 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memórias do Instituto Oswaldo Cruz, Vol. 103, No. 5, August 2008, pp. 417-422 Prevalence and clinical aspects of respiratory syncytial virus A and B groups in children seen at Hospital de Clínicas of Uberlândia, MG, Brazil TFM OliveiraI; GRO FreitasI; LZG RibeiroI; J YokosawaI; MM SiqueiraII; SAR PortesII; HL SilveiraIII; T CalegariIII; LF CostaI; OC ManteseIII; DAO QueirózI, * ILaboratório
de Virologia, Instituto de Ciências Biomédicas Financial support: Fapemig, CNPq, UFU Received 16 November
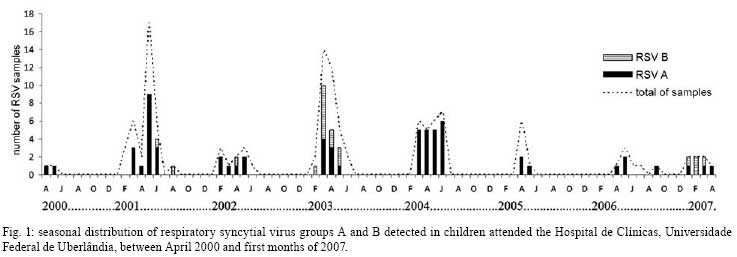
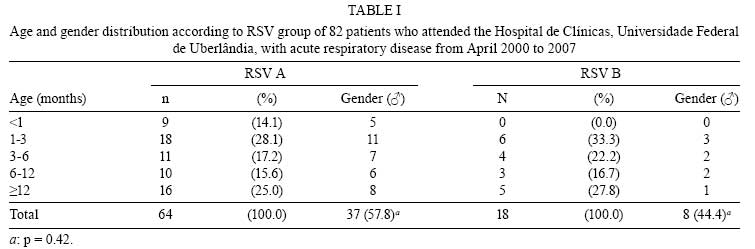
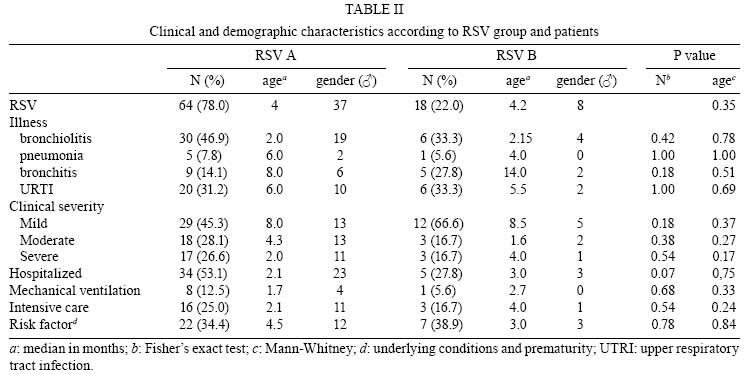
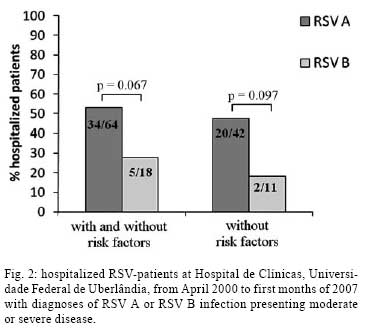
2007 Code Number: oc08074 ABSTRACT Respiratory syncytial virus (RSV) is well recognized as the most important pathogen causing acute respiratory disease in infants and young children, mainly in the form of bronchiolitis and pneumonia. Two major antigenic groups, A and B, have been identified; however, there is disagreement about the severity of the diseases caused by these two types. This study investigated a possible association between RSV groups and severity of disease. Reverse transcription-polymerase chain reaction was used to characterize 128 RSV nasopharyngeal specimens from children less than five years old experiencing acute respiratory disease. A total of 82 of 128 samples (64.1%) could be typed, and, of these, 78% were group A, and 22% were group B. Severity was measured by clinical evaluation associated with demographic factors: for RSV A-infected patients, 53.1% were hospitalized, whereas for RSV B patients, 27.8% were hospitalized (p = 0.07). Around 35.0% of the patients presented risk factors for severity (e.g., prematurity). For those without risk factors, the hospitalization occurred in 47.6% of patients infected with RSV A and in 18.2% infected with RSV B. There was a trend for RSV B infections to be milder than those of RSV A. Even though RSV A-infected patients, including cases without underlying condition and prematurity, were more likely to require hospitalization than those infected by RSV B, the disease severity could not to be attributed to the RSV groups. Key words: Respiratory syncytial virus groups - young children - disease severity Respiratory syncytial virus (RSV) is a common cause of hospitalization and visits to the emergency rooms among neonates and young children, especially in their first years of life (Sangaré et al. 2006). It is the principal cause of bronchiolitis and pneumonia in children under six months of age (Queiróz et al. 2002, Calegari et al. 2005). An RSV infection does not produce substantial immunity to subsequent infection; thus, reinfections are common, with the frequency of symptoms decreasing with age (Black 2003). Sequelae from the RSV infection have been observed, which are mostly persistent wheezing, increased airway hypereactivity or atopic asthma (Simoes 2001). Virtually all infants have been RSV infected by the age of two (Parrott et al. 1974). In the first infection, 40-50% have involvement of the lower respiratory tract, and 1-2% of previously healthy infants develop severe disease requiring hospitalization (Yun et al. 1995). No effective vaccine is currently available for prophylaxis, and ribavirin therapy has presented only modest benefits (Walsh et al. 1997). In addition, younger infants tend to have a prolonged illness with little response to medications in general (Howidi et al. 2007). On the other hand, palivizumab, a humanized monoclonal antibody (IgG1K) directed against an epitope in the A antigenic site of the F protein of RSV, is effective in reducing both the incidence and severity of RSV infections in high-risk infants (Black 2003). Children at the greatest risk of RSV infection include those born prematurely and those with congenital heart disease or chronic lung conditions or immunocompromised (Welliver 2003). Prevention of infection in these infants for as long as possible is particularly important (Black 2003). RSV is a Pneumovirus belonging to the Paramyxoviridae family, with the genome composed of a nonsegmented negative-strand RNA that encodes 11 proteins (Cane 2001). The virus infects the ciliated epithelial cells that line the airways, and their rapid destruction results in the symptoms characteristic of the infection (Black 2003), such as fever, rhinorrhea, cough and wheezing (Park & Barnett 2002) and possibly acute otitis media (Queiróz et al. 2002). RSV isolates are divided into two groups by antigenic and genetic characteristics: A and B (Anderson et al. 1985, Peret et al. 1998). This has led to the speculation that the specific virus group may affect severity and recurrence of the RSV disease (Straliotto et al. 1994). Studies on the clinical aspects associated with each virus group have provide limited information and conflicting results (Walsh et al. 1997, Imaz et al. 2000, Devincenzo 2004); however, it has become important to understand the possible differences in disease severity between subtypes because more therapeutic and prophylactic modalities against RSV have become available, and an understanding of such differences may have an effect on treatment strategies (Papadopoulos et al. 2004). In temperate weather regions, RSV epidemics occur annually in the winter months, whereas in tropical areas, the outbreaks are associated with the rainy season (Cane 2001), and, in semi-tropical areas, the virus circulates mainly during autumn (Vieira et al. 2001, Costa et al. 2006). Both groups circulate concurrently in each epidemic, and group A is the most prevalent in many of the epidemics. Several studies indicate that RSV A and B alternate in prevalence during successive years (Mufson et al. 1988, Sullender 2000). In Brazil, studies have identified the simultaneous circulation of the RSV groups in different years in the Northern (Mello & Silva 1992), Northeastern (Moura et al. 2003), Southeastern (Siqueira et al. 1991, Cintra et al. 2001) and Southern regions (Straliotto et al. 2001), but, to date, no epidemiological pattern for each specific RSV group has been established for Central Brazil. Recently, we reported a study to determine the viral etiology of acute respiratory disease (ARD) in children less than five years of age in Uberlândia (Costa et al. 2006). RSV was the most frequently identified agent in acute lower respiratory infections, accounting for approximately 25% of the cases. The purpose of this study was to determine the RSV group in the samples in which RSV was detected. Moreover, we attempted to establish whether there was a relationship between a specific RSV group and disease severity by analyzing clinical and demographic features of children with confirmed RSV infections. PATIENTS, MATERIALS AND METHODS Patients and specimens - Since April 2000, respiratory viruses have been investigated by indirect immunofluorescence assay (IFA) in nasopharyngeal aspirates (NPA) of children who were less than five years old, experiencing ARD, and attended the Hospital de Clínicas (HC), Universidade Federal de Uberlândia (UFU), state of Minas Gerais, Southeastern Brazil. The study was approved by the ethics committees of UFU and signed consent was obtained from the parents of each child included in this study. Afterwards, a questionnaire was administered to ascertain information about clinical and demographic data, e.g., age, gender, gestational age, clinical symptoms, and risk factors such as immunodeficiency, chronic respiratory disorders (bronchopulmonary dysplasia, cystic fibrosis), congenital heart disease and prematurity. Also, information on any intensive care unit (ICU) hospitalization, requirement of mechanical ventilation and clinical diagnostic criteria such as signs, symptoms, laboratory data, chest radiographs and the pathologies classified according to WHO (1994) were recorded. Hospitalization was required only for those patients presenting moderate or severe disease. Clinical symptoms were divided into: bronchiolitis, bronchitis (laryngotracheobronchitis, bronchospasm, Pertussis-like syndrome, whooping cough, and bronchitis), pneumonia (bronchopneumonia and pneumonia) and upper respiratory tract infection (acute otitis media, rhinitis, sinusitis, flu and upper respiratory tract infection). One milliliter of physiologic solution was instilled into the nostril of patients and NPA was collected within five days of the onset of symptoms for viral diagnosis. Nasal secretions were aspirated through a catheter into a mucus trap, which was connected to a vacuum source. The catheter was inserted into one nostril parallel to the palate. A vacuum was applied, and the catheter was slowly withdrawn with a rotating motion. Mucus from the other nostril was collected in the same manner. NPAs were processed and RSV diagnoses were performed according to Queiróz et al. (2002) using an IFA kit (Respiratory Panel I Viral Screening and Identification IFA, Chemicon Internacional, Temecula, CA). RSV isolation in cell culture - NPAs were inoculated in cell culture (HEp-2 cells; ATCC CCL-23) according to the methods by Queiróz et al. (2002). To confirm the isolation of RSV, regardless of the presence of cytopathic effects, cells were removed from the flasks and tested by an IFA kit, as mentioned above. Cell culture supernatants were used in RT-PCR. Some NPA specimens were not inoculated in cell culture and were tested directly (in natura) by RT-PCR. RSV molecular characterization - The viral RNA was extracted from 250 µ of NPA or 125 µ of RSV-infected HEp-2 cells, using Trizol® (Invitrogen Corp, Carlsbad, CA). Complementary DNA synthesis and PCR amplification were carried out as previously described (Stockton et al. 1998). The primers used for group determination were generated against the N and P regions of the RSV genome, according to the methods by Stockton et al (1998). Ten microliters of each RT-PCR product was separated on a 1.5% agarose gel and photographed with ImageMaster® VDS GE Healthcare, after staining with ethidium bromide. RSV strains Long (group A; ATCC VR-26) and CH18537 (group B; ATCC VR-1580), both as positive controls, and water as a negative control, were run together in each RT-PCR assay to validate the amplification process and to exclude the presence of contaminants. Statistical analysis - Data were analyzed by using the WINKS 4.8a program (TexaSoft, Cedar Hill, TX, USA) with a statistical significance level of p < 0.05. Categorical variables were examined by using the Fisher's exact test (two-tailed) with 95% confidence intervals (CI). For analyses in which the dependent variable was continuous, non-paired Mann-Whitney was used. RESULTS In approximately seven years, we obtained 475 NPAs from children with respiratory disease who attended the HC. Using IFA, RSV was detected in 26.9% (128/475) samples, of which 46 were from the pediatric first aid clinic, 39 were from the emergency room, 13 were from the nursery ward, and 30 were from the pediatric ICU. By using RT-PCR with RNA extracted either directly from NPAs or from isolates in cell culture, it was possible to determine the virus group in 82 out of 128 RSV-positive samples (64.1%); these 82 were further classified into RSV A (78%, n = 64) and RSV B (22%, n = 18). Testing of in natura samples, i.e., NPAs tested directly in the RT-PCR assay, resulted in slightly greater (57.3%) success in determining the RSV group than testing of isolates in cell culture (49.4%), although only three samples needed to be assayed by both methods. Regarding the RSV circulation by subtype, Fig. 1 shows that RSV A was detected in all seven years of the study, while RSV B was detected in only four years (2001, 2002, 2003 and 2007), when it cocirculated with RSV A. Furthermore, RSV B was more prevalent in 2003 and 2007. In general, RSV was detected from January to June (mid-summer to late autumn) with higher incidence of cases from April to May. However, in 2001, one case was detected in August, and, in 2006, one case occurred in September. In terms of gender, 57.8% (37/64) of the RSV A cases were males, compared with 44.4% (8/18) RSV B cases. However, the difference was not statistically significant (p = 0.42) (Table 1). By comparing the age of the patients, RSV A- and B-infected patients presented similar me-dians (4.0 and 4.2 months old, respectively). For RSV A, 59.4% of the patients were < 6 months old, while for RSV B, the rate was 55.6%. However, RSV B was not detected in any patients < 1 month old (Table 1). Bronchiolitis was the clinical diagnosis more frequently observed in RSV A-infected children (Table 2). For clinical severity, RSV B infections tended to be milder than infections with RSV A (p = 0.18), and, except in one case, all children with severe disease were less than six months old. One fatal case was registered of an infant presenting with a RSV A-infection at her 9th day in the ICU. For both the requirement of mechanical ventilation (RSV A: 8/64; RSV B: 1/18) and of ICU hospitalization (RSV A: 16/64; RSV B: 3/18), no statistical difference was observed between the groups. A total of 35.4% (29/82) of the RSV-infected patients presented with prematurity and other underlying conditions (RSV A: 22/64; RSV B: 7/18). Fig. 2 shows that, for the 39 hospitalized patients, 53.1% (34/64) were infected with RSV A, while 27.8% (5/18) were infected with RSV B (p = 0.07; OR 2.95; 95% CI; median age 2.1 and 3.0 months, respectively). When analyzing children without underlying conditions and/or prematurity, hospitalization occurred in 47.6% (20/42) of RSV A cases and in 18.2% (2/11) of RSV B cases (p = 0.10; OR 4.09; 95% CI). In addition, 66.7% (26/39) of the hospitalized patients were males (RSV A: 23/34; RSV B: 3/5) (Table 2). DISCUSSION In this study, we determined the RSV group of specimens collected over approximately seven years from children with respiratory disease. Our results, showing that cases with RSV A predominated over cases with RSV B, are in agreement with the majority of such typing studies (Martinello et al. 2002, Savon et al. 2006). However, one study from 1992 to 1995 in Denmark, reported a predominance of RSV B infections (Johansen et al. 1997). We were able to determine the subtype of approximately 64% of RSV-positive specimens. Uncharacterizeable specimens also occurred in studies by other authors (Straliotto et al. 1994, Walsh et al. 1997, Cintra et al. 2001). Papadopoulos et al. (2004) typed 59.0% using RT-PCR directly from NPA samples, and, in this study, using the same method and the same primers sequences (Stockton et al. 1998), we typed 57.3%. On the other hand, when using RT-PCR in the RSV samples inoculated in cell culture, we were able to characterize 49.4% of RSV samples. This lower rate could be caused by the lack of virus infectivity or replication in the cells that could have arisen from the long period of specimen storage in freezers at -70ºC and/or liquid nitrogen. In addition, it was shown that group B strains tend to grow more slowly in tissue culture, to produce fewer virus particles, and to lose the characteristic of syncytial formation. Therefore, these features could hamper the ability to isolate the virus from clinical specimens and, consequently, the ability to perform group determination (Hall et al. 1990). The detection of RSV B in alternating years is consistent with other studies (Arbiza et al. 2005, Galiano et al. 2005). Mufson et al. (1987) concluded that an infection by RSV A provides some degree of protection against the reappearance by this same group in the subsequent year. The fact that RSV B was not detected in 2005 and 2006 could be because of the few numbers of clinical specimens obtained in those years. Over 20 years ago, Anderson et al. (1985) described the existence of these two groups, the possibility of their occurrence in the same season and their worldwide distribution. It is known that male children are more susceptible to severe disease than females (Burr et al. 1993, Queiróz et al. 2002), but the reasons are still unknown. In our study, the majority of RSV A-infected children were male. This result is consistent with that of Sangaré et al. (2006), who suggested that being female was protective against RSV hospitalization. We also found that RSV A-infected patients tended to be slightly younger (median 4.0 vs. 4.2 years), as previously observed (mean 4.6 vs. 5.1 years) (Imaz et al. 2000), and, in the current study, children less than one month of age were infected solely by the group A. In contrast, based on the mean value of ages observed, Papadopoulos et al. (2004) reported a predominance of RSV B infection in the youngest children. For information on lower tract infections, our data are consistent with those of Garzon and Wiles (2002); they found that bronchiolitis was the most common clinical diagnosis, followed by pneumonia associated with RSV infection. Similar findings were reported by other investigators (Queiróz et al. 2002, Sangaré et al. 2006). Papadopoulos et al. (2004), using duration of hospitalization in the severity index, did not find significant differences between the groups. They stated, however, that the length of hospitalization is based on clinical decisions that cannot be controlled. Considering that including hospitalization in the severity index involves more subjective assessments, this factor was not taken into account in this study. Nevertheless, we observed that patients infected by RSV A were more frequently hospitalized than the patients with RSV B. It has been reported that RSV A was more frequently detected and caused more severe disease than RSV B strains in hospitalized infants (Coates et al. 1963). In relation to disease severity, however, others have reported the opposite (Palomino et al. 2004) or even that there was a lack of evidence for differences between groups (Coggins et al. 1998, Cintra et al. 2001), which was similar to what we observed in this study. Also, it was noteworthy that most of the patients with severe symptoms were less than six months old. This observation was in accordance with the results obtained by Imaz et al. (2000) and Cintra et al (2001). In the comparison of RSV groups with respect to severity of disease, group A infections tended to be slightly more severe than B; however, it was not statistically significant, maybe because of the small sample size or the subjective parameters selected. For instance, more detailed studies of RSV molecular characterization and of the immune response should be done in an attempt to better understand the association with RSV virulence and individual susceptibility. In conclusion, we did not observe statistical differences in clinical severity between the RSV groups, but we observed a trend for RSV B infection to be milder than RSV A. Even though RSV A-infected patients, including cases without underlying condition and prematurity, were more likely to require hospitalization than those infected by RSV B, the disease severity could not to be attributed to the RSV groups. ACKNOWLEDGEMENTS To Dr. Dean D. Erdman (CDC), for providing some reagents; Dr. Juan Arbiza, for useful discussions; the laboratories of Immunology, Molecular Biology, Parasitology, Physiology and Genetics, UFU, for their equipments; the health care professionals of the Hospital de Clínicas; the patients and their parents. REFERENCES
Copyright 2008 - Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc08074t2.jpg] [oc08074g2.jpg] [oc08074t1.jpg] [oc08074g1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}