 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memórias do Instituto Oswaldo Cruz, Vol. 102, No. 8, December, 2007, pp. 937-941 Antigenic and genomic characterization of adenovirus associated to respiratory infections in children living in Northeast Brazil Fernanda EA Moura/+, Jacó RL de Mesquita*, Silvana AR Portes**, Eduardo AG Ramos***, Marilda M Siqueira** Laboratório de Virologia *Programa de Pós-Graduação
em Microbiologia Médica, Departamento de Patologia e Medicina
Legal, Universidade Federal do Ceará, R. Monsenhor Furtado
s/n, 60441-750 Fortaleza, CE, Brasil **Laboratório de Vírus
Respiratórios, Instituto Oswaldo Cruz-Fiocruz, Rio de Janeiro,
RJ, Brasil ***Laboratório de Patologia, Centro de Pesquisas
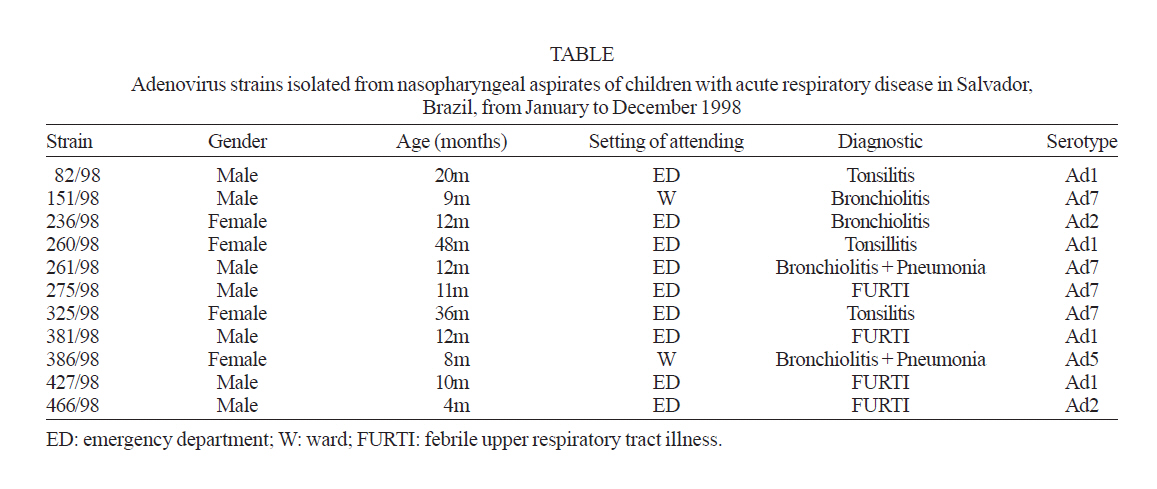
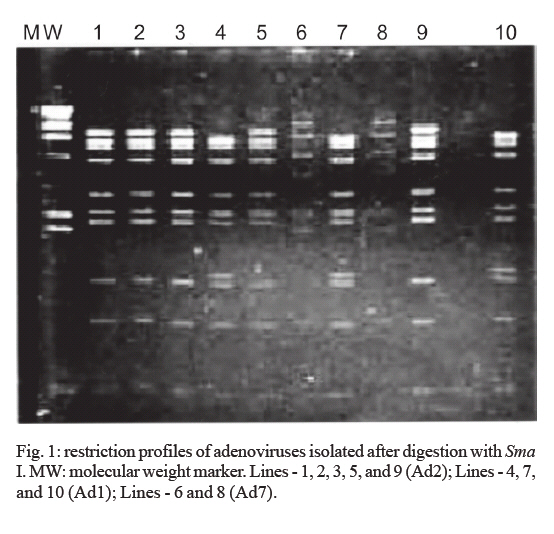
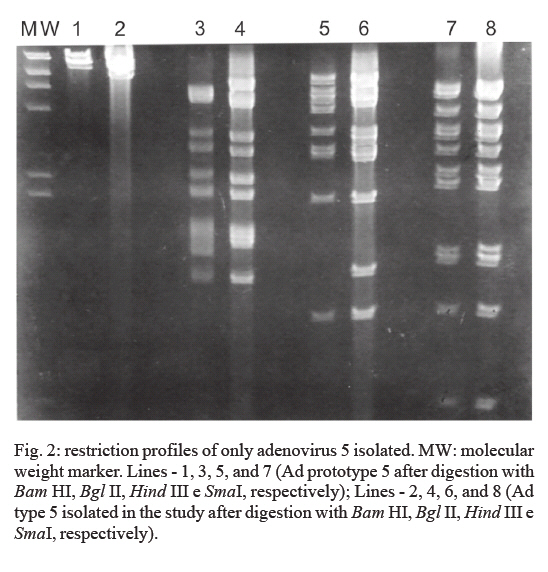
Gonçalo Moniz-Fiocruz, Salvador, BA, Brasil Received 10 July 2007 Code Number: oc07169 From January to December 1998, nasopharyngeal aspirates were obtained from 482 children with acute respiratory infections attended in emergence department and wards of a teaching hospital in the city of Salvador, Brazil. The samples were tested for the presence of adenovirus by isolation in tissue culture and indirect immunofluorescence assay. Eleven adenoviruses were detected by both methods in the same clinical samples. Infections by adenovirus were observed during seven months of the year without association with rainy season. Genome analysis was performed on these 11 isolates. Species C was represented by serotypes 1, 2 and 5. Within species B, only serotype 7 (Ad7) was detected. Two genomic variants of Ad1, two variants of Ad2, one of Ad5, and one of Ad7 (7h) were identified. This is the first study of molecular epidemiology of adenovirus associated to acute respiratory infections in children living in Northeast Brazil, and contributes to a better understanding of adenovirus infections in the country. Key words: adenovirus - acute respiratory infections - genotypes - Brazil Adenoviruses (Ad) are a significant cause of acute respiratory infections (ARI), including bronchiolitis and pneumonia, in infants and young children. To date 51 human Ad serotypes have been identified, grouped in six species (Ad A to F) based on a variety of parameters, including biochemical, biophysical characteristics and nucleotide, and deduced aminoacid sequences (Wadell 1984, Adrian et al. 1986, van Regenmortel 1999). Ad-B species have been divided further into two subgroups: B1, including Ad type 3 (Ad3), Ad7, Ad16, Ad21 and Ad50, and B2, including Ad11, Ad14, Ad34, and Ad35 (Stone et al. 2003). The serotypes more frequently recovered from children with ARI were: Ad1, Ad2, Ad3, Ad5, and Ad7 (Schimitz et al. 1983). Ad3, Ad7 and, less frequently, Ad 21, are involved in severe infections in children associated in outbreaks (Kim et al. 2003). In clinical practice, when the role of Ad is suspected in cases of ARI, the diagnosis is currently based on viral isolation techniques, immunofluorescence and, enzyme-linked immunosorbent assays (Vabret et al. 2004). Polymerase chain reaction (PCR), real-time PCR and immunochromatographic kits have recently become available for this purpose (Fujimoto et al. 2004). Typing of Ads isolates can be achieved by neutralization, hemmaglutination inhibition, restriction endonuclease analysis (REA), sequencing and, PCR combined with REA (Allard et al. 2001, Sarantis et al. 2004). Until recently, the interest in serotype and genotype determination of Ad isolates was mainly epidemiological, however, this has changed due to the increasingly clear association between specific serotypes and genotypes and more severe disease presentation (Kajon & Wadell 1994, Larrañaga et al. 2000, Carballal et al. 2002). Genome typing or REA has been used to ascertain the genetic variation within the species. The identification of genome types offers a chance to follow the epidemiological distribution of these viruses in time and space, and allows their pathogenic and other biological characteristics to be compared. Several reports of the genomic characterization of Brazilian Ad isolates from patients with respiratory, ocular and gastrointestinal infections have been published since 1988, but none of them included any Ad isolates of patients living in Northeast Brazil (Wadell et al. 1985, Gomes et al. 1988, Moraes et al. 1997, 1998, Kajon et al. 1999, de Albuquerque et al. 2003, Moura et al. 2007). These studies have shown an important genetic variability for members of subgenus C. Among members of subgenus B, serotype 3 has been represented by genotypes 3p1 and 3a variant described previously (Kajon et al. 1999, Moura et al. 2007). Data of Brazilian studies suggest replacements of Ad7 genome types circulating in Brazil as has been reported in other studies (Kajon & Wadell 1994, Erdman et al. 2000). The purpose of this study was to describe epidemiological, clinical, and viral characteristics of ARIs by Ad in a group of children attending a teaching hospital in the city of Salvador during the year of 1998. SUBJECTS, MATERIALS AND METHODS Samples of nasopharyngeal aspirates were collected from children presenting upper or lower acute respiratory tract infections who were attending at Centro Pediátrico Hosanah de Oliveira (CPHO) in the city of Salvador, northeast Brazil, from January to December 1998. Children under five years of age and with disease of less than seven days of evolution were included in the study. All samples were tested by an indirect immunofluorescence assay (IFA) to Ad, respiratory syncytial virus (RSV), influenza A and B, parainfluenzaviruses 1, 2 and 3 (Chemicon International, Temecula, CA, USA) no more than 4 h after collection. Samples were stored in virus transport medium (Eagle's Minimal Essential Medium with 100 U penicillin and 50 mg gentamicin) and 4% bovine serum albumin at -70ºC until to be inoculated on HEp-2 cells, when tubes with cells were not available to immediate inoculation. All samples were inoculated on HEp-2 that were grown in Eagle's Minimal Essential Medium containing 10% of fetal bovine serum, 100 µl penicilin and 50 µl gentamicin. The cells were observed daily to detect the cytopathic effect (CPE). IFA was performed to confirm the isolation of Ad. Supernatants of culture positive to Ad were stored at -70ºC. All Ad isolated strains were serotyped by neutralization with rabbit reference antisera for Ad types 1, 2, 3, 4, 5, 6, and 7, following standard protocols (Hierholtzer 1995). HEp-2 cells grown in 75 cm2 plastic flasks were inoculated with Ad that were stored at -70ºC. Viral DNAs were extracted from infected cells as described previously (Shinagawa et al. 1983). Aliquots containing 1-2 µg of viral DNAs were digested with 10 units of different endonucleases (Bam HI, Bgl II, BstE II, Hind III, and Sma I) under conditions specified by the manufacturers (Boehringer, Mannheim, Germany). DNA fragments were loaded onto 1.2% agarose gels. Bands were observed by using a transilluminator, and photographed using Polaroid Land film 665 or 667. The resulting restriction profiles were assigned to corresponding virus species and genotypes according to the literature data. Ethical issues - This study was approved by Ethics Committee of CPHO (resolution 14/97). Parents or legal guardians provided signed informed consents for inclusion of children in the study. From January to December 1998, 482 samples were collected, 360 from patients attending the emergency department and 122 from hospitalized patients. Viral infections were detected in 154 patients. Adenoviral infections (11 cases) represented 7.14% of viral infections, and 2.28% of all cases of ARI. Ads were the fourth viral agent after RSV, influenza A and parainfluenza 3. In this study, Ad infections were more prevalent in the children attending the emergence than in those being treated at wards. Adenoviral infections were observed in children aged two months to four years with most of them occurred during the first year of their lives (81.8%). The majority of infections caused by Ad (63.6%) were diagnosed as upper respiratory tract infections (URTI). Cases of lower respiratory tract infections (LRTI) were observed in outpatients and those hospitalized. Characteristics of the children with ARI caused by Ad are shown in Table. All of the 11 Ad detected by IFA were isolated in HEp-2 cells. The genomic analysis showed that 83.3% of the analyzed isolates belonged to the species C, and was represented by serotypes 1, 2 and 5 followed by species represented by serotype 7 accounting for 16.7% of the cases. The seroneutralization test identified four Ad1, two Ad2, one Ad5 and four Ad7. The restriction profiles of adeno-viruses analysed in this study are shown in Figs 1 and 2. Two DNA variants were observed among strains classified as Ad1, one was identified as genome type D1 and three as D10 (only two of them are showed in the Fig. 2). Strains of Ad2 were characterized as genome type D5. The only Ad5 of this study had a similar pattern to that named as 5# in an Argentine study (Kajon & Wadell 1992). All four Ad7 identified were characterized as 7h. DISCUSSION In this study Ad infections were more prevalent in the children who were attended in the emergency department than those attended in the wards. This finding differs from data reported by other Brazilian and South American studies, which indicate Ad as the second most prevalent virus in ARI observed in hospitalized children (Nascimento et al. 1991, Kajon et al. 1999, Larrañaga et al. 2000, Straliotto et al. 2002). In this study the rate of ARI by Ad in hospitalized patients was 1.6%, while in other studies this rate ranged from 3.3% to 12.6% (Larrañaga et al. 2000, Hong et al. 2001, Tsai et al. 2001, Chen et al. 2004). Respiratory infections by Ad are generally characterized as self-limited mild URTI, however LRTI can occur, and some cases present as severe pneumonia followed by respiratory failure, serious sequelae or fatal outcome (Kajon & Wadell 1994, Farng et al. 2002). In other similar studies, Ad was seen to act as an agent of URTI (Tsai et al. 2001, Echavarria et al. 2006). In a recent study, Ad was detected in 9.4% of nasal swab samples collected from outpatients with flu-like symptoms (Echavarria et al. 2006). The impact and severity of Ad infections were shown in a study of viral acute lower tract infections in children admitted to the pediatric intensive care unit of two hospitals in the city of Porto Alegre (Straliotto et al. 2004). In that study, 7.7% of viral respiratory infections were due to Ad. Moreover those infections showed a high case fatality rate of 25%. During the twelve months of study, Ad infections were observed year round without a clear seasonality as it was observed in other Brazilian cities and in other tropical countries (Arruda et al. 1991, Nascimento et al. 1991, Shek & Lee 2003, Tsuchiya et al. 2005). Referring to the antigenic diversity of Ad associated to children ARI in Salvador in 1998 it was observed that members of species C predominated, in accordance with other studies (Frabasile et al. 2005, Echavarria et al. 2006). This characteristic differs from those seen in studies in Argentina and Chile, where members of species B were the most prevalent (Kajon et al. 1996, Videla et al. 1998, Larrañaga et al. 2000, Carballal et al. 2002). In spite of the small number of Ad analyzed, the results of this study show a relative genetic variability for members of species C, as observed previously (Kajon et al. 1999, Frabasile et al. 2005, Moura et al. 2007). Several studies have shown that one particular genotype can circulate in different geographic regions in different years. The data obtained in this study show that genotypes circulating in Salvador during 1998 had circulated in other Brazilian cities and other South American countries in previous years. The genotypes D1 and D10 of Ad1, and the genotype D5 of Ad2 identified in Salvador during 1998 had circulated in the cities of Belém and Rio de Janeiro in the 80s and early 90s (Kajon et al. 1999). The only Ad5 detected in Salvador had circulated in Argentina between 1984 and 1988 (Kajon & Wadell 1992). The finding of four Ad of genotype 7h in Salvador in 1998 confirms the tendency of this genotype to spread rapidly, since it was first identified in Argentina (Kajon & Wadell 1994). The occurrence of this genome type remained restricted in countries of South Cone of South America (Argentina, Chile and Uruguay) until 1994, when it was identified in Southeast Brazil associated to a case of follicular conjunctivitis (Tanaka et al. 2000). The circulation of this genome type outside of South America occurred in 1996 in Japan and in 1998 in Southeast of United States (Hashido et al. 1999, Erdman et al. 2000). The first identification of Ad7h in case of ARI in Brazil occurred in 1995 (Moura et al. 2007). Previous analysis of Ad7 in Brazil had identified only the genome types Ad7b and Ad7e (Wadell et al. 1985, Moraes et al. 1997, Kajon et al. 1999). The analysis of 40 strains of Ad7 identified in cases of ARI in patients living in Southern and Southeastern regions of Brazil showed that in a period of 12 years (1980-1991) only the genome types Ad7b and Ad7e were identified (Moraes et al. 1997). Similar result was observed among 14 strains of Ad7 isolated from respiratory specimens from patients with ARI living in Northern and Southeastern regions between 1976 and 1995 (Kajon et al. 1999). In the more recent Brazilian study about molecular epidemiology of adenovirus revealed that all 17 serotype isolates belonged to genome type 7h (Moura et al. 2007). Shifts or replacements of genome types of Ad7 had been reported in the former Soviet Union, Argentina and Australia (Li & Wadell 1986, Galovina et al. 1991, Kajon & Wadell 1994). More continuous studies with a larger number of strains in analysis are required in order to characterize if in Brazil the genome types Ad7b and Ad7e were replaced by Ad7h as has been suggested in the Brazilian studies cited previously. The principal limitations of this study are related to the low number of strains analyzed and the long time past since the circulation of them. These strains of Ad represented the only isolated from respiratory specimens of children living in Northeast Brazil available for study, and contribute for a better understanding of Ad in the country. The comparison of the results of the present study with those presented in Brazilian studies published before and after 1998 allows us to observe that the circulation of some genotypes of adenovirus detected in Salvador had been reported before of the present study, and they remained circulating in Brazil years after. At same time, this study confirms the quick spread of Ad7h in South America. This is the first report about molecular epidemiology of adenovirus circulating in Northeast Brazil. REFERENCES
Copyright 2007 Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc07169f2.jpg] [oc07169f1.jpg] [oc07169t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}