 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memórias do Instituto Oswaldo Cruz, Vol. 103, No. 5, August 2008, pp. 489-492 Mycobacterium tuberculosis strains of the Beijing genotype are rarely observed in tuberculosis patients in South America Viviana RitaccoI, *; Beatriz LópezI; Patricia I CafruneII; Lucilaine FerrazoliIII; Philip N SuffysIV; Norma CandiaV; Lucy VásquezVI; Teresa RealpeVII; Jorge FernándezVIII; Karla V LimaIX; Jeannete ZuritaX; Jaime RobledoVII; Maria L RossettiII; Afranio L KritskiXI; Maria A TellesIII; Juan C PalominoXII; Herre HeersmaXIII; Dick van SoolingenXIII; Kristin KremerXIII; Lucía BarreraI IInstituto
Nacional de Enfermedades Infecciosas ANLIS Carlos Malbrán, Vélez
Sarsfield 563, 1281 Buenos Aires, Argentina Financial support: European Union (ICA4-CT-2001-10087), CNPq (Prosul 490514/2007), Cyted (207RT0311), EC CP (201690) Received 18 March
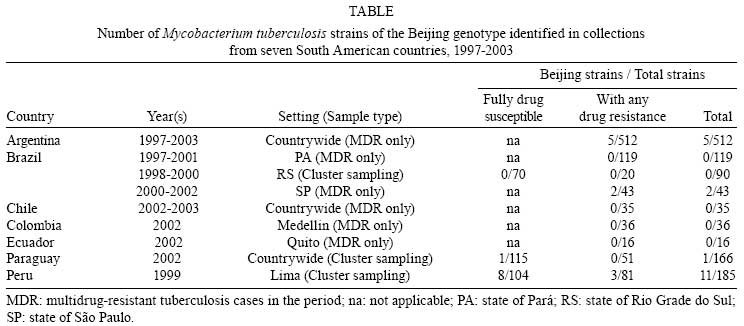
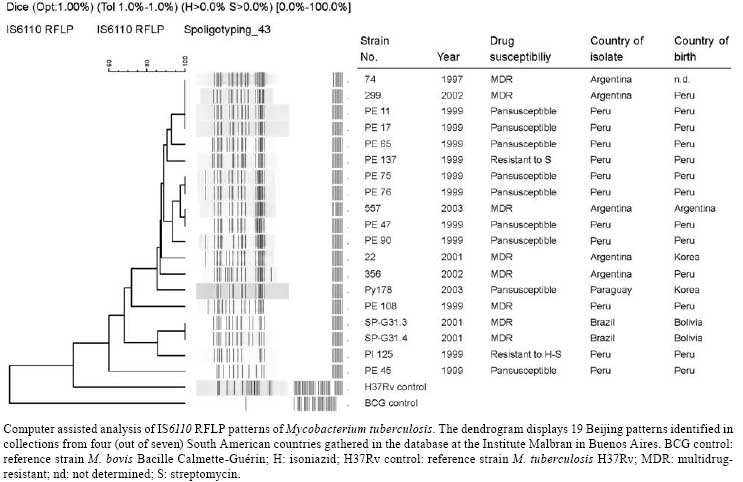
2008 Code Number: oc08086 ABSTRACT The frequency of the Beijing genotype of Mycobacterium tuberculosis as a cause of tuberculosis (TB) in South America was determined by analyzing genotypes of strains isolated from patients that had been diagnosed with the disease between 1997 and 2003 in seven countries of the subcontinent. In total, 19 of the 1,202 (1.6%) TB cases carried Beijing isolates, including 11 of the 185 patients from Peru (5.9%), five of the 512 patients from Argentina (1.0%), two of the 252 Brazilian cases (0.8%), one of the 166 patients from Paraguay (0.6%) and none of the samples obtained from Chile (35), Colombia (36) and Ecuador (16). Except for two patients that were East Asian immigrants, all cases with Beijing strains were native South Americans. No association was found between carrying a strain with the Beijing genotype and having drug or multi-drug resistant disease. Our data show that presently transmission of M. tuberculosis strains of the Beijing genotype is not frequent in Latin America. In addition, the lack of association of drug resistant TB and infection with M. tuberculosis of the Beijing genotype observed presently demands efforts to define better the contribution of the virulence and lack of response to treatment to the growing spread of Beijing strains observed in other parts of the world. Key words: Mycobacterium tuberculosis - genotype - Beijing - Latin America Genotyping has allowed the association of the presence of particular strain families of Mycobacterium tuberculosis and demographic and transmission characteristics of tuberculosis (TB). Strains of the Beijing genotype were first ascribed to be highly prevalent in patients from East Asia (van Soolingen et al. 1995). Shortly after, the contribution of such strains to TB transmission in another region was reported when the W strain of M. tuberculosis that was responsible for an outbreak of multidrug-resistant (MDR) TB in New York city (Bifani et al. 1996) turned out to be of the Beijing genotype. Since then, transmission of TB by strains of the Beijing genotype has been associated with increasing incidence of disease and drug resistant or MDR TB in many parts of the world (ECA 2006). There is scarce knowledge on the contribution of M. tuberculosis of the Beijing genotype to TB transmission in Latin America. Some small outbreaks caused by M. tuberculosis strains of the Beijing genotype have been reported, such as an outbreak of TB in 18 cases diagnosed in a correctional facility in Cuba (Diaz et al. 1998) and the isolation of a strain in 11 cases in the Port of Buenaventura, Colombia (Laserson et al. 1998). Strains of the Beijing genotype were not observed however among isolates obtained from 670 patients from several regions of Venezuela (Aristimuño et al. 2006). Also, recent studies performed in São Paulo and Rio de Janeiro, the main metropolises of Brazil, demonstrated low prevalence of Beijing strains (Telles et al. 2005, Lazzarini et al. 2007). Similar data were obtained from studies in Asunción and Buenos Aires, capital cities of Paraguay (Candia et al. 2007) and Argentina (Morcillo et al. 2005), respectively. To determine the contribution of infection with strains of M. tuberculosis with the Beijing genotype to TB transmission in South America, we searched for Beijing patterns in an M. tuberculosis IS6110 fingerprinting database containing patterns from seven countries in the region. PATIENTS, MATERIALS AND METHODS Patients and strains - We analyzed the genotypes present in a pilot database of M. tuberculosis genotypes created at the Malbran Institute in Buenos Aires aimed to assist the surveillance of MDR TB transmission in the region within the frame of a CA/INCO project of the European Commission. The database contains IS6110 RFLP patterns of M. tuberculosis strains isolated and typed at several TB reference laboratories in Latin America between 1993 and 2006. The M. tuberculosis strains included in this study had been isolated from 1,202 TB patients that were diagnosed between 1997 and 2003 and resided in seven countries of South America, as described in Table. The isolates from Paraguay (n = 166), Peru (185) and the state of Rio Grande do Sul, Brazil (90) came from consecutive cases of smear positive pulmonary TB that were diagnosed as part of surveys for evaluation of drug resistance and had been recruited following cluster sampling procedures according to WHO/IUATLD guidelines (2003). The strains from Chile (n = 35), Argentina (512), Colombia (36), Ecuador (16) and the Brazilian states of São Paulo (3) and Pará (119) came from all the patients with laboratory-confirmed diagnosis of MDR TB in their respective periods. The isolates had been characterized and their drug susceptibility tested at TB reference laboratories (Laboratório Central in Asunción, Paraguay; Instituto Nacional de Salud in Lima, Peru; Laboratório Central do Rio Grande do Sul in Porto Alegre, Instituto Evandro Chagas in Belém, Instituto Adolfo Lutz in São Paulo, Brazil; Instituto de Salud Pública de Chile in Santiago, Chile; Instituto Carlos Malbran in Buenos Aires, Argentina; Corporación de Investigaciones Biológicas in Medellín, Colombia; Hospital Vozandes in Quito, Ecuador). As no additional sampling was performed for the present study, written consent was not required from the patients. Patient information was handled anonymously in accordance with the ethical standards of the committees on human experimentation of the participant institutions and with the Helsinki Declaration of 1964, as revised in 1996 (http://www.wma.net/e/policy/b3.htm). Genotyping and genotype analysis - BioNumerics (Version 4.6; Applied Maths, Sint-Martens-Latem, Belgium) was used for computer-assisted analysis of the IS6110 RFLP patterns obtained by the standardized protocol described by van Embden et al. (1993). In order to pick up the Beijing RFLP patterns in our study population, the latter were compared with the 19 Beijing reference patterns available at the RIVM, The Netherlands, using the Dice coefficient with 1% band position tolerance and 1% optimization (Kremer et al. 2004). A strain was classified as belonging to the Beijing genotype when presenting an IS6110 RFLP pattern with at least 80% similarity to any of 19 selected Beijing reference IS6110 RFLP patterns. In isolates that presented RFLP patterns between 75 and 80% similar to any of the patterns of the 19 reference strains, the classification as Beijing or not was defined by spoligotyping. Spoligotyping was performed as previously described (Kamerbeek et al. 1997). The Beijing strains were defined as those hybridizing to at least three of the spacers 35 to 43 in the absence of hybridization to spacers 1 to 34 in the spoligotyping (Kremer et al. 2004). For cluster analysis, we used the unweighted pair group method using arithmetic averages (UPGMA) and also a 1% band position tolerance and 1% optimization (Heersma et al. 1998). Fisher exact test was used for statistical comparison of categorical variables. RESULTS Out of the IS6110 RFLP patterns from isolates of 1,202 patients examined in this study, 19 presented at least 80% similarity to the pattern of one of the 19 reference Beijing strains. All were confirmed as Beijing by spoligotyping (Figure). Among these, 11 had been isolated in Peru, five in Argentina, two in Brazil and one in Paraguay. Three more isolates had a similarity between 75 and 80% with the reference RFLP fingerprints but none presented the spoligopattern of Beijing strains (data not shown). Upon analysis of data available of the patients that carried Beijing strains, we observed that two cases with different RFLP patterns, one from Buenos Aires and the other from Asuncion were born in Korea and had immigrated when young. The remaining patients harboring Beijing strains were all native South Americans and had apparently no Asian heritage or exposure to overseas sources of infection. Upon cluster analysis of the Beijing RFLP patterns in the strains from our study population, 10 (53%) of the isolates belonged to four clusters, including one cluster of four isolates and three clusters containing each two cases (Figure). The largest cluster was composed of strains isolated from patients that had been diagnosed in Lima and in Cordoba, an Argentinean inland city known to contain a large community of Peruvian immigrants (Figure). One of the other clusters was composed of strains derived from two household contacts in São Paulo, Brazil, both immigrants from Bolivia. No epidemiological linkage was apparent for the patients that had isolates that belonged to the other clusters. Upon comparison of frequency of drug resistant Beijing strains with that of drug susceptible Beijing isolates derived from patients of Lima, Peru, no statistically significant difference was observed between both groups (3/81 vs. 8/104, p = 0.35). DISCUSSION To our knowledge, this is the first study analyzing the frequency of M. tuberculosis strains with the Beijing genotype in South America. Our data are in agreement with earlier studies that included either a small number of patients or TB cases diagnosed in a single setting (Morcillo et al. 2005, Telles et al. 2005, Aristimuño et al. 2006, Mancilla et al. 2006, Candia et al. 2007, Lazzarini et al. 2007), confirming the low prevalence of strains of this family in South American countries (Vazquez et al. 2004). Interestingly, 68% (13/19) of the Beijing isolates observed presently were from Peruvian patients (11 living in Peru and 2 in Argentina; Figure). Our data seem to be in agreement with the reports by two independent research groups, demonstrating the importation of Beijing strains into Spain by Peruvian immigrants (Codina et al. 1999, García de Viedma et al. 2006). It is therefore tempting to speculate that M. tuberculosis strains of the Beijing genotype were introduced into Peru and eventually into other South American countries when the former country received a significant number of Chinese immigrants who settled as coolies in mid XIX century. Although we admit that our study is limited by a small sampling size, the considerable diversity of the IS6110 RFLP patterns combined with the low frequency of Beijing isolates supports the idea of earlier introduction of different ancestors. Different migration waves from East Asian countries might have contributed to the introduction of Beijing strains into the South American territory throughout the past 150 years. Evaluation of other genetic markers that determine the relation of Beijing strains is currently being performed. The modest role of the Beijing genotype in the epidemiology of TB in the region we studied presently is illustrated by the lack of association of drug resistance with Beijing in the Peruvian and Paraguayan isolates. This seems to be in agreement with the meager contribution of Beijing M. tuberculosis strains to the burden of MDR TB in Argentina where a few non-Beijing M. tuberculosis strains that caused major MDR TB outbreaks a decade ago still prevail over other MDR M. tuberculosis strains in the country (Palmero et al. 2003, 2005). Our data were obtained from a database that was created as part of a pilot study for evaluation of genotyping as an additional tool for management and surveillance of spreading of drug resistant and MDR TB. Among the laboratories that contributed to the construction of this database, some focused on surveillance of MDR TB while others evaluated all consecutive acid fast bacilli smear positive cases as observed during a certain time frame. The heterogeneity in sampling procedures certainly reduces the accuracy of genotype frequencies observed in this study. In addition, the small sample size could have contributed to the absence of strains with the Beijing pattern in native Brazilian, Paraguayan, Colombian, Ecuadorian and Chilean patients and we might have overseen sporadic cases or outbreaks due to Beijing strains. Nonetheless, other studies that present Beijing strains as a significant contributor to TB and MDR TB transmission often suffer from the same limitations. REFERENCES
Copyright 2008 - Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc08086f1.jpg] [oc08086t1.jpg] |
| |||||||||

{kind=link}
{kind=link}