 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memórias do Instituto Oswaldo Cruz, Vol. 103, No. 7, November, 2008, pp. 661-667 ARTICLES Comparison of serological responses in two different populations with pulmonary tuberculosis Zaida AraujoI, +; Francesca GiampietroI; Lucio Castellano CançadoII; Mahavir SinghIII; Albina WideIV ILaboratorio
de Inmunología de Enfermedades Infecciosas, Instituto de Biomedicina Financial support: FONACIT (S1-2000000667), BIOLAC/UNU Received 10 April
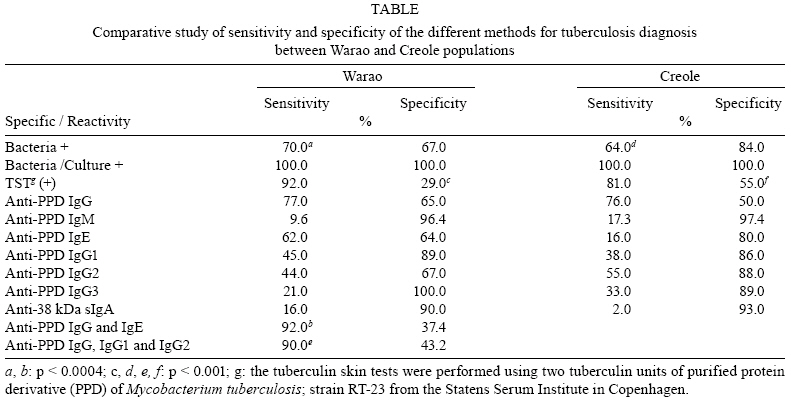
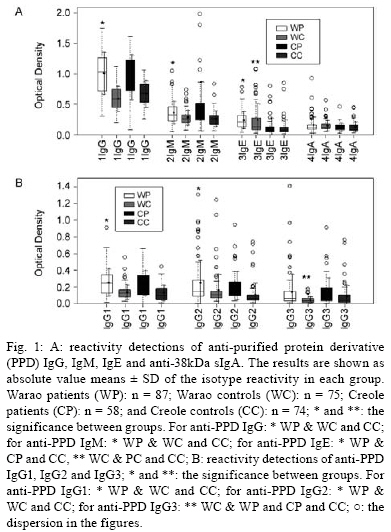
2008 ABSTRACT Observational studies on the humoural immune responses of the Warao indigenous people from Delta Amacuro, an isolated area, were compared with urban residents of the Venezuelan capital. Mycobacterium tuberculosis-specific reactivities (IgM, IgE, sIgA, IgG and IgG subclasses) were measured by ELISA using PPD and 38-kDa M. tuberculosis antigens. A total of 294 individuals were studied, 162 Warao (indigenous people) and 132 Creole (non-indigenous people). The patient group consisted of 87 Warao patients and 58 Creole patients, while the control group consisted of 75 Warao controls and 74 Creole controls. Combinations among the isotypes studied were performed. The findings showed that for the Warao people, sensitivity to the combination including anti-PPD IgG and IgE was 92.0%, while for the Creole people, sensitivity to the combination including anti-PPD IgG but more so anti-PPD IgG1 and IgG2 was 90.0%. Simple tests were able to show higher specificities, which were population-specific; specificities were anti-PPD IgG3, 100.0% and anti-PPD IgM, 97.4% for the Warao and Creole peoples, respectively. In conclusion, while simple tests reached high specificity, the multi-isotype tests improved sensitivity; the latter shows this approach may be useful in diagnostic testing. Key words: tuberculosis - Warao - Creole - IgG subclasses - purified protein derivative - diagnosis Tuberculosis (TB) diagnosis needs to be improved, as it largely depends upon clinical examination and radiographic findings, mainly confirmed by sputum smear microscopy and bacterial culture (Murray et al. 1980). The latter requires a long cultivation period and diagnostic confirmation still relies on sputum smear examinations. Many alternative methodologies have been applied in TB diagnosis, such as western blot, microscopic observed direct sensitivity culture, PCR and cell-mediated immune response reactions (Moore et al. 2006, Negi et al. 2006). These methods require trained personnel and specific laboratory conditions, which hinder their implementation in many areas of high TB endemicity (mainly low-income countries) and field work application. On the other hand, there are other options that are currently under evaluation, including antibody detection by serology. While specific antibody detection by serology is under evaluation for a definitive demonstration that the humoural response can be used as a tool for the diagnosis of TB, future studies should be carried out in order to combine serological and cellular methods, such as T.SPOT-TB or Quantiferon Gold assay, which are considered to be approved tools. Regarding the immunodiagnosis of TB based on the T cell response to ESAT-6 and purified protein derivative (PPD) antigens, recently it has been reported that the IFN- assay using ESAT-6 as an antigenic stimulus has the potential to be used as a tool for the immunodiagnosis of early TB in children (Van-Lume et al. 2008). The demand for a rapid, reliable, cost-effective and easy TB diagnostic tool focuses on antibody detection by serology (Bothamley 1995). It has been reported that the isotypic restriction of antibodies correlates with the biochemical nature of antigens; most antibodies against proteins are of IgG1 and IgG3 isotypes, while in those against carbohydrates IgG2 is over-represented (Chiang et al. 1997, Gupta et al. 2005). This is reflected in vivo where, for instance, antibody responses to viral proteins are mainly of the IgG1 and IgG3 subclasses. In contrast, bacteria carbohydrates usually induce type 2 T-independent responses, mainly of the IgG1 and IgG2 isotypes. Several ELISA tests have been attempted and results have presented a large variability in their accuracy depending on the antigen employed (one alone or a pool) (Chiang et al. 1997, Gupta et al. 2005), the immunoglobulin (Ig) class, the subclass measured (Radin et al. 1983, Daniel & Debane 1987, Pottumarthy et al. 2000, Conde et al. 2004, Imaz et al. 2004) and Mycobacterium tuberculosis strain variation (Alde et al. 1989, Zheng et al. 1994, Raja et al. 2002). This indicates either that other antigens need to be assessed for diagnosis or it reinforces the idea of differential antibody responses due to genetic ethnic variation (Demkow et al. 2004, Weldingh et al. 2005). In the latter, few studies have addressed the importance of the antibody response due to a different genetic background. Official data on the TB situation in Venezuela showed that between 1997-2001, the TB rate was between 93.2-81.0 per 100,000 inhabitants among the Warao people (MSAS 1999, Fernandez de Larrea et al. 2002, MSDS 2002). Both the Warao and Creole peoples have been tested for the human leukocyte antigen (HLA), HLA-A, B, HLA-Cw, HLA-DR and HLA-DR/DW 1-8 antigens. For the Warao, the findings confirmed the existence of the DR/DW dissociation previously observed in North American Indian, Japanese and Caucasian populations and showed inheritance and segregation of DW specificities (DW 8.3, DW 16, DW 22) defined only with homozygous typing cells of Warao origin. These data illustrated HLA haplotypes, linkage-disequilibrium and DR/DQ associations not seen previously in other human populations (Araujo et al. 2003). Data regarding the HLA class I and class II allele and haplotype distributions among Venezuelan Creoles showed that genes of Mongoloid, Negroid and Caucasoid origin have created a distinctive HLA genetic profile in this hybrid Creole population. The predominant HLA-B DQA1 DQB1 DRB1 haplotype is HLA-B44 DQA1*0201 DQB1*0201 DRB1*0701 (5.3%). It is noteworthy that the HLA-A3 B7 DR2 and the HLA-A1 B8 DR3 linkage groups are part of conserved or ancestral haplotypes (Makhatadze et al. 1997). In order to study the serological response in two populations with different genetic backgrounds, in the present work saliva IgA (sIgA) and serum IgM, IgE, IgG and IgG1, IgG2 and IgG3 subclass reactivities were measured against M. tuberculosis antigens in the Warao and Creole peoples. PATIENTS, MATERIALS AND METHODS Study population and clinical and epidemiological criteria - A prospective trial was performed, which included the Warao indigenous people, a population in a rural area isolated from contact with the tubercle bacillus for millennia until the mid-1960s. Within the Warao population, a high prevalence of active TB is observed, indicating a high susceptibility to disease, even among bacille Calmette-Guerin-vaccinated individuals. The humoural immune response of the Warao was compared with individual residents of the capital of Venezuela (urban area), the Creoles. A total of 294 adults aged from 15-60 years were studied: 162 Warao and 132 Creoles living in rural and urban areas, respectively. Individuals were grouped according to patient group: Warao patients (WP, n = 87), and Creole patients (CP, n = 58). These individuals had TB disease activity, where the clinical evaluation included recent weight loss or inadequate progress of weight gain, prolonged febrile syndrome, night sweats and coughing or wheezing for more than two weeks. The control group consisted of Warao healthy controls (WC, n = 75), and Creole healthy controls (CC, n = 74). These were individuals with lack of symptoms or without TB disease activity. The tuberculin skin test (TST) was performed on all the individuals of this study by a similar test previously described. The criterion for positive test reactivity was based on measurements of induration values ≥10mm (Snider 1982, Arnadottir et al. 1996). For the confirmatory diagnosis of TB, smears from sputum were stained by the Ziehl-Neelsen direct method. For each sputum specimen, two tubes of modified Ogawa egg medium and Lowënstein-Jensen were inoculated, using the swab method of Kudoh and Kudoh (1974). Vaccination status was inferred from the presence of BCG scars; in Venezuela, the vaccination program has been conducted by the Tuberculosis National Program, which recommends the BCG immunization international policies, namely one dose of vaccine at the age of 0-5 years old. Exclusion criteria included: (1) patients and healthy controls who are HIV positive; (2) patients taking immunosuppressive drugs (e.g., corticosteroids, azathioprine and cyclophosphamide) and (3) participants who did not sign an informed consent agreement. Specific treatments were initiated in all newly identified cases of TB following the norms of the Tuberculosis National Program (MSAS 1999, MSDS 2002). This study was approved by the Ethical Committee of the Biomedicine Institute, Central University of Venezuela, (protocol number 2000000667/18/06/99) and written informed consent was voluntarily signed by all patients and control individuals. Multiple Antigen Blot Assay (MABA) - MABA test was used to confirm mycobacteria-PPD and 38-kDa as antigens for the purposes of studying the isotype reactivities (Noya & Alarcón 1998). Briefly, MABA permits the simultaneous screening of different antigens, saliva or sera based on a dot-blot ELISA test. Using an acrylic device (Minibloter® 28 S-L Immunetics Inc, Cambridge, MA, USA) containing at least 12 parallel troughs, antigens were distributed and immobilized onto a nitrocellulose membrane. Strips were cut perpendicularly and exposed to immune samples (sera and saliva diluted 1:400 and 1:10, respectively) for 1 h at 37°C. Then these were washed four times and then incubated for 1 h at 37°C with peroxidase-conjugated monoclonal antibody anti-IgG-gamma chain (Promega Corporation, USA) and peroxidase-conjugated monoclonal antibody anti-alpha chain IgA (Sigma-Aldrich, USA), which were used as the second antibodies. The reaction was developed by a chemiluminescent substrate, the results being recorded on film. Positive reactions to the different antigens are seen as small black squares on each strip. Anti-PPD IgG, IgM and IgE tests - ELISA was performed for the measurement of antibodies (IgG, IgM and IgE) against PPD as previously reported (Araujo et al. 2004). Briefly, the levels of anti-PPD IgG, IgM and IgE were determined in serum by an ELISA as follows. Sera were isolated from venous blood obtained from controls and TB patients. Microtiter plates (Immunolon, Birmingham, UK) with 96 wells were coated with PPD (Statens Seruminstitut, Copenhagen), (1 µg/well of each antigen in carbonate-bicarbonate buffer pH 9.6) overnight at 4°C. Excess protein binding sites were blocked by incubation with 1% BSA in PBS at 37°C for 1 h. Samples diluted 1:400 (for anti-PPD IgG) and 1:50 (for anti-PPD IgM and IgE) in PBS containing 0.5% BSA were added and plates were incubated for 1 h at 37°C. The plates were washed four times, then incubated with the secondary antibodies: anti-human IgG HRP-conjugate (Promega Corporation, USA), anti-human IgM HRP-conjugate (PIERCE Biotechnology) and anti-human IgE biotin-labelled (Vector Laboratories), incubated for 1 h at 37°C and washed four times. Substrate solution (30 µL of 30% H2O2 and 10 mg o-phenylenediamine dihydrochloride, Sigma-Aldrich, USA) in 25 mL citrate buffer, pH 5 was added and incubated for 6 min at rt. Colour development was measured in an ELISA reader at 492 nm. Anti-38 kDa sIgA - The levels of sIgA in saliva were determined by a similar ELISA to that described for serum anti-PPD IgG. Microtiter plates were coated with 38 kDa antigen (GBF and LIONEX GmbH, Braunschweig, Germany) overnight at 4°C (1 µg/well of each antigen in carbonate-bicarbonate buffer pH 9.6). The saliva samples were diluted 1:10 and monoclonal antibody anti-human IgA peroxidase-conjugate (Sigma-Aldrich, USA) was used as the secondary antibody. Anti-PPD IgG subclasses - The levels of anti-PPD IgG1, IgG2 and IgG3 subclasses were determined by a similar ELISA to that described for serum anti-PPD IgG. Briefly, microtiter plates (Immunolon, Birmingham, UK) with 96 wells were coated with PPD antigen (1µg/well). The serum samples were diluted 1:50 and peroxidase-conjugate monoclonal antibodies anti-human IgG1, IgG2 and IgG3 (AP006, AP007 and AP008, The Binding Site, UK) were used as the secondary antibodies. Other serological markers - HIV diagnostic testing was done with the Passive Particle Agglutination Test for the detection of antibodies to HIV-1 and/or HIV-2 from FUJIREBIO Diagnostics (Abbott? Laboratorie, Dainabot Co Ltd, Tokyo, Japan). Statistical analysis - The statistical test used to compare the significance of the differences between the percentage values of individuals positive and negative for the TST was the Fisher's exact test. The reactivity was measured by enzyme linked immunosorbent assay and the differences in the isotype reactivity for each group were compared and evaluated using an unpaired Student's t test; p values < 0.05 were considered significant. R Development Core Team (2008) was used to highlight the outliers for showing the dispersion in the figures. RESULTS Bacteriological studies - The sensitivities of the smears were 70.0% and 64.0% for the Warao and Creole peoples, respectively, while culture test showed a sensitivity of 100.0% (Table). Delayed type hypersensitivity and BCG vaccination status - There was no statistically significant difference in relation to the TST reactivity between the WP (80/87) and CP (47/58) groups. However, within control groups, the WC group (53/75) showed higher TST reactivity than the CC group (34/74) (p < 0.001) (Table). The findings regarding the BCG vaccination status between the groups suggests that BCG vaccination does not have a significant effect on the incidence of the TST response (data not shown). Reactivity response - The means of optical density ± deviation density of the anti-PPD IgG, IgG subclasses, IgM, IgE and anti-38kDa sIgA reactivities are shown in Fig. 1. The anti-PPD IgG showed higher reactivity in serum and anti-sIgA 38-kDa in saliva when MABA was used to select the antigen for studying the isotype reactivity (data not shown). The anti-PPD IgG reactivity evaluation showed that WP presented higher reactivity (1.010 ± 0.348) than respective controls, WC (0.592 ± 0.139) and CC (0.669 ± 0.222) (p < 0.0001) (Fig. 1A). Also for anti-PPD IgM reactivity, it was observed that WP presented a significantly higher reactivity (0.365 ± 0.193) than respective controls, WC (0.281 ± 0.074) and CC (0.264 ± 0.133) (p < 0.0005 and p < 0.0002, respectively) (Fig. 1A). Concerning the IgE antibody response, serum anti-PPD IgE reactivity analysis showed that the Warao people reacted more than the Creole people, independently of whether they were patients or controls (Fig. 1A), WP (0.241 ± 0.146) and WC (0.247 ± 0.033) than CP (0.127 ± 0.035) and CC (0.115 ± 0.136) (p < 0.0001) (Fig. 1A). Regarding anti-38kDa sIgA reactivity, a statistically significant difference was not observed between the groups (Fig. 1A). Serum anti-PPD IgG1 analysis showed that WP presented a significantly higher IgG1 reactivity (0.255 ± 0.167) than WC (0.140 ± 0.156) and CC (0.130 ± 0.096) (p < 0.0001) (Fig. 1B). For anti-PPD IgG2 reactivity, it was observed that WP presented a significantly higher IgG2 reactivity (0.255 ± 0.267) than respective controls, WC (0.165 ± 0.159) and CC (0.111 ± 0.142) (p < 0.001 and p < 0.0001, respectively) (Fig. 1B). There was no anti-PPD IgG3 reactivity in WC (0 ± 0) as compared to WP (0.142 ± 0.0.219), CP (0.145 ± 0.108) and CC (0.090 ± 0.137) ( p < 0.0002, p < 0.0001 and p < 0.005, respectively) (Fig. 1B). The antibody reactivity to M. tuberculosis antigens after and before treatment is shown in Fig. 2. We observed a statistically significant difference between anti-PPD IgG reactivity after treatment (0.576 ± 0.205) and before treatment (0.902 ± 0.072) (p < 0.008) (Fig. 2A). For anti-PPD IgE, the higher reactivity found after treatment (0.669 ± 0.465) was statistically significant compared to before treatment (0.225 ± 0.184) (p < 0.02) (Fig. 2A). There was not a statistically significant difference concerning anti-PPD IgM, anti-PPD IgG1, anti-PPD IgG3 and anti-38-kDa sIgA reactivities after treatment as compared to before treatment (Fig. 2A), while we did observe a statistically significant difference between anti-PPD IgG2 reactivity after (0.100 ± 0.026) and before treatment (0.267 ± 0.008) (p < 0.0001) (Fig. 2B). Sensitivity and specificity tests - The sensitivity and specificity of the different methods are shown in the Table. We observed high specificity between the methods, two methods were especially highly specific, anti-PPD IgG3 and anti-PPD IgM (100.0% in the Warao people and 97.4%, in the Creole people, respectively) (Table). However, we found low sensitivity between the methods, anti-38 kDa sIgA (2.0% in the Creole people) and anti-PPD IgG (77.0% in the Warao people). Among the combinations performed among all isotypes, in the Warao people the anti-PPD IgG and anti-PPD IgE combination and in the Creole people, the anti-PPD IgG, anti-PPD IgG1 and anti-PPD IgG2 combination detected the largest number of patients which brought an improved sensitivity level of 92.0% and 90.0%, respectively, even though specificity levels dropped to 37.4% and 43.2%, respectively (Table). In both patient groups, there were statistically significant differences between the sensitivities of the combination methods and the smear methods, 92.0% versus 70.0%, p < 0.0004, and 90.0% versus 64.0%, p < 0.001, in the Warao and Creole groups, respectively (Table). DISCUSSION The present work tried to reinforce the use of multi-antigen and multi-isotype assays as the central rationale to develop a test for TB to be used effectively in different settings in Venezuela. The findings showed that combinations among the isotypes studied improved the sensitivity, even though the specificity dropped to lower levels; for the Warao people, sensitivity of the combination including anti-PPD IgG and IgE was at 92.0%, while for the Creole people, sensitivity of the combination that included anti-PPD IgG but more so anti-PPD IgG1 and IgG2 was at 90.0%. In contrast, simple tests were able to show higher specificities, which were population-specific, anti-PPD IgG3 (100.0%) and anti-PPD IgM (97.4%) for the Warao and Creole peoples, respectively. Regarding the IgG specific response, the results showed that the anti-PPD IgG responses were serologically indistinguishable between Warao and Creole untreated TB patients. These results are in concordance with studies showing that patients with active TB clearly had higher levels of IgG antibody to PPD antigen than did a healthy control group (Radin et al. 1983, Hussain et al. 1995). It has been proposed by the WHO that new diagnostic methods should have sensitivity at least higher than bacilloscopy (WHO 2003). The sensitivities of the microscopic examination of sputum for acid-fast bacilli were statistically low in the WP and CP groups as compared to the combination methods. In a previous study conducted with Warao children, we found for anti-PPD IgG a low sensitivity of 38.2% and a high specificity of 95.8% (Araujo et al. 2004). One report describes the high and low sensitivity of anti-PPD IgG test (Lyashchenko et al. 1998); these different findings can be explained since it has been reported that serum IgG antibodies are produced against a variety of epitopes on the antigen surface. Also, the number and the species of serologically reactive antigens varied greatly from individual to individual, and the level of specific antibodies could also vary with the genetic background or the age of individuals (Lyashchenko et al. 1998). The anti-PPD IgM methods showed low sensitivities, while specificities were higher for both populations. The latter correlates with the results reported on the commercial methods, which use recombinant mycobacterial antigens. These commercial methods available for TB serological diagnosis based on IgM reactivity show lower sensitivity rates for both adults and children than tests based on other antibody classes, although specificity has remained at elevated rates (Pottumarthy et al. 2000, Imaz et al. 2004). The anti-38kDa sIgA method was included in our study due to the fact that it provided an improvement in the diagnosis of TB in Warao children (Araujo et al. 2004). A combination including anti-PPD IgG, IgE and anti-38kDa sIgA detected a larger number of child patients and allowed us to obtain a sensitivity level of 64.7% and a specificity of 81.8% (Araujo et al. 2004). In the present study a major percentage of WP elicited saliva positive reactivity, anti-38kDa sIgA, as compared to the Creole people; these methods were not very sensitive, but highly specific. These findings correlate with previous results obtained in Warao children, where the anti-38kDa sIgA method showed high specificity and low sensitivity (Araujo et al. 2004). Few studies have addressed anti-38kDa sIgA reactivity, although it has been reported to have sensitivity around 80% using the 38-kDa antigen to test sera samples instead of saliva (Young et al. 1986, Uma et al. 2001). Regarding the anti-PPD IgG subclass reactivities, higher percentages of both WP and CP showed anti-PPD IgG1 and IgG2 reactivities than control groups; the latter was highly reactive in the Creole people as compared to the Warao people. It has been reported that antibody responses to bacterial carbohydrates are mainly of the IgG1 and IgG2 subclasses (Gupta et al. 2005). The importance of IgG2 in human TB is not evident; the authors reported that a few cases of active TB showed moderately increased IgG2, while in relapse and chronic TB cases with reactivity to IgG2 these levels were decreased. Therefore, IgG2 subclass could not differentiate between TB cases and healthy controls with latent infection (Gupta et al. 2005). The latter was not in concordance with our results for the Warao people, as WP presented a significant higher reactivity than the respective control groups studied. The present results regarding anti-PPD IgG3 reactivity are in concordance with a report that shows that in TB patients, both anti-PPD IgG1 and IgG3 tests reacted more often than in controls (Hussain et al. 1995, Gupta et al. 2005). Within the Warao people, the anti-PPD IgG3 method showed the highest specificity at 100%, even though sensitivity levels dropped to 21%. These findings suggest that there is no basis for a useful diagnostic test, but it could be of use in confirming that no TB cases among the people from this population resulted from false positive cases. When IgG, IgM, sIgA and IgG subclass reactivities were evaluated before and after treatment in the Warao population, it was found that two of these, IgG and sIgA, were affected by anti-TB treatment. The results permit us to suggest that these isotypes are markers of active infection and could be predictive of treatment outcome in this population, such as has been reported by others authors, who have suggested that the levels of antibodies to M. tuberculosis represent serological correlates of active disease since these were affected in an antigen-specific fashion by anti-TB treatment (Azzurri et al. 2006). Since it is known that poor sensitivity tests may be due to substantial and unexplained heterogeneity of the humoural response to M. tuberculosis (Hussain et al. 1995), it seems probable that the development of either multi-antigen tests or multi-isotype tests could optimize both sensitivity and specificity. The present findings showed that the combination methods were able to optimize sensitivity; for the Warao people, sensitivity of the combination including anti-PPD IgG and IgE was at 92.0%, while for the Creole people, sensitivity of the combination including anti-PPD IgG but more so anti-PPD IgG1 and IgG2 was at 90.0%. In contrast, simple tests were able to show higher specificities, which were population-specific, with anti-PPD IgG3 at 100.0% and anti-PPD IgM at 97.4% for the Warao and Creole people, respectively. In a report on the antibody responses to CFP-21, ESAT-6, MPT-63 and MPT-64 antigens, it was found that sensitivity to the multi-antigen complex was higher than for the four single antigens and that the specificity was at 100% (Wang et al. 2005). The combination methods utilized in the present study should be extended to other TB endemic regions of Venezuela for the evaluation of both the sensitivity and specificity of the methods. Taking into account that the combination methods included PPD, a crude antigen that is present in other Mycobacterium species, such as non TB mycobacteria and Mycobacterium leprae, further studies testing in parallel patients with leprosy and using different antigens such as rESAT-6 or rAg85 are necessary. In addition, these methods must be combined with any of the sensitive and approved tools, such as IFN- release assay, T.SPOT-TB or Quantiferon Gold assay; if these tests are in agreement with the methods studied here, it could reinforce the use of the multi-antigen and multi-isotype tests performed in this study. Finally, while the multi-isotype methods improved sensitivity, simple methods allowed for maximum specificity to be obtained. Since our results show that both a combination method and a simple method yield different responses in specific populations, the variability of the humoural immune response to M. tuberculosis must be taken into account in order to optimize sensitivity, especially in populations with different genetic backgrounds. ACKNOWLEDGEMENTS To Komal Roy Siripaul, for critical review of the manuscript. REFERENCES
Copyright 2008 - Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc08120f2.jpg] [oc08120t1.jpg] [oc08120f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}