 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
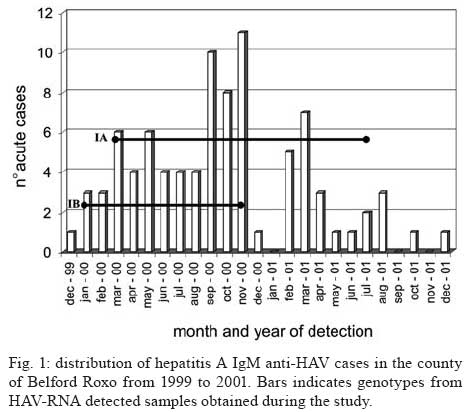
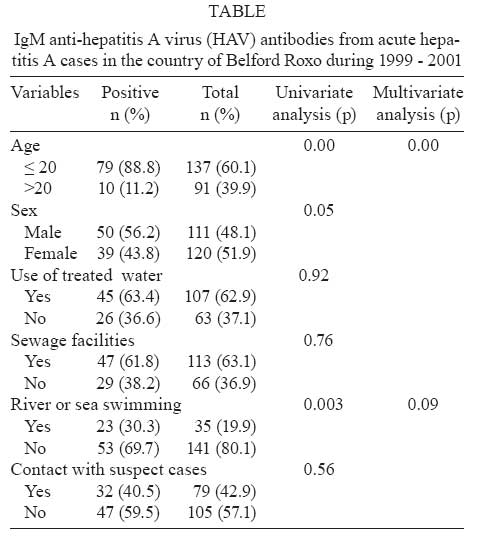
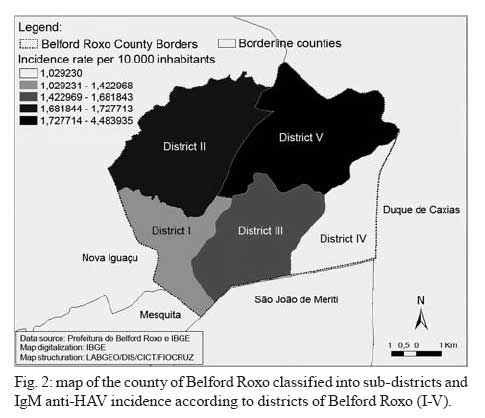
Memórias do Instituto Oswaldo Cruz, Vol. 103, No. 3, May 2008, pp. 254-258 Hepatitis A virus subgenotypes dissemination during a community outbreak in a surrounding region of Rio de Janeiro Débora Regina Lopes dos SantosI, +; Livia Melo VillarII; Vanessa Salete de PaulaI; Gerson Silva de LimaIII; Ana Maria Coimbra GasparI ILaboratório de Desenvolvimento Tecnológico Financial support: CNPq Received 21 November 2007 Code Number: oc08043 ABSTRACT From December 1999 to December 2001, many cases of hepatitis A were notified in the county of Belford Roxo involving individuals aged 0 to 79 years. Serum samples were collected to evaluate the prevalence of anti-hepatitis A virus (HAV) antibodies, to detect HAV-RNA and to correlate with possible risk factors of HAV infection. Serum samples were screened by commercial IgM and total anti-HAV antibody ELISA and HAV-RNA was isolated and subsequently amplified by reverse transcription-polymerase chain reaction (RT-PCR) at VP1/2A region, sequenced and analyzed. Total anti-HAV prevalence was 87.9% (203/231) and IgM anti-HAV prevalence was 38.7% (89/231). Multivariate analysis showed that individuals under 20 years old are risks groups to acquire the infection suggesting that hygienic habits of young subjects are the principal factor of transmission and so they could be the target for vaccine programs. HAV-RNA was amplified from 29 (32.5%) IgM anti-HAV positive patients and 26 samples were sequenced and classified into subgenotypes IB (8 isolates) and IA (18 isolates). Isolates classified into subgenotype IB were identical representing one distinct strain. We could observe both subgenotypes circulating during the study which suggests different sources of infection. Prophylactic measures as vaccination strategies added to improvements in hygienic and sanitary conditions would be highly effective to reduction of infection. Key words: hepatitis A virus - molecular epidemiology - co-circulation of subgenotypes IA and IB Hepatitis A virus (HAV) is an RNA virus that is transmitted mainly by fecal oral route and is the only member of the genus Hepatovirus of the Picornaviridae family (Melnick 1982, 1992). Studies on nucleic acid heterogeneity of HAV strains, in VP1/2A junction, characterize and group isolates in six different genotypes (I-VI) and six sub-genotypes (IA, IB, IIA, IIB, IIIA, and IIIB) (Robertson et al. 1992, Lu et al. 2004). Genotypes are distinguished by 15-25% sequence diversity, whereas sub-genotypes in each genotype differ in about 7.5% of base positions (Robertson et al. 1992). Comparison among nucleotide sequences allows genetically relating different strains during an outbreak and providing new insights into the molecular epidemiology of HAV. HAV is the main cause for acute viral hepatitis which represents a significant public health problem worldwide. However, a progressive decline in hepatitis A mortality rate could be seen in all Brazilian regions, being observed a rate of 0.2/100,000 inhabitants in 1980 to the rate of 0.02/100,000 inhabitants in 2002 (Vitral et al. 1998, 2006). The incidence of hepatitis A in Brazil has markedly decreased as showed by Vitral et al. (1998) who demonstraded that the HAV seroprevalence declined from 98.1 to 7.8% among children under the age of five in two different populations of low socioeconomic status in Rio de Janeiro, a city located in the Southeastern region (Vitral et al. 1998). This phenomenon can probably be attributed to improvements in sanitary conditions. If this hypothesis is true, then the transmission route of HAV in Brazil may have changed within time. Studying changes in HAV transmission routes in Brazil may therefore elucidate the influence of sanitation on transmission routes. Molecular epidemiological approaches may also be useful for studying transmission routes and provide new information for the control of this disease. Studies carried out in Brazil have shown that two subgenotypes circulate in our country and strains isolated from the same region demonstrated close genetic relatedness (de Paula et al. 2002, 2004, Villar et al. 2004, 2006). In this study, we have analyzed the molecular and epidemiological relationship between HAV isolates recovered from acute cases notified in communities of surrounding region of Rio de Janeiro sampled from 1999 to 2001. PATIENTS, MATERIALS AND METHODS Population study - The county of Belfor Roxo covers 30 Km Northwest of the city of Rio de Janeiro with a population of approximately 435.000 inhabitants. This city is subdivided in five districts (Fig. 1). From December 1999 to December 2001, several cases of acute hepatitis were reported to the epidemiological surveillance of the county of Belford Roxo (ESBRC). All individuals showing clinical signs of hepatitis A (jaundice, fever, dark urine, colure, hepatomegaly abdominal pain) were notified to ESBRC and blood samples were collected. A total of 231 specimens were collected from suspected cases and household contacts aged 0 to 79 years. Sera samples were processed and stored at -20ºC until assays procedures. Symptomatic and asymptomatic hepatitis A acute cases were defined when the serum sample shown positive test for IgM anti-HAV. As part of the active surveillance program, reported index cases are offered hygienic advice and are questioned about possible risk situations that occurred up to six weeks prior to the first day of illness. Also, susceptible contacts are traced and are subsequently offered hygienic advice. To investigate the risk factors for the suspect cases, a case control study was performed, choosing as controls the healthy individuals who were negative for IgM anti-HAV. Demographic and risk factors analyzed were gender, age group, availability of treated water and sewage system; bath practice in rivers, swimming pools, beaches, lagoons or waterfalls, contact with hepatitis infected suspect and sub-district (I-V). For each exposure factor the odds ratio and 95% confidence intervals between cases and controls were calculated using the χ2 test with Yates correction. SPSS version 8.0 was used to perform univariate and multivariate analysis. Formal consent to participate in this study was obtained from all subjects. Serological tests - IgM and total anti-HAV antibodies in sera samples were detected by commercially available ELISA kits (Organon Teknika, Boxtel, The Netherlands) following the instructions of the supplier. Nucleic acid extraction and reverse transcription-polymerase chain reaction (RT-PCR)/Nested RT-PCR - Viral nucleic acid was extracted from 100 µl of IgM anti-HAV antibody positive sera by TRIzol® method as described by Chomczynski and Sacchi (1987) (Life Technologies, Rockville, MD). RT was carried out using 10 µl RNA, 20 pmol of random primers and 200 U of Moloney murine leukemia virus RT (Life Technologies) in a final volume of 20 µl at 37ºC for 1h, followed by 10 min incubation at 65ºC. PCR was performed with VP1/2A specific primers described previously (de Paula et al. 2002). Sequencing and phylogenetic analysis - The nested RT-PCR products were purified using the QIAquick Gel extraction kit (Qiagen, GmbH, Germany) according to the manufacturer. Direct nucleotide sequencing reaction was performed in both directions with a Big Dye Terminator kit (Applied Biosystems, CA, USA) and an automatic DNA sequencer (ABI Prism 310; Applied Biosystems). To construct a phylogenetic tree, sequences from 168 nucleotides (position 3024 to 3191) of VP1/2A junction were aligned using the Clustal X program (Thompson et al. 1997). Afterwards, a matrix was generated for the Kimura-two parameter model (Kimura 1990), and using this matrix and the Neighbor Joining model, a phylogenetic tree was created and her reliability was assessed by bootstrap resampling (1000 pseudo-replicas). These methods were implemented with software from the MEGA program (Kumar et al. 1994). Twenty HAV strains isolated from different regions of the world and isolated from other outbreaks occurred in Rio de Janeiro were included in this dendogram: HAP108 (DQ198361, Brazil), RJ215 (AY323023, Brazil), RJPMC1 (AF410386, Brazil), childA07 (DQ061171, Brazil), childB02 (DQ061160, Brazil), RDJBrasilPA (L07681, Brazil), RJ104 (AY323022, Brazil), RJ12 (AY323034, Brazil), HAS15 (X15464, USA), childD12 (DQ061182, Brazil), RJ055 (AF410384, Brazil), RJNSG2 (AF410383), childA26 (DQ061185, Brazil), HAP279 (DQ198362, Brazil), HAP331 (DQ198360, Brazil), staff006 (DQ061178, Brazil), HM175Australia (M14707, Australia), RJ049 (AY322851, Brazil), RJ005 (AF410381, Brazil), SLF88 (L07729, Sierra Leoa), Nor21 (AF050227, Norway), CF53 (AY644676, France), HAJNG0690F (AB258387, Japan). Sequences obtained in this study are available in Genbank under access numbers DQ438954-DQ438970; EF222210-EF222220. RESULTS Descriptive epidemiology - Between December 1999 and December 2001, 231 serum specimens were collected from 138 suspected HAV cases and 93 household contacts living in a surrounding region of Rio de Janeiro. They were distributed in five districts: I - 19%; II - 22.1%; III - 12.1%; IV - 4.8%; V - 39.8%. Fig. 1 show the time of onset for all acute patients over the two years. The peak of cases was in November 2000 when 11 cases were determined. The population study comprised 120 females and 111 males aging 0 to 79 years (mean = 22.08). Total anti-HAV prevalence was 87.9% (203/231) and IgM anti-HAV prevalence was 38.7% (89/231). IgM anti-HAV detection decreased in individuals aging more than 20 years demonstrating statistical significance (p < 0.00) (Table), IgM positive individuals were most detected in males (56.2%) but it was not statistically significant. Furthermore, IgM anti-HAV was most prevalent in individuals living in district V (42.7%) (Fig. 2). Among 89 hepatitis A acute cases, 32 (40.5%) reported having contact with hepatitis infected suspect, 26 (36.6%) do not have treated water, 47 (61.8%) do not have sewage system availability, 23 (30.3%) related bath practice in rivers, swimming pools, beaches, lagoons or waterfalls during the 2-6 weeks before symptoms onset. Univariate analysis demonstrated that age and bath practices were statistically correlated with hepatitis A infection, while in multivariate analysis only age was statistical significant showing that subjects under 20 years old have more risk to acquire hepatitis A (Table). HAV-RNA detection - HAV-RNA was amplified from 29 (32.5%) IgM anti-HAV positive patients. Among HAV-RNA positive patients, 28 aged less than 20 years old, 15 were contact from index patients, 15 lived at district V, and 18 were males. HAV-RNA detection was not associated with demographic or risk-factor variables (data not shown). Phylogenetic relatedness of HAV isolates - A phylogenetic analysis was carried out to determine the genetic variability degree among 26 the county of Belford Roxo HAV isolates compared to other 22 prototype HAV strains and isolates from state of Rio de Janeiro. All isolates from acute cases notified in the county of Belford Roxo were classified in genotype I, most of them (18/26) belonged to subgenotype IA and the other eight isolates were genotype IB (Fig. 2). Identity among nucleotide sequence of IA isolates varied from 84.9% to 95% and between IB isolates 100% similarity was observed defining a single strain. A comparison of the predicted amino acid sequences of the VP1/2A region from the county of Belford Roxo isolates demonstrated an identity from 86.1 to 100% (data not shown). Co-circulation of both subgenotypes (IA and IB) were observed during January to November 2000. Both subgenotype were detected in all subdistricts except for subdistrict IV in which subgenotype IB was not detected. DISCUSSION This study addressed a community-wide outbreak of hepatitis A in terms of serological and genetic spectrum focusing on demographic and risk factor information as also characterizing isolates sequences among individuals. Total anti-HAV prevalence in this population was 87.8% as it was demonstrated by other researchers in areas where hepatitis A is endemic (de Almeida et al. 2002, Jacobsen & Koopman 2004, Venugopalan et al. 2004). Recent studies have demonstrated a decrease to intermediate and low HAV prevalence in some regions of Brazil due to improvements in hygienic conditions (Vitral et al. 1998, 2006, Clemens et al. 2000, de Almeida et al. 2002, Zago-Gomes et al. 2005). The existence of areas of intermediate endemicity for HAV infection similar to observed in this study may lead to outbreaks as it was described in recent years in Rio de Janeiro (Villar et al. 2002, de Paula et al. 2003, Morais et al. 2006), so vaccination strategy should be revised. In our study, 64% of acute HAV cases were under 20 years old showing that this group represents a higher risk group to acquire HAV infection. Furthermore the risk of acquiring infection in univariate analysis was associated to younger subjects (less than 20 years old) and bath practices showing that person to person transmission and water could be important vehicles of transmission. It is known that water represents an important vehicle (Garin et al. 1994, Villar et al. 2002) and wide-community outbreaks linked to water consumption have been documented (De Serres et al. 2002, Venugopalan et al. 2004). Most of acute HAV cases in this study do not have sewage system (61.8%) which can be one of the factors involved in HAV transmission since the presence of HAV has been detected in this specimen by molecular approaches (Villar et al. 2007). Nevertheless, person to person transmission is also an important mode of transmission responsible for several outbreaks (Robertson et al. 2000, de Paula et al. 2002, Villar et al. 2002) and since the multivariate analysis showed age group as the only risk factor, we could suggest that hygienic habits of younger subjects are the main factor of transmission. In the county of Belford Roxo, 26 HAV isolates had a 168 bp fragment of VP1/2A junction sequenced and most of them (61.5%) belonged to subgenotype IA that comprises over 80% of strains isolated worldwide (Robertson et al. 1992). It was observed a considerable variability degree among isolates of genotype IA as Costa-Mattioli et al. (2001) demonstrated among IA strains isolated during an outbreak occurred in France (Costa-Mattioli et al. 2001). We also observed eight isolates from subgenotype IB in this community with 100% of similarity among each other and to a strain isolated from a sporadic case in Rio de Janeiro (de Paula et al. 2002). Isolates from subgenotype IA and subgenotype IB were closely related to other strains isolated from sporadic cases (de Paula et al. 2002), and outbreak cases that occurred in an orphanage in Rio de Janeiro (de Paula et al. 2003, Morais et al. 2006) and another one that occurred in a public school in the county of Paracambi (Rio de Janeiro) (Villar et al. 2002). In the county of Belford Roxo, subgenotype IB was detected from January 2000 till November 2000 and all isolates shared the same homology suggesting a common source of infection. Subgenotype IA isolates co-circulated with subgenotype IB isolates during march 2000 to November 2000 suggesting that at least two sources of infection were responsible for HAV infection during this period. Co-circulation was previously reported among sporadic cases and outbreaks in Rio de Janeiro (de Paula et al. 2002, 2004, Villar et al. 2004, Morais et al. 2006). This result demonstrates the endemic circulation of some strains in Rio de Janeiro and concomitant circulation of HAV strains at least from two different sources during this outbreak. Epidemiological results demonstrated that age was an independent factor associated to HAV infection and we conclude that person to person transmission associated to the absence of sewage system could be important vehicle of transmission. The association of epidemiological, geographic and molecular data provides information that helps to determine potential contamination sources of HAV infection (Normann et al. 1995, Robertson et al. 2000) and could facilitate the adoption of preventive measures such as vaccine strategies, information about prevention of HAV infection and adoption of hygienic measures, such as sodium hypochlorite distribution. These two last measures were adopted in this county on 2001 and reduced the incidence of HAV infection in this community but vaccination should also be considered especially in individuals aging less than 20 years old to avoid HAV dissemination. ACKNOWLEDGEMENTS To employees of ESBRC for technical assistance and data provided. REFERENCES
Copyright 2008 - Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc08043f1.jpg] [oc08043t1.jpg] [oc08043f2.jpg] [oc08043f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}