestive rash or purpura fulminans; A39.9, ISCD-10). Of the 413 confirmed cases (A39.0+G01* or A39.2, ISCD-10), 351 were detected by culture or latex agglutination test and 62 by polymerase chain reaction (PCR) assays. The increase in terms of numbers of cases was mainly attributed to serogroup C and W135 disease (Figure). In that period, there were 229 (55%) serogroup B, 132 (32%) serogroup C, and 43 (11%) serogroup W135 cases diagnosed; 9 (2%) cases were identified as serogroups A, 29E, X or Y. Between 1988 and 2002, there were 3225 (69.3%) serogroup B, 1382 (29.7%) serogroup C, 16 (0.4%) serogroup A, 14 (0.3%) serogroup W135, 4 (0.1%) serogroup Y, and 10 (0.2%) nongroupable cases reported. It represented a significant increment of cases caused by serogroup W135, compared with results of 15 years of laboratory-based surveillance. The median age was 19-years old and 31% were over 20-years old for W135 cases diagnosed between 2003 and 2005; 9% were elderly patients (> 60 years). Whilst in the previous period, the median age was 12-years old and 15% were over 20-years old. In strains submitted for sero-subtyping, serogroup W135 and some serogroup C organisms express a class 2 outer membrane protein, generally characterized as serotype 2a and with a class 1 protein many times characterized as P1.2 or P1.5,2. Before 2000, clinical isolates of serogroup C were often characterized as C:2a:P1.2 or C2b:P1.10, 1.3 and serogroup W135 as C:19,10:P1.16 or W135:19:nt in the Rio de Janeiro Region. The E-test (AB BIODISK) for testing susceptibility of the serogroup W135 organisms did not show resistance to penicillin, chloranphenicol, ceftriaxone, rifampicin, and ciprofloxacin; 50% were sulfadiazine resistant. The inception of PCR assays in 2005 for clinical research of suppurative meningitis in the Oswaldo Cruz Institute has contributed for the demonstration of meningococcal aetiology and genogrouping (Rebelo et al. 2006, Pedro et al. 2007). Using PCR for diagnostic purposes, case cluster of serogroup W135 was identified in the city of Nova Iguaçu, in 2004, affecting young children (Pedro et al. 2007) and due to serogroup C in the city of Rio de Janeiro, in 2006, in a group of young adults from the same working place and in the city of Petrópolis, in 2007, in children attending a crèche (Barroso, unpublished observations). Sporadic cases of disease caused by both serogroups continue to be reported into the Metropolitan area. In 2006 (data is not yet definitive), 23 cases of serogroup B, 30 cases of serogroup C, and 17 cases of serogroup W135 were notified to the Rio de Janeiro State Department of Health. At present, N. meningitidis capsular serogroup W135 and part of serogroup C has been isolated from cases in Rio de Janeiro expressing the same phenotype of the clone associated with Hajj-related outbreaks of meningococcal disease identified as W135:2a:P1.5, 1.2 - ST-11 (Report of a WHO Consultation 2001). This clone has been spread to countries around the world after the first reported outbreak in Saudi Arabia in the year 2000. Strains genetically related to the ST-11 complex have been described bearing serogroup C or W135 polysaccharide capsules as reported in North America (Pollard et al. 2004). It has serious implication for vaccine design and Public Health response to situations demanding quick action in our community, because the tetravalent meningococcal vaccine (A+C+Y+ W135) is not available in Brazil. Additional studies are being conducted to determine the antigenic and genetic variation in serogroup C and W135 N. meningitidis isolated from patients and carriers in the city of Rio de Janeiro, which has no implication for planning vaccine implementation taking into account the current scenario and the specificity of the vaccine for each capsular polysaccharide (WHO 1998). ACKNOWLEDEGMENTS To Dr Ana Paula de Lemos at the National Reference Meningitis Centre, Adolfo Lutz Institute who did the sero-subtyping and Dr Maria de Fátima Calderaro, Meningitis Advisory Committee, Rio de Janeiro State Department of Health for providing the epidemiological surveillance data. REFERENCES
Copyright 2007 Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc07124f1.jpg] |
| |||||||||

{kind=link}