 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memórias do Instituto Oswaldo Cruz, Vol. 104, No. 2, March, 2009, pp. 383-388 Prevalence of acute toxoplasmosis infection among 41,112 pregnant women and the mother-to-child transmission rate in a public hospital in South Brazil Ivana S VarellaI, +; Ivete CT CantiI; Breno R SantosI; Angela Z CoppiniI; Luciana C ArgondizzoI; Carina ToninI; Mário B WagnerII IHospital
Nossa Senhora da Conceição, Grupo Hospitalar Conceição,
Porto Alegre, RS, Brasil Received 10 October
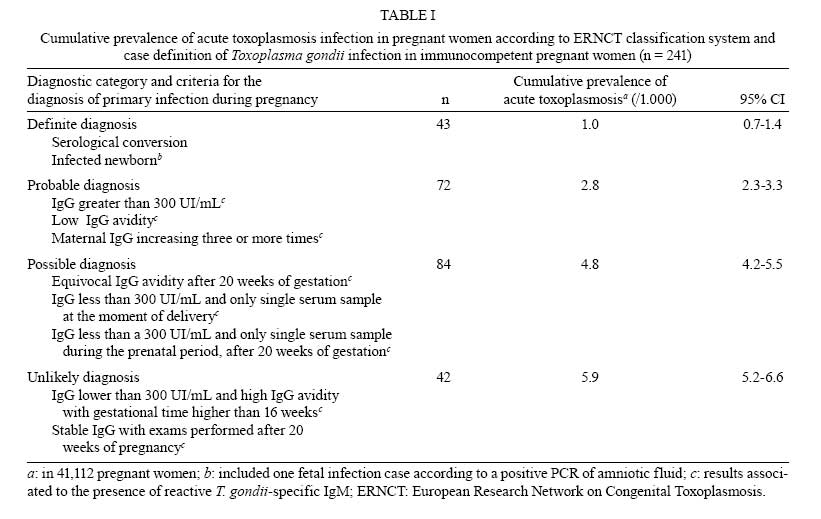
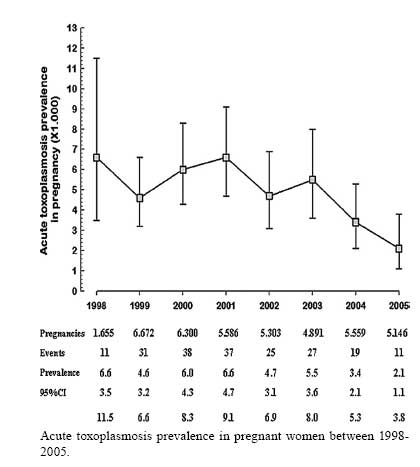
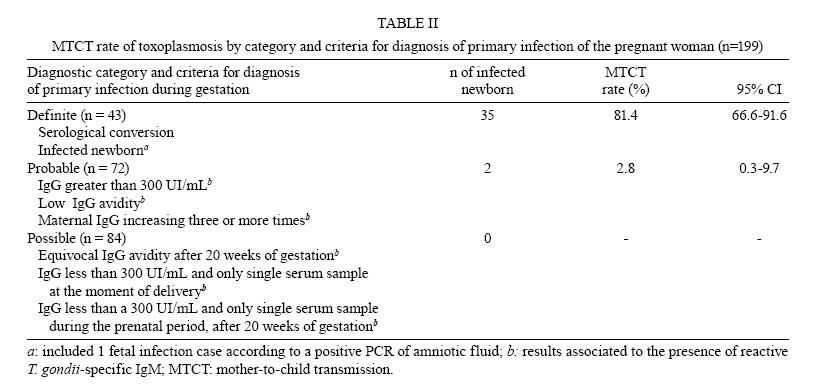
2008 Code Number: oc09060 ABSTRACT Untreated acute toxoplasmosis among pregnant women can lead to serious sequelae among newborns, including neurological impairment and blindness. In Brazil, the risk of congenital toxoplasmosis (CTox) has not been fully evaluated. Our aim was to evaluate trends in acute toxoplasmosis prevalence from 1998-2005, the incidence of CTox and the rate of mother-to-child transmission (MTCT). A cross-sectional study was undertaken to dentify patients who fit the criteria for acute toxoplasmosis during pregnancy. Exposed newborns were included in a historical cohort, with a median follow-up time of 11 months, to establish definite diagnosis of CTox. Diagnoses for acute infection in pregnancy and CTox were based on European Research Network on Congenital Toxoplasmosis criteria. In 41,112 pregnant women, the prevalence of acute toxoplasmosis was 4.8/1,000 women. The birth prevalence of CTox was 0.6/1,000 newborns [95% confidence interval (CI): 0.4-0.9]. During the follow-up study, 12 additional cases were detected, increasing the CTox rate to 0.9/1,000 newborns (95% CI: 0.6-1.3). Among the 200 newborns exposed to Toxoplasma gondii,there were 37 babies presenting diagnostic criteria of CTox, leading to an MTCT rate of 18.5% (95% CI: 13.4-24.6%). The additional cases identified during follow-up reinforce the need for serological monitoring during the first year of life, even in the absence of evidence of congenital infection at birth. Key words:toxoplasmosis - congenital toxoplasmosis - pregnancy Untreated acute toxoplasmosis among pregnant women can lead to infection of the foetus via transplacental transmission. Although newborns affected by congenital infection may seem normal upon first examination, serious sequelae, such as neurological impairment and blindness, can develop a few years later (Mombro et al. 1995, Dunn et al. 1999, Safadi et al. 2003, Remington et al. 2005). In high risk areas, serological screening has been recommended to identify susceptible individuals in order to adopt primary preventive measures (Foulon et al. 1988). Some reports have suggested that pregnant women diagnosed with acute toxoplasmosis should be treated as soon as possible to reduce the risk and severity of congenital infection (Foulon et al. 1999, Gilbert et al. 2001, Gras et al. 2005). Others have argued that there is still no treatment capable of reducing vertical transmission (Foulon et al. 2000, Peyron et al. 2000, Gilbert et al. 2001). Nevertheless, a recent meta-analysis reported that a maternal treatment started within three weeks of seroconversion had a small effect in the reduction of vertical transmission when compared to treatments that were started eight or more weeks after seroconversion (Thiebaut et al. 2007). Incidence studies of acute toxoplasmosis around the world have found rates per 1,000 pregnancies of 0.5 in Sweden (Evengard et al. 2001), 1.7 in Norway (Jenum et al. 1998), 2.1 in Denmark (Lebech et al. 1999), 2.0 in New York, USA (Lopez et al. 2000), 6.6 in Paris, France (Remington et al. 2005), and 8.5 in Belgium (Naessens 2003). In Brazil, there is no established epidemiological surveillance program for toxoplasmosis among pregnant women. Despite that, the prevalence of acute toxoplasmosis per 1,000 pregnant women in Mato Grosso do Sul was 4.2 (Figueiro-Filho et al. 2007) and 5.7 in Brasilia (Nobrega & Karnikowski 2005). The occurrence of congenital toxoplasmosis (CTox) was found to be 0.07/1,000 births in Sweden (Evengard et al. 2001), 0.08/1,000 in Massachusetts, USA, and in London, England (Guerina et al. 1994, Gilbert et al. 1995), 0.12/1,000 in Switzerland (Signorell et al. 2006), 0.3/1,000 in Barcelona, Spain (Munoz Batet et al. 2004), 0.4/1,000 in Denmark (Lebech et al. 1999), 1.1/1,000 in Poland (Paul et al. 2001), and 1.9-3.2/1,000 in Paris, France (Remington et al. 2005). In Brazil, the occurrence of CTox varied according to study design and serological method. In the Southern region, the prevalence of congenital infection based on cord blood samples reached 0.8/1,000 births (95% CI: 0.02-4.45) (Mozzatto & Procianoy 2003). Other studies using blood samples adsorbed onto filter paper found prevalences from 0.3/1,000 (Neto et al. 2000) to 0.6/1,000 newborns (Lago et al. 2007). In Ribeirão Preto, São Paulo, another cross-sectional study also using blood samples adsorbed onto filter paper (Carvalheiro et al. 2005) found a prevalence of 0.3/1,000 births. Using cord blood samples, Segundo et al. (2004) found a high prevalence of 5.0/1,000 newborns (95% CI: 1.4-12.7) in Uberlândia, Minas Gerais. Mother-to-child transmission (MTCT) rates have been found to be around 20-50% (Jones et al. 2001). Several studies have suggested lower rates of foetal transmission when maternal infection took place early during gestation (Hohlfeld et al. 1989, Jenum et al. 1998, Dunn et al. 1999, Foulon et al. 1999, Remington et al. 2005). On the other hand, there are reports that point towards a more serious disease when the mother is infected during the first trimester (Hohlfeld et al. 1989, Dunn et al. 1999, Montoya & Liesenfeld 2004). Apparently, these two findings are contradictory and need further investigation. Considering the above points, we decided to conduct a study to estimate the prevalence of acute toxoplasmosis among pregnant women in a large public hospital in Southern Brazil. Additionally, we estimated the birth prevalence of CTox and its incidence during the first year of life. We also assessed MTCT rates based on the likeliness of infection as determined by the diagnostic categories set by theEuropean Research Network on Congenital Toxoplasmosis (ERNCT). PATIENTS, MATERIALS AND METHODS Patients - Maternity care at Hospital Nossa Senhora da Conceição (HNSC) , a 900-bed public general hospital in Porto Alegre, Rio Grande do Sul, Brazil, is characterised by assisting medium and high risk pregnancies covered by the Brazilian National Health System. The hospital is a reference centre for assisting pregnant women and babies with suspected or proven Toxoplasma gondii infections. A cross-sectional study was conducted from October 1998-December 2005 in which 41,112 pregnant women were screened for T. gondii antibodies. All of the newborns from the women presenting ERNCT diagnostic criteria (Lebech et al. 1996) of acute toxoplasmosis during pregnancy were included in a historical cohort. The infants were included in a follow-up study for a median time of 11 months to identify definite diagnosis by persistent IgG antibodies. The diagnostic criteria used in this study were based on an adaptation of the ERNCT classification system due to the inclusion of the IgG avidity test in our routine. Therefore, the probability of a primary T. gondii infection during pregnancy was grouped into four categories: definite, probable, possible and unlikely. In addition to the maternal criteria diagnosis, we considered a positive polymerase chain reaction (PCR) nested assay in the amniotic fluid as a definite diagnosis, while a low IgG avidity test was considered a probable diagnosis. The newborns were screened soon after birth using clinical examination, complete blood cell count with differential and platelet count, specific anti-T. gondii IgG and IgM antibodies, cerebrospinal fluid (CSF) cell count, head ultrasonographic evaluation, PCR-nested assays of blood or CSF samples and a detailed ophthalmologic examination. All positive specific-IgM antibody results were re-tested on the fifth or sixth day of life. Additionally, in the neonatal evaluation, we considered a blood sample or CSF with a positive PCR-nested assay as a probable diagnosis. These assays were not part of the original ERNCT criteria (Lebech et al. 1996). Unlikely cases were not included when CTox rates were calculated. Pregnant women with positive IgM and persistently low IgG concentrations (lower than 300 UI/mL) were excluded if the initial serology was performed during the first 20 weeks of pregnancy. This serological profile with a residual IgM index suggests an infection prior to the pregnancy. HIV-positive women and those with high IgG avidity detected in the first 16 weeks of pregnancy were also excluded (Remington et al. 2005). Materials - Three different immunological assays were used in the serological survey. During the first four years, the Microparticle Enzyme Immunoassay (MEIA, Abbott Diagnostics AxSYM® SYSTEM Toxo IgG and IgM version 2.0) was used alone. Since 2001, the hospital has introduced two additional tests to confirm MEIA's results: IgM capture technique and IgG avidity by Enzyme Linked Fluorescent Assay (VIDAS®). Statistical analysis - Proportions and their respective 95% confidence intervals were calculated based on the binomial distribution. The chi-square procedure was used to assess linear trends among proportions during the study period. Ethics - The present work has been approved by the ethics committee of HNSC. RESULTS From October 1998-December 2005, 41,112 pregnant women sought assistance at the HNSC's maternity health facility. The distribution of 241 of the initially included pregnant women is presented in Table I, according to ERNCT categories (definite, probable, possible and unlikely diagnosis). Among these women, 199 were identified using ERNCT criteria (definite, probable or possible) to have acute toxoplasmosis, which led to a cumulative prevalence of 4.8/1,000 pregnancies (95% CI: 4.2-5.6). Due to a twin gestation, there were 200 exposed babies included in the follow-up study. Figure shows acute toxoplasmosis prevalence rates in pregnant women during the study. After 2001, there was a considerable decrease in the prevalence rates from 6.6/1,000 (in 2001) to 2.1/1,000 pregnancies (in 2005) (χ2 for trend, p < 0.001). After 2001, the proportion of women with systematic serological screening performed during antenatal care was higher than in the previous period (86.7% vs. 64.1%, respectively). However, when IgM capture and IgG avidity tests were introduced in our routine, it was observed that the average gestational age for testing during pregnancy became progressively higher (27.3-32.1 weeks from 2002-2005). There were 40,727 live births out of the 41,112 pregnancies. Out of these, 25 were considered to have CTox at birth. When only considering the definite and probable categories, the estimated prevalence of CTox at birth was 0.6/1,000 newborns (95% CI: 0.4-0.9). Twelve additional cases were detected during the follow-up study, increasing the CTox rate to 0.9/1,000 newborns (95% CI: 0.6-1.3). Therefore, the incidence of CTox diagnosed during the first year of life was 0.3/1,000 newborns (95% CI: 0.2-0.5). From the 200 exposed babies, we found 37 CTox cases according to ERNCT criteria by the end of the first year of life. This led to a MTCT rate of 18.5% (95% CI: 13.5-24.7). The MTCT rates stratified by ERNCT categories for diagnosis of primary maternal infection are shown in Table II. Because of losses during the follow-up period, it was not possible to establish a definite CTox diagnosis for 47 out of the 200 followed infants (23.5%). Considering that both cohort groups had the same characteristics (origin, number of years of school and maternal age, prenatal care, amniocentesis, treatment during the pregnancy and birthweight), the losses probably did not influence the results. DISCUSSION The high prevalence of acute toxoplasmosis during pregnancy found in this study was expected, since a high frequency of seropositivity (prevalence: 59.8%; 95% CI: 57.0-62.5%) in this population was reported in a previous study (Varella et al. 2003). In the present report, we have stratified toxoplasmosis diagnosis according to adapted ERNCT criteria. Cases of acute acquired toxoplasmosis during gestation that were classified as definite or probable were responsible for our findings of an MTCT rate of 18.5%, while the remaining categories, possible and unlikely, did not cause congenital infection. The acute toxoplasmosis rate in pregnant women (2.8/1,000) (Table I) found in this study was higher than the rates found in Sweden (0.5/1,000) (Evengard et al. 2001), Norway (1.7/1,000) (Jenum et al. 1998), Denmark (2.1/1,000) (Lebech et al. 1999) and New York (2.0/1,000) (Lopez et al. 2000), but lower than the rates published by others (Naessens 2003, Remington et al. 2005). In Brazil, the Southern region, where this study was conducted, has a low prevalence of toxoplasmosis among pregnant women (Nobrega & Karnikowski 2005, Figueiro-Filho et al. 2007). However, there is substantial variability in the reported data, depending on chosen population, diagnostic methods used in screening, or even the different risk factors involved in disease transmission (Buffolano et al. 1996, Kapperud et al. 1996, Cook et al. 2000, Jones et al. 2001). The introduction of the IgG avidity test in the diagnostic panel of acute toxoplasmosis reduced false-positive rates and unnecessary diagnostic and therapeutic interventions (Liesenfeld et al. 2001, Montoya et al. 2002, Remington et al. 2004). We found that the IgG avidity test did not impact incidence rate findings in this study. This test can only rule out acute infection if performed within 16 weeks of gestation, contrary to what happened in our cohort (Remington et al. 2004). It seems that other factors may be involved in the reduction of toxoplasmosis prevalence. We considered that the reduction of prevalence during the study period could reflect a failure of the healthcare system in following guidelines and guaranteeing that the suspected case will have easy access to reference serv-ices. Additionally, the introduction of the IgM capture test may have contributed to the reduced prevalence due to its higher specificity, but this possibility was not evaluated in the present study. The prevalence of CTox by the end of the first year of life in our study (0.9/1,000/ newborns) was comparable to that found at birth in other areas of Southern Brazil (Glasner et al. 1992, Mozzatto & Procianoy 2003, Lago et al. 2007). A prevalence of 5.0/1,000 newborns reported in Minas Gerais, Brazil, could partially be explained by the use of cord blood samples (Segundo et al. 2004). According to some authors, using this type of sample could induce higher false positive rates (Naessens et al. 1999). Compared to other countries, our CTox rate at one year of age was similar to that found in Poland (1.1/1,000) (Paul et al. 2001) and was greater than those reported for Sweden (0.07/1,000) (Evengard et al. 2001), Massachusetts, USA (0.08/1000) (Guerina et al. 1994) and London, England (0.08/1,000) (Gilbert et al. 1995), Switzerland (0.12/1,000) (Signorell et al. 2006), Barcelona, Spain (0.3/1,000) (Munoz Batet et al. 2004) and Denmark (0.4/1,000) (Lebech et al. 1999). Only in Paris, France was a higher occurrence reported (1.9-3.2/1,000) (Remington et al. 2005). The high prevalence of CTox at 12 months of age found in our study (0.9/1,000 newborns) is cause for concern. This rate could have been underestimated, particularly if we take into account that some potential cases could have been lost in the follow-up study. On the other hand, some cases could have been added to our cohort due to referral bias. Therefore, we suggest future, large collaborative studies using a standardised methodology to gather more precise estimates of the burden of this disease in our region. We found an overall rate for MTCT of 18.5%. Due to the difficulties involved in establishing an adequate diagnosis during pregnancy, we presented MTCT rates by ERNCT categories. This approach encompasses all aspects of CTox and provides MTCT rates that could be compared between locations with different health systems. If we only consider the definite category, our MTCT rate could be as high as 81.4%, which would be higher than that reported by Foulon et al. (1999). On the other hand, we should not neglect the possibility of transmission in the probable ERNCT category. In Brazil, preventive strategies for CTox have not yet been proposed. There is some controversy regarding which screening method would achieve the best results. Should we perform antenatal screening with early treatment (Thiebaut et al. 2007) or neonatal screening and treat the consequences? Regarding these questions, our study has clarified one particular point: there is a considerable level of incidence, estimated to be around 0.3 cases/1,000 newborns, that goes undetected with the current neonatal screening strategy. The future challenge for CTox screening is to identify the most cost-effective strategy so that it may be adopted in the coming years. REFERENCES
Copyright 2009 - Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc09060t2.jpg] [oc09060t1.jpg] [oc09060t3.jpg] [oc09060f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}