 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memórias do Instituto Oswaldo Cruz, Vol. 103, No. 1, February, 2008, pp. 79-84 Chloroquine resistant Plasmodium falciparum malaria in Osogbo Nigeria: efficacy of amodiaquine + sulfadoxine-pyrimethamine and chloroquine + chlorpheniramine for treatment TO Ogungbamigbe/1, O Ojurongbe1,4/+, PS Ogunro1,2, BM Okanlawon3, SO Kolawole Department
of Pharmacology & Therapeutics 4Department of Medical
Microbiology and Parasitology, College of Health Sciences, Ladoke
Akintola University of Technology, Osogbo, Nigeria 2Department
of Chemical Pathology 3Department of Biomedical Sciences 1Malaria Research Clinic & Laboratory, College of
Health Sciences, Ladoke Akintola University Teaching Hospital, Osogbo,
Nigeria Received
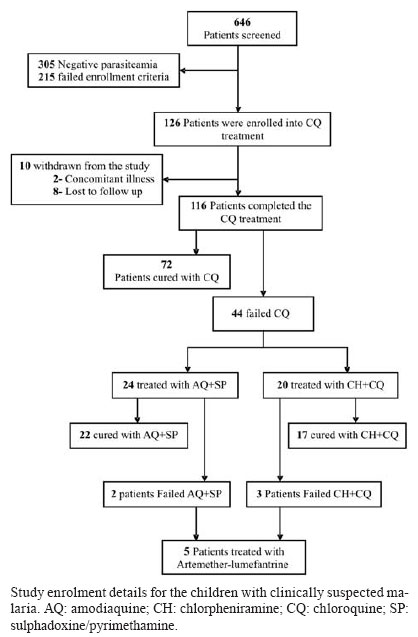
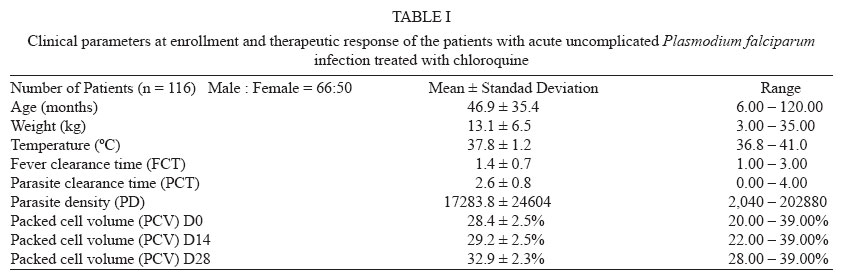
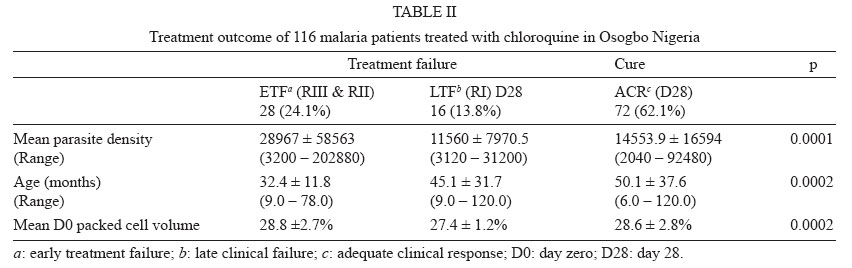
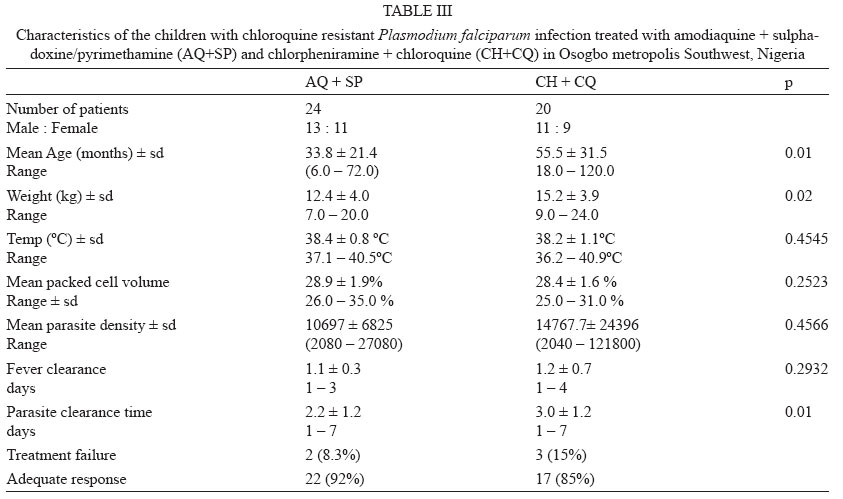
5 September 2007 Code Number: oc08012 Chloroquine (CQ) resistance in Plasmodium falciparum contributes to increasing malaria-attributable morbidity and mortality in Sub-Saharan Africa. Despite a change in drug policy, continued prescription of CQ did not abate. Therefore the therapeutic efficacy of CQ in uncomplicated falciparum malaria patients was assessed in a standard 28-day protocol in 116 children aged between six and 120 months in Osogbo, Southwest Nigeria. Parasitological and clinical assessments of response to treatment showed that 72 (62.1%) of the patients were cured and 44 (37.9%) failed the CQ treatment. High initial parasite density and young age were independent predictors for early treatment failure. Out of the 44 patients that failed CQ, 24 received amodiaquine + sulphadoxine/pyrimethamine (AQ+SP) and 20 received chlorpheniramine + chloroquine (CH+CQ) combinations. Mean fever clearance time in those treated with AQ+SP was not significantly different from those treated with CH+CQ (p = 0.05). There was no significant difference in the mean parasite density of the two groups. The cure rate for AQ+SP group was 92% while those of CH+CQ was 85%. There was a significant difference in parasite clearance time (p = 0.01) between the two groups. The 38% treatment failure for CQ reported in this study is higher than the 10% recommended by World Health Organization in other to effect change in antimalarial treatment policy. Hence we conclude that CQ can no more be solely relied upon for the treatment of falciparum malaria in Osogbo, Nigeria. AQ+SP and CH+CQ are effective in the treatment of acute uncomplicated malaria and may be considered as useful alternative drugs in the absence of artemisinin-based combination therapies. Key words: chloroquine - resistance - Plasmodium falciparum - non-ACTs - Nigeria Malaria continues to be one of the leading killer diseases in the tropical areas affecting the world's poorest children and pregnant women and resistance of Plasmodium falciparumto chloroquine (CQ) has contributed to a substantial increase in its morbidity and mortality (Trape 2001). CQ has been the most frequently used drug for the first-line treatment of malaria infections in many tropical countries because it is cheap, low in toxicity, effective against all forms of malaria, relatively easy to manufacture and chemically stable and thus it is readily stored and transported even under extreme climatic conditions (Ginsburg 2005). Despite the recent change in National malaria drug policy to artemisinin-based combination therapy (ACT) in Nigeria, CQ still remains the commonest antimalarial drug widely prescribed in the treatment of falciparum infection in certain areas of the country (Ogungbamigbe et al. 2005). Continuous monitoring of the efficacy and the level of resistance development to CQ is therefore increasingly important to guide decision-makers on drug policy and enforcement. To counter the threat of resistance of P. falciparum and to improve treatment outcomes, ACTs against malaria are now recommended (WHO 2006). It has been reported that antimalarial combination therapies could improve therapeutic effectiveness, reduce gametocyte carriage and delay the emergence and spread of drug resistant parasites (WHO 2006). Non-ACTs regimens of chloroquine, amodiaquine (AQ) and sulphadoxine/pyrimethamine (SP) are reported to be effective, safe, readily available, and affordable compared to ACTs. Chlorpheniramine (CH), a histamine H1-receptor antagonist commonly prescribed in combination with CQ for the treatment of CQ-induced pruritus, has been shown to reverse CQ resistance in African isolates of P. falciparum malaria (Basco & Le Bras 1994, Okonkwo et al. 1999). Although the combination of CH+CQ is not by definition an antimalarial combination therapy, it has been shown to be more effective than CQ alone (Sowunmi et al. 1997, 2000). Also the combination of AQ+SP was recently shown to be more effective than artemether-lumefantrine for the treatment of uncomplicated malaria in Burkina Fasso (Zongo et al. 2007). This combination has also been shown to be effective in the treatment of malaria in Southwest Nigeria (Sowunmi 2002, Sowunmi et al. 2006). Several countries in West Africa, including Nigeria, have changed their recommended first-line treatment for uncomplicated malaria to artemether-lumefantrine. However, high cost (US$ 6.20-11.7 per adult course) (Yeung et al. 2004) and non-availability of this drug has been limiting the effective use of this drug, rather the cheap and readily available CQ is continually being used. The aim of this work therefore is to assess the efficacy of chloroquine in Osogbo Western Nigeria. The efficacy of non-ACTs (CH+CQ and AQ+SP) for the treatment of CQ resistance falciparum malaria was also investigated. PATIENTS, MATERIALS AND METHOD The study took place at the Malaria research clinic and laboratory, Ladoke Akintola University of Technology (LAUTECH) Teaching Hospital (LTH) and General Hospital Asubiaro, both in Osogbo Metropolis. Osogbo lies 100 km North of Ibadan in Southwest Nigeria, where malaria is hyper-endemic (Salako et al. 1990). Malaria transmission in Southwest Nigeria is perennial but seasonal and peaks during the rainy season, which normally runs from April to November. Recruitment and follow-up for the study took place between August 2004 and July 2005. The study received ethical approval from Joint College of Health Sciences/Ladoke Akintola University Teaching Hospital and Osun State Hospitals Management Board ethics review committees. Out of 646 children that were screened, 126 were enrolled and 116 were successfully followed up for 28 days. To be enrolled the children had to be aged between 6-120 months, presenting with symptoms compatible with acute uncomplicated P. falciparum malaria with history of fever in the preceding 24-48 h or temperature > 37.5ºC and pure P. falciparum parasitemia > 2000 asexual forms/µl of blood. Patients with concomitant illnesses, sickle cell anemia or severe complicated malaria were excluded (WHO 1990). Informed consent of the parent or guardian was obtained for each child. A child is withdrawn from the study if there is development of concomitant illness during the follow-up period or with parent or guardian seeking voluntary withdrawal. Before enrollment, a medical history of each patient was obtained from the parent or guardian, after which the child was examined. Body weight and auxiliary temperature were recorded. Thick smears were prepared from finger-prick blood samples on days (D) 0-3, D7, D14, D21, D28 for parasite identification and quantification. Venous blood and filter paper samples were collected for full blood counts and polymerase chain reaction (PCR) analysis during follow up visit. The PCR analysis was done to distinguish re-infection from recrudescence. Drug treatment - The detected parasitaemic cases were treated with 25 mg/kg CQ in divided doses for three days at 10 mg/kg daily on D0 and D1 and 5 mg/kg on D2. Subsequent follow up appointments were scheduled for days 3, 7, 14, 21 and 28. All children who failed CQ were allocated randomly into two groups to receive a combination of AQ+SP or CH+CQ. AQ was given at a dose of 10 mg/kg daily for three days and SP at 25 mg/kg as single dose on D0, CH was given at 6-8 mg 8 hourly for five days (D0-D4) (Sowunmi et al. 1997) in addition to the standard dose of CQ at 25 mg/kg for three days. Patients were followed up daily on D0-D3, D7, D14, D21 and D28. Artemeter-lumefantrine was used as a rescue drug for patients that failed the combination of AQ+SP or CH+CQ. All the drugs were administered orally by a physician and observed for at least 3 h to ensure that the drugs were not vomited. Drugs were re-administered following initial vomiting, but withdrawn from the study with another episode of vomiting. Thick blood films were prepared on each visit day for parasite quantification and identification. Evaluation of response - Classification of responses to treatment was done according to the World Health Organization (WHO) criteria (WHO 2003). Clinical observations were recorded daily for four days (days 0-3) and on days 7, 14, 21 and 28. Parents or guardian were questioned and children examined for evidence or presence of adverse reactions to the drugs. Thick blood smear was examined during each visit and parasitemia was estimated by counting asexual parasites against 200 leucocytes with the assumption that each patient had 8,000 leucocytes/µl blood (White 1996). Therapeutic outcome was classified as early treatment failure (ETF), late clinical failure (LTF), late parasitological failure (LPF), or adequate clinical and parasitological response (ACPR) (WHO 2003). Treatment was considered a failure if D2 parasitaemia was greater than D0 or D3 parasitaemia was greater than 25% of the D0 value (RIII), if parasiteamia did not clear by D7 (RII), or if parasiteamia cleared before D7, but reappeared before D28 (RI). Response was classified as sensitive (S) if the D3 parasite density was less than 25% of the D0 count and no parasites were detected during the remaining follow-up days. Treatment failure rates were corrected by merozoite surface protein 2 (msp-2) genotyping of parasites at enrollment and recrudescence (Snounou et al. 1999). The fever clearance time (FCT) was defined as the time taken from drug administration until axillary temperature falls below 37.4ºC and remains at that value for 72 h. Parasite clearance time (PCT) was defined as the time taken from drug administration until no patent parasiteamia is detected. Cure rates were defined as the proportions of patients who remained free of parasiteamia on D14, and D28 of follow-up. Statistical analysis - Data were analyzed using R version 2.51 statistical software by The R Foundation for Statistical Computing 2007. Welch two Sample t-test was carried out for the different variables. The alternative hypothesis was that true difference in means is not equal to 0. Also proportions were compared by Chi-square (X2) with Yates' correction or by Fisher's exact tests using Graph-pad instat of Graphpad software Incorporation USA. A p-value of < 0.05 was taken as significant. RESULTS Clinical features and therapeutic response to CQ - In all, 646 children were screened, 126 fulfilled all the enrollment criteria while 116 children were successfully followed up for 28 days (Figure). Table I shows the enrollment data and therapeutic responses to CQ in 116 patients. ACPR was seen in 72 (62.1%) while 45 (38.2%) had CQ treatment failure. When adjusted with PCR analysis one of the cases was a re-infection while the remaining 44 (37.9%) cases were evidently recrudescence. Table II shows the breakdown of the cure rate and treatment failure recorded in the study. Twenty eight (24.1%) had ETF (RIII and RII) while 16 (13.8%) had LTF (RI). A significant difference (p = 0.001) was recorded in mean parasite density of the treatment outcome group with the ETF recording the highest mean parasite density of 28,967 ± 58,563 (range of 3,200-202,880). Also there was a significant difference (p = 0.0002) in age, in relation to treatment outcome. Patients having ACPR were significantly older and tend to have lower initial parasite densities than children who experienced ETF. Clinical features and therapeutic response to the SP+AQ and CQ+CH combinations- 44 children comprising of 24 males and 20 females who failed CQ treatment were randomly treated with AQ+SP and CH+CQ. 24 (55%), 13 males and 11 females received AQ+SP combination while 20 (45.5%) 11 males and nine females received CH+CQ combination. The pre-enrolment characteristics of the two treatment groups are shown in Table III. Out of the 23 children treated with AQ+SP combination, ACPR was seen in 21 (92%), one had parasiteamia without clinical malaria up till D28 while the other had recrudescence by D21. Of the 20 children treated with CH+CQ, cure rate was on 17 (85%) while 3 (15%) had treatment failure at the end of D28. The therapeutic responses of the patients are shown in Table III. There was no significant difference in the average FCT in patients treated with AQ+SP (1.1 ± 0.3 days with a range of 1-3 days) and those treated with CH+CQ (1.2 ± 0.7 days with a range of 1-4 days). The average PCT was significantly different in the two groups with those treated with AQ+SP having 2.2 ± 1.6 days while those treated with CH+CQ was higher with 3.0 ± 1.2. Adverse reactions - Pruritus was the most significant adverse reaction common among the children followed by vomiting and diarrhea. All the adverse reactions except for the sleep disturbance in those with pruritus were mild and none necessitated discontinuation of therapy. DISCUSSION The affordable and widely available antimalarial, CQ, that was in the past the mainstay of malaria control is now widely reported to be ineffective in the treatment of falciparum malaria in most endemic areas (Mockenhaupt et al. 2005b, Olumese et al. 2002). Although it was recently shown that after CQ has been withdrawn from the market, CQ-sensitive P. falciparumre-emerged and CQ could again be used successfully as an antimalarial (Laufer et al. 2006). In this study, 62% of the patients were cured with CQ while treatment failure occurred in 38%. The failure rate recorded in this study was higher than the 31% previously reported in Ibadan a neighboring town to Osogbo (Happi et al. 2004). We have also previously reported a high prevalence of pfcrt 76T gene known to be associated with CQ resistance in this area (Ojurongbe et al. 2007). The overall assessment of these reports is that CQ can no longer be totally relied upon for the treatment of uncomplicated falciparum malaria in this area. WHO recommendation that a change of first-line treatment should be initiated if the total failure proportion exceeds 10% (WHO 2006). A greater percentage of the patients with ACPR are older, and were with fewer parasites. This underscored the fact that acquired immunity contributed to parasite clearance and clinical improvement (Maire et al. 2006). It also shows that high initial parasitemia and age are potential risk factors to early treatment failure. The agreement between clinical efficacy and parasitological response was at variance as less than 12% of parasitologically resistant cases were observed to have adequate clinical cure. Ehrhardt et al. (2002) found that more than half of the parasitologically resistant cases were considered to have ACPR, where they reported 29% clinical failure but 57% parasitological resistance in Ghana. While in a Malian study the difference was marginal, 10%-15% treatment failure and 13%-17% parasitological resistance (Plowe et al. 2001, Ehrhardt et al. 2002). The relatively high endemicity in this area, allows for development of immune responses which may partly be responsible for the observed variation in the clinical and parasitological responses. The result of this study showed that AQ+SP and CH+CQ were effective for clearance of CQ resistant malaria infections with the combination of AQ+SP being more effective for reduction of the overall incidence of malaria after treatment. The efficacy of CH+CQ for the treatment of CQ resistant malaria in Nigeria has been previously established (Sowunmi et al. 1997) and was again confirmed in this study. In this study 85% of children treated with this combination showed adequate clinical and parasitological response at D28 which differ from previous studies using other combination regimens based on the reversal phenomenon. In a similar study, using the same drugs but at a lower dose with longer duration for chlorpheniramine, a cure rate of 87.5% at D28 was reported (Okonkwo et al. 1999). The sustained effectiveness of this combination till now after almost a decade is as a consequence of the prescription of chlorpheniramine routinely to prevent CQ-induced pruritus in children and adults with malaria. This combination was not indicated for drug resistant malaria but its use has become a common practice among medical practitioners in Southwest Nigeria (Ogungbamigbe et al. 2005). Of the non-artemisinin combination regimens, AQ+SP has shown excellent antimalarial efficacy in most African studies, even in those from regions, such as east Africa, where levels of resistance to each component drug are high (Staedke et al. 2001, Schellenberg et al. 2002). In this study 92% of children treated showed adequate clinical and parasitological responses at D28 without any serious adverse reaction. In several comparative trials, AQ+SP has shown similar or better efficacy than that of artemisinin based combinations (Dorsey et al. 2002, Koram et al. 2005, Zongo et al. 2007). In a study where the monotherapy of AQ, and CQ was compared with their combinations with SP, a cure rate of 100% was recorded by D28 (Sowunmi 2002). Also in another comparative study of AQ and SP as monotherapy and as combination in Southern Cameroon a cure rate of 100% was reported for the combination and 85% for the individual monotherapy (Basco et al. 2002). It has been suggested that AQ+SP combination might be especially useful in West Africa, where resistance to both AQ and SP is low. This combination treatment had more than 94% efficacy against uncomplicated malaria in Nigeria (Sowunmi 2002) Ghana (Mockenhaupt et al. 2005a), and Burkina Faso (Zongo et al. 2005). The parasite clearance time in the combination of AQ+SP in our study was 2.2 ± 1.2 days this was similar to 2.1 ± 0.7 days that was reported in Ibadan in 2002 (Sowunmi 2002). While that of CH+CQ (3.0 ± 1.4 days) was higher than 2.0 ± 0.5 days previously reported in Ibadan (Okonkwo et al. 1999). The safety profile of new antimalarial regimens remains a point of concern. Both AQ and SP have been associated with toxic effect when used for long term chemoprophylaxis, but seems to be safe, effective and well tolerated for short term antimalarial treatment. Both combinations of CH+CQ and SP+AQ in our study were well tolerated only pruritus, which is a well known consequence of aminoquinoline treatment, was observed without any serious adverse events. There are some crucial issues that must be addressed in the implementation of combination therapy as replacement option to CQ; the cost of various combinations may be unavoidable in poor people which form the greater percentage of the disease burden thus encouraging continued prescription of CQ. The difficulty of co-blistering of the various combinations also may pose a problem of compliance with long-term implications for the development of drug resistance. Ideally, revision of drug policies must be considered long before evidences of clinical failures are reported. The change in treatment policy in Nigeria to ACTs without adequate sensitization and education of medical personnel may pose some difficulties that could lead to high morbidity and mortality. A resultant increase in resistance development of P. falciparum parasite to these new combinations may also arise since transition into an alternative compound may take some years before they are accepted and put into proper use (Shretta et al. 2000). Cost effectiveness analysis thus seems largely to favor the nationwide use of the AQ+SP combination in Nigeria. This combination should be encouraged since the failure rate is still low enough for the combination to be recommended (Sowunmi et al. 2005, Zongo et al. 2007). In Nigeria, a widespread therapeutic efficacy studies of individual combination has not been properly ascertained especially in different epidemiological settings. The AQ+SP combination seems to be safe, highly effective, relatively cheap and viable therapeutic option that may be of immediate value that can ensure the therapeutic lifespan of these drugs. It will also be necessary for the government to ensure that CQ be withdrawn from the market to discourage its continuous use. It was recently reported that CQ could regain its efficacy after been successfully withdrawn from the market (Laufer et al. 2006). It is also necessary to conduct extensive comparative efficacy studies of non-ACTs and artemisinin-based combinations in different epidemiological settings and their relative pharmaco-economics especially in resource poor sub-Saharan Africa that carries the highest disease burden. ACKNOWLEDGEMENTS To the management of LAUTECH, Ogbomoso for providing the financial support and materials for the research and Fidson drugs Nigeria Limited for supplying the chloroquine that was used in this study. To all the members of staff of Malaria Research Clinic and Laboratory, Department of Pharmacology and Therapeutics. To Mrs. Taiwo Ojurongbe who carried out the statistical analysis. REFERENCES
Copyright 2008 Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc08012t2.jpg] [oc08012t1.jpg] [oc08012f1.jpg] [oc08012t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}