 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memórias do Instituto Oswaldo Cruz, Vol. 104, No. supp 1, July, 2009, pp. 159-166 Morbidity and prognostic factors in chronic chagasic cardiopathy Manoel Otávio C Rocha+; Maria Carmo P Nunes; Antonio L Ribeiro Programa de Pós-Graduação
em Ciências da Saúde, Infectologia e Medicina Tropical, Departamento
de Clínica Médica, Faculdade de Medicina, Hospital das Clínicas,
Universidade Federal de Minas Gerais, Av. Alfredo Balena 190, 30130-100 Belo
Horizonte, MG, Brasil Received 26 March
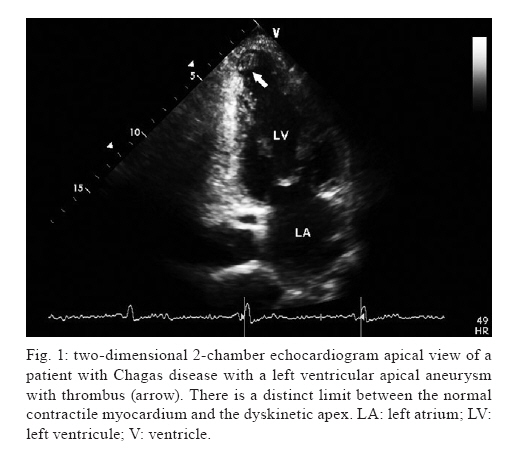
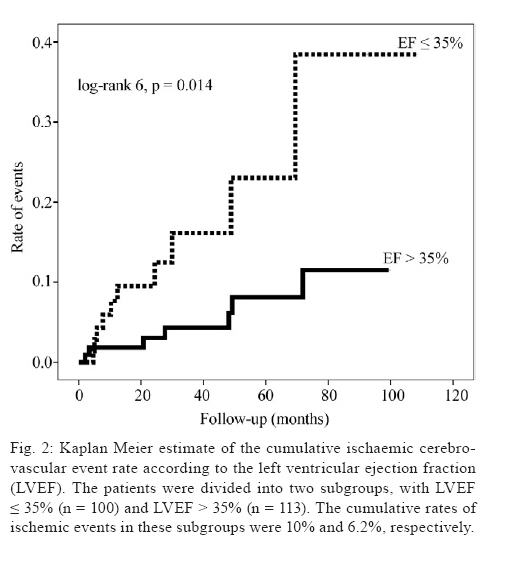
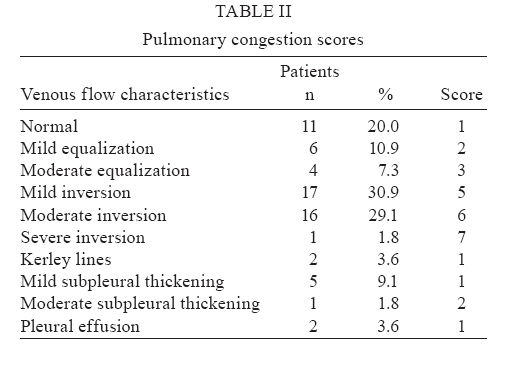
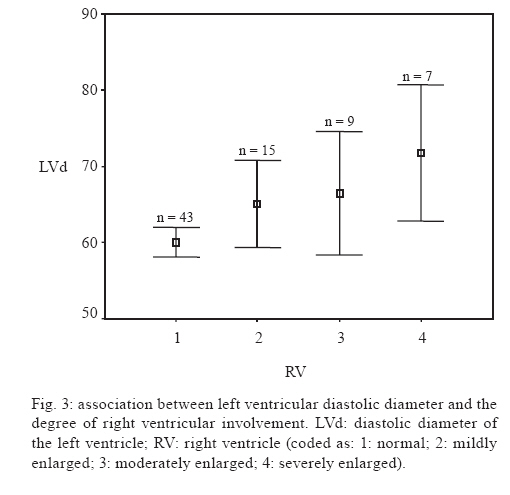
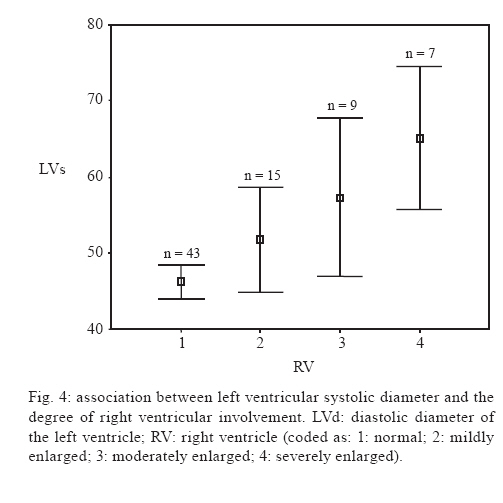
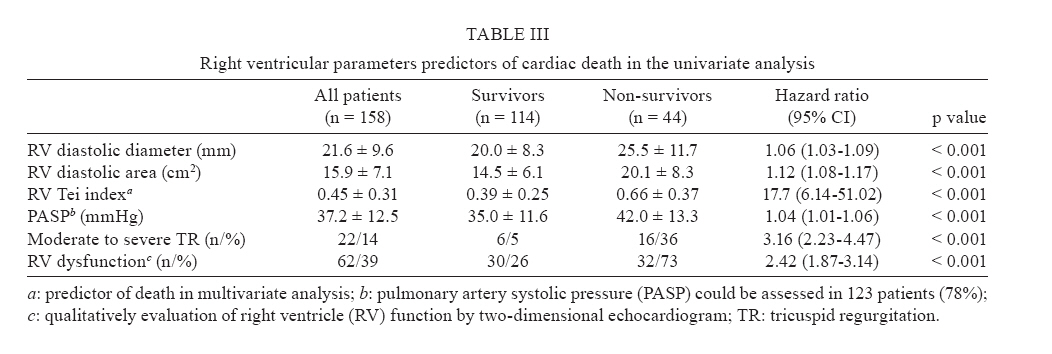
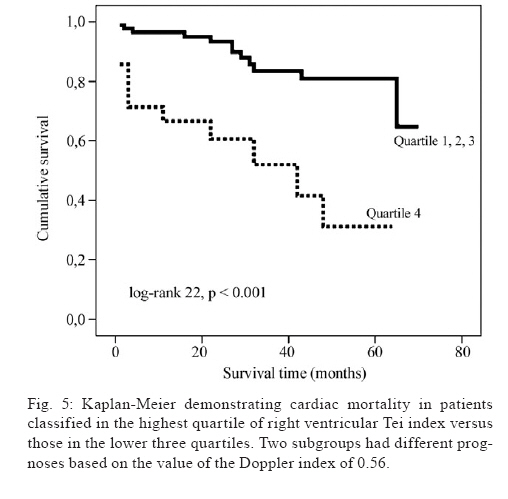
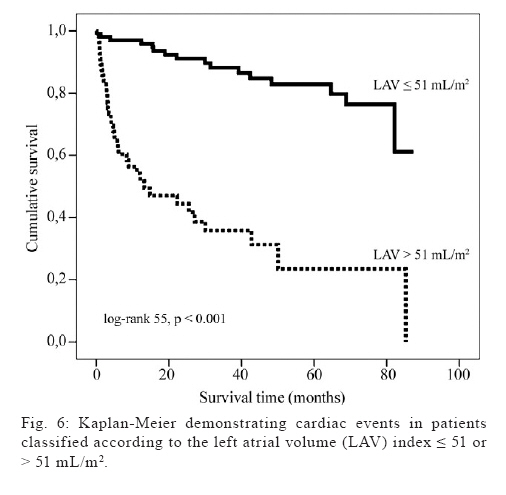
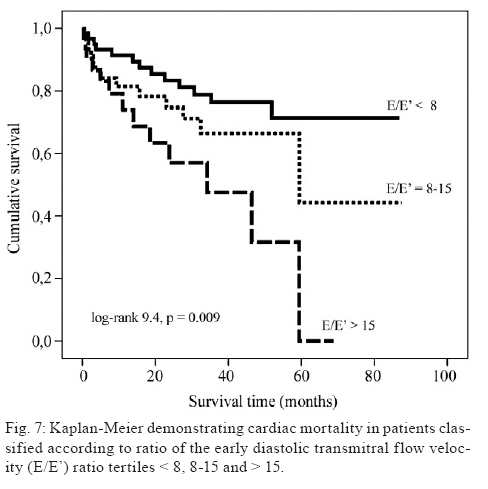
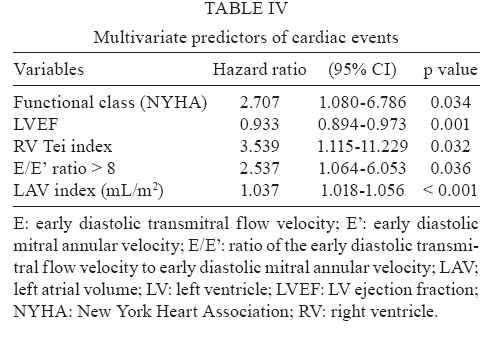
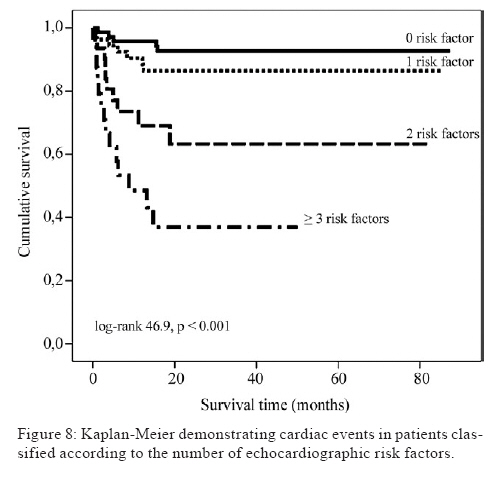
2009 Financial support: FAPEMIG, CNPq Code Number: oc09104 ABSTRACT Chagas disease is a pleomorphic clinical entity that has several unique features. The aim of this study is to summarise some of the recent contributions from our research group to knowledge of the morbidity and prognostic factors in Chagas heart disease. A retrospective study suggested that ischaemic stroke associated with left ventricular (LV) apical thrombi is the first clinical manifestation of Chagas disease observed in a large proportion of patients. LV function and left atrial volume (LAV) are independent risk factors for ischaemic cerebrovascular events during follow-up of Chagas heart disease patients. Pulmonary congestion in Chagas-related dilated cardiomyopathy is common but usually mild. Although early right ventricular (RV) involvement has been described, we have shown by Doppler echocardiography that RV dysfunction is evident almost exclusively when it is associated with left ventricle dilatation and functional impairment. In addition, RV dysfunction is a powerful predictor of survival in patients with heart failure secondary to Chagas disease. We have also demonstrated that LAV provides incremental prognostic information independent of clinical data and conventional echocardiographic parameters that predict survival. Key words: Chagas disease - prognosis - morbidity - heart failure - arrhythmias Chagas disease is endemic in South and Central America, where an estimated 10 million patients are infected and another 100-120 million people are at risk of contracting the disease (PAHO 2007). Every year in Latin America approximately 21,000 patients die of Chagas-related causes (WHO 2009). Moreover, Chagas disease frequently affects patients in their most productive working years and treatment is very costly, so this disease has important economic consequences for the region (Wilson et al. 2005). Chronic cardiomyopathy is the most important and severe manifestation of human Chagas disease, eventually affecting approximately 20-30% of those in the chronic phase of the disease. It causes heart failure, arrhythmias, heart-blocks, thromboembolism, stroke and sudden death (Rocha et al. 2003, 2007). The main cardiac pathological finding in Chagas disease patients is chronic, progressive and fibrosing myocarditis (Rossi 1998, Andrade 1999, 2000, Rossi et al. 2003, Coura 2007). Focal myocarditis occurs even in the indeterminate form of the disease and becomes more intense as the disease progresses to more severe clinical stages. In the chronic stages of the disease, tissue parasitism and blood parasitemia are scant. The loss of cardiomyocytes and their substitution by fibrotic tissue appear to induce disruption of muscle fibres and fascicles (Bogliolo 1976a, b). These architectural changes lead to malfunctioning of the electrophysiological sincitia, causing heart failure and ventricular arrhythmias that result in poor prognoses and high premature mortality rates. Damage to the autonomic nervous system, especially the parasympathetic branch, is also a specific and early feature in Chagas disease that may contribute to the high rate of sudden death among these patients (Ribeiro et al. 2001, 2002). The clinical approach to Chagas disease patients should consider the pleomorphism of clinical presentations and the existence of unique features in this disease, such as the high prevalence of apical ventricular aneurisms, the biventricular nature of the associated heart failure, the importance of thromboembolic manifestations, and the high prevalence of both conduction disturbances and ventricular arrhythmias (Rocha et al. 2007). Previous studies have demonstrated a poorer prognosis for patients with Chagas cardiomyopathy than for those with other causes of heart failure (Freitas et al. 2005 Campos Lopes et al. 2006, Silva et al. 2008). Very few clinical trials (Roberti et al. 1992, Khoury et al. 1996, Davila et al. 2002, Botoni et al. 2007b) have been carried out on patients with Chagas heart failure and some of those were short-term, non-randomised studies. Nonetheless, the treatment guidelines for heart failure due to other conditions (Hunt et al. 2005) are generally applied to treatment of the condition in the Chagas disease population. The direct transposition of recommendations derived from studies on heart failure from other aetiologies in patients generally from Europe and North America to Latin American Chagas disease patients is potentially misleading (Botoni et al. 2007b). Moreover, the physician's perception that Chagas disease is a distinct condition may lead to suboptimal dosing or a lack of initiation of medications with proven efficacy in patients with other heart failure aetiologies (Botoni et al. 2007a). Thus, validated recommendations for the management of Chagas-associated heart failure are clearly needed. In this article, we summarise some recent contributions from our research group to knowledge of the morbidity and prognosic factors of Chagas heart disease. Morbidity factors related to chronic Chagas cardiopathy Thromboembolic events - Embolic events are quite common in Chagas disease, representing the third leading cause of death and a significant cause of long-term disability among these patients.In the majority of cases, mortality from these complications is related to pulmonary and cerebral embolism (Braga et al. 1995). Cardiac thrombi commonly cause embolisms in Chagas cardiomyopathy (Braga et al. 1995, Bestetti 2000, Salomone et al. 2003). The inflammatory process, as well as dilation and dysfunction of the myocardium and endocardium, result in blood stasis and thrombosis. The reported prevalence of intracardiac thrombi in patients with Chagas disease varies widely. Most published data come from necropsy studies, which excludes patients in the early stages of the disease or those minimally affected. Necropsy studies have detected left ventricular (LV) thrombosis in 35-46% of patients who died from congestive heart failure or sudden death with chronic Chagas disease (Samuel et al. 1983). A previous study from our group (Nunes et al. 2005) that assessed the prevalence of cardiac thrombi in 75 patients with Chagas cardiomyopathy by transthoracic and transesophageal echocardiography detected LV thrombi in 17 patients (23%), whereas apical aneurysms were found in 35 patients (47%). Four patients (5%) had thrombi in the left atrial appendage and one (1%) in the right atrial appendage. Similar to other studies, intra-cavitary thrombi were detected mainly in the apex and in the presence of the apical aneurysm typical of Chagas disease (Fig. 1). In our study, ischaemic stroke was associated with LV apical thrombi and was the first clinical manifestation of Chagas disease in 57% of the patients with mild systolic dysfunction. Although these patients would otherwise be considered to have a better prognosis, they have disabilities as a consequence of the stroke. Thus, mild systolic dysfunction in patients with Chagas disease does not seem to warrant a good prognosis for embolic events. All efforts to detect thrombi and other risk factors for stroke must be made, even in this group of patients. Our study demonstrates that anticoagulation may be advisable in the management of patients with Chagas cardiomyopathy, even for those patients who do not present with severe systolic dysfunction. Ischaemic stroke is independently associated with Chagas disease (Carod-Artal et al. 2005, Oliveira-Filho et al. 2005, Carod-Artal 2007). In contrast to autopsy studies, which report a high frequency of cerebral in-farction (Samuel et al. 1983, Pittella 1993), clinical studies have revealed a low prevalence of stroke in patients with chronic Chagas heart disease (Bestetti 2000). Apical aneurysm, mural thrombus, congestive heart failure and cardiac arrhythmias are important risk factors in the genesis of ischaemic stroke related to Chagas cardiomyopathy (Carod-Artal et al. 2005, Nunes et al. 2005, Oliveira-Filho et al. 2005, Carod-Artal 2007). The available studies on heart failure suggest that patients with poor LV systolic function have an increased risk of thromboembolic events (Dries et al. 1997). The identification of factors that can predict a high risk of embolic complications is important, because these risk factors could influence decisions regarding the use of anticoagulants. Therefore, we performed a study to assess the long-term cumulative risk of ischaemic cerebrovascular event (ICE) in a large cohort of patients with Chagas cardiomyopathy (Nunes et al. 2009a). The study enrolled 213 consecutive patients with Chagas disease and LV systolic dysfunction who were recruited prospectively from our institution from June 1999-Jan 2007. The use of anticoagulation was based on clinical indications. ECG and a comprehensive Doppler echocardiogram with colour flow mapping were obtained in all patients. The endpoint was an ICE, which was defined as a fatal or nonfatal stroke or transient ischaemic attack (TIA). The mean patient age was 48.7 ± 11.9 years and 82 (38%) were female. Apical aneurysms were detected in 95 patients (45%) and these aneurysms were associated with a thrombus. Thrombi were detected by two-dimensional echocardiography in 30 patients (14%) during the first echocardiographic evaluation. At the time of enrolment, 39 patients (18%) had had a previous ICE. Multiple logistic regression revealed that apical aneurysm (odds ratio, 2.95; 95% CI, 1.32-6.59; p = 0.009) and LV thrombus (odds ratio, 3.69; 95% CI, 1.53-8.89; p = 0.004) were independent risk factors for previous cerebrovascular events. During a mean follow-up of 35.8 months (median 27.6; range 7 days-9 years), 69 patients died and seven patients underwent cardiac transplantation. ICE occurred in 17 patients (8%): nine had a stroke (3 fatal cases) and eight had a TIA, with an overall incidence of 2.67 events per 100 patient-years. Independent risk factors for ICE included LV ejection fraction (LVEF) (hazard ratio 0.95, 95% CI, 0.91-0.99; p = 0.009) and left atrial volume (LAV) corrected for body surface area (hazard ratio 1.04, 95% CI, 1.01-1.07; p = 0.007), which persisted after adjustment for anticoagulation use. Data from patients with atrial fibrillation were excluded from the analysis, because it is an independent risk factor for stroke. The presence of an apical aneurysm or thrombus was not an independent long-term risk factor for future ICE. However, patients with LV thrombus were also more likely to be anticoagulated (40%, vs. 22% in those without thrombus; p = 0.041). Of the 39 patients who had had a previous stroke or TIA, four patients (10%) presented with a new ischaemic event and 13 patients (33%) had a transplant or died during the follow-up period. Although a history of ischaemic events is also a risk factor for a subsequent stroke, in our study, we were not able to demonstrate a relation between the presence of these risk factors and future embolic cerebrovascular events. However, the patients we identified as high risk for ischaemic events were anticoagulated, which may have prevented further embolic events. To determine the threshold LVEF below which the rate of ICE increased, patients were divided into two groups based on the ejection fraction (< 35%, n = 100, and > 35%, n = 113). The total cumulative ICE rate in each subgroup was as follows: 10% for patients with an LVEF of < 35% and 6.2% for those with an LVEF above 35% (p = 0.016) (Fig. 2). Therefore, the annual incidence of ICE in patients with Chagas cardiomyopathy was low. LVEF and LAV appear to be independently associated with ischaemic events. In conclusion, embolic events in patients with Chagas cardiomyopathy are associated with apical aneurysms and mural thrombi. Intracavitary thrombi are detected mainly in the apex and in the presence of the typical Chagas disease aneurysm. In our study, the annual incidence of ICE in patients with sinus rhythm was low; however, patients at high risk for ischaemic events were anticoagulated. Clinical trials have not addressed the effectiveness or the risks of long-term anticoagulation in patients with Chagas cardiomyopathy. Considering the high cost of anticoagulation for patients with low socioeconomic status, the routine use of anticoagulants in these patients may not be justified. Currently, anticoagulation is recommended for patients with LV apical aneurysms with a mural thrombus, atrial fibrillation or previous stroke. Pulmonary congestion in Chagas cardiomyopathy In patients with Chagas cardiomyopathy, it is common to find a discrepancy between the intensity of pulmonary congestion and the grade of cardiomegaly, in spite of significant LV systolic dysfunction (Ferreira 1985). The mechanism underlying the pulmonary congestion has not been established. A previous study from our group (Barral 2006) investigated the correlation between the degree of pulmonary congestion as detected by standard chest X-ray and various echocardiographic and Doppler indexes of left ventricle function in 55 patients with Chagas dilated cardiomyopathy. The degree of change in pulmonary venous vessels on chest X-ray was graded using a pulmonary congestion score and then compared to echocardiographic parameters. All radiological parameters were graded and the degree of changes of pulmonary venous vessels on chest X-ray was established (Table I) using a previously described pulmonary congestion score (Milne et al. 1985). Chest X-rays were reviewed by a second independent observer, and four cases (7%) of inter-observer discordance were solved by consensus. Chest X-ray was normal in 11 patients (20%) and showed some degree of pulmonary venous abnormality in 44 patients (80%). The radiological findings of pulmonary congestion are shown in Table II. The mean lung congestion score was 4.22 ± 2.29. In a multivariate analysis, LVEF, right ventricular (RV) function and the colour M-mode velocity correlated with the degree of pulmonary congestion. In conclusion, pulmonary venous changes on chest X-rays are common but usually mild in patients with Chagas dilated cardiomyopathy. In a comparative study of pulmonary venous hypertension between 65 consecutive patients with Chagas cardiomyopathy and 65 with non-chagasic cardiomyopathy, we showed that the degree of pulmonary congestion was lower in the chagasic patients (Barral 2006). In this study, we found that diastolic dysfunction with increased LV flling pressure is associated with the degree of pulmonary congestion by chest X-ray in both groups. The LV filling pressure is higher in non-chagasic cardiomyopathy than in chagasic cardiomyopathy. RV function in patients with Chagas cardiomyopathy Heart failure in Chagas disease presents certain physiopathology and management peculiarities (Acquatella et al. 1987, Rocha et al. 2003) with considerable variability in the clinical course of individual patients. Early RV involvement has been demonstrated in studies that analysed biventricular function (Marin-Neto et al. 1998, Barros et al. 2002) and severe RV dysfunction was identified as the only functional cardiac abnormality in asymptomatic patients with chronic Chagas disease who do not exhibit overt clinical signs of heart failure (Marin-Neto et al. 1988). Although early RV involvement has been described, we previously showed that RV dysfunction by Doppler echocardiography was evident when it was associated with dilatation and LV functional impairment (Nunes et al. 2004). In this study, greater dilation of the right ventricle was associated with larger LV diastolic (Fig. 3) and systolic (Fig. 4) diameters in 74 patients with Chagas cardiomyopathy. As LV function deteriorated, the RV began to fail too. Though the inflammatory process caused by the infection likely contributes to this failure, RV failure is observed because the elevated LV end-diastolic pressure increases RV afterload. This explains why RV dysfunction, as detected by Doppler echocardiography, occurred only in the presence of associated LV dysfunction in our study. Mild RV involvement detected by biopsy (Mady et al. 1999) may be clinically insignificant and not detectable by Doppler echocardiography. Regardless of the aetiology of the cardiomyopathy, RV function is determined by intrinsic RV contractile ability and by ventricular preload and afterload. The causes of right heart failure vary widely and can be subdivided into different pathophysiological states, which can coexist in the same patient. Hence, in another study with a larger sample of 158 patients (Nunes et al. 2007), we demonstrated that RV function is likely related to other mechanisms besides elevated pulmonary artery pressure in Chagas disease. Several standard Doppler echocardiographic measurements used to assess the RV function were associated with mortality in a univariate analysis (Table III). However, the quantitative evaluation of global RV function by Doppler-derived Tei index had the strongest correlation with cardiac mortality (hazard ratio 17.7, 95% CI, 6.14-51.02) as compared to other measurements such as end-diastolic diameter and area, as shown in Table III. In a multivariate Cox regression, backward stepwise analysis adjusted by other variables, prolonged RV Tei index persisted as a significant predictor of death (hazard ratio 5.75, 95% CI, 1.69-19.51), adding incremental prognostic value to the New York Heart Association (NYHA) functional class and LVEF. Cardiac mortality was compared by Kaplan Meier analysis according to the quartiles of RV Tei index. When RV index was > 0.56 (highest quartile), the hazard ratio of cardiac death was significantly increased as compared with the lower quartiles (hazard ratio 5.29, 95% CI, 2.43-11.52) (Fig. 5). The pathogenesis of myocardial lesions in the chronic form of Chagas heart disease is complex. Several questions remain to be answered to fully understand its mechanism. The differences in cardiac morphology in our patients may have been a consequence of more extensive biventricular involvement in the primary pathologic process (myocardial fibrosis and myofibrillar loss) in the patients with RV dysfunction, which may be independent of pulmonary hypertension. Therefore, irrespective of the mechanism, RV dysfunction is a powerful predictor of survival in patients with heart failure secondary to Chagas dilated cardiomyopathy. Prognostic value of LAV in patients with Chagas cardiomyopathy A variety of echocardiographic techniques can identify abnormal diastolic function, LV filling pressures and cardiovascular mortality. In patients with chronic Chagas cardiomyopathy, diastolic dysfunction is a hallmark of severe disease (Carrasco Guerra et al. 1987). The accumulation of interstitial collagen fibres in Chagas disease chronic myocarditis may decrease myocardial compliance, which will lead to increased left atrial pressure (Carrasco Guerra et al. 1987, Rochitte et al. 2005). Nevertheless, studies assessing the long-term prognostic value of echocardiographic parameters in Chagas disease patients are scarce. LAV, a marker of chronically elevated LV filling pressure, is a predictor of prognosis in patients with heart failure and may be important in the risk assessment of patients with Chagas disease. Therefore, we evaluated the prognostic value of LAV in a large series of patients with impaired LV systolic function due to Chagas heart disease (Nunes et al. 2009b). We also compared the prognostic impact of LAV to other established echocardiographic outcome predictor parameters. A total of 192 patients with Chagas cardiomyopathy (mean age 48 ± 12 years, 37% women) were prospectively enrolled. Endpoints were death or cardiac transplantation. With a mean follow-up of 33.8 months, LAV normalised for body surface area emerged as an independent predictor of survival (hazard ratio 1.037 per 1-mL/m2 change, 95% CI, 1.018-1.056, p < 0.001), adding incremental prognostic value to clinical factors, LVEF, and Doppler-derived parameters of diastolic function. The analysis of the receiver-operator characteristic (ROC) curve identified the best cut-off values for the prediction of endpoints. A LAV > 51 mL/m2 was associated with significantly higher mortality (log-rank, p < 0.001) (Fig. 6). Likewise, E/E' ratio, a new parameter that has been proposed and validated as an estimate of LV filling pressures (Ommen et al. 2000), was an independent predictor of adverse outcome. Similar analyses were also performed after stratifying patients based on E/E' ratio tertiles (Fig. 7). An E/E' ratio > 8 suggested abnormal filling pressure and correlated independently with adverse outcomes in multivariate analysis (hazard ratio 2.537, 95% CI, 1.064-6.053, p = 0.036). Multivariate associations with events are shown in Table IV. Five variables maintained their prognostic significance after multivariate analysis: NYHA functional class, LVEF, RV Tei index, E/E' ratio and LAV index. We plotted ROC curves to identify the cut-off values for unadjusted 1-year cardiac event rate. Likewise, to better define the individual risk of Chagasic patients with reduced LVEF, we developed a non-invasive predictive model based on the independent echocardiographic risk factors identified by multivariate analysis. The prediction model made it possible to identify four patient risk groups according to the number of echocardiographic risk factors. The Cox proportional hazard model showed that patients with three or more risk factors had a hazard ratio of 11.408 (95% CI, 5.009-25.324, p < 0.001), when compared to patients with no risk factors. At 1-year follow-up, the event-free survival rate was 96% for patients with no risk factors versus 43% for those with three or more risk factors; the intermediate group results were between these figures, as expected (Fig. 8). In conclusion, we demonstrated that LAV provides powerful incremental prognostic information independent of clinical data and conventional echocardiographic survival predictors of mortality. NYHA functional class, LVEF, RV function, E/E' ratio and LAV index may be used to build a risk prediction model for clinical use. Chagas disease is still a major health problem in Latin American despite reasonable control of the infection. The clinical course of the disease is quite variable. More severely affected patients may experience serious cardiac disease with heart failure, arrhythmias, heart blocks and thromboembolic events. Given the high number of Chagas disease patients in Latin America, it is very useful to identify patient groups with a high risk of disease progression and death. These high-risk patients might benefit the most from aggressive therapies, including defibrillator implantation, cardiac resynchronisation and cardiac transplantation, and these aggressive interventions could potentially improve patient survival. This article reviewed our recent contributions to understanding the morbidity and mortality of Chagas disease, focusing on some controversial issues such as thromboembolic manifestations, pulmonary congestion, RV function and LAV. Further clinical research is warranted to optimise the care of Chagas disease patients, as well as to improve the assessment of patients' risk for disease progression and death. ACKNOWLEDGEMENTS To Felipe Barbosa, for the help in writing this manuscript. REFERENCES
Copyright 2009 - Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc09104t4.jpg] [oc09104f7.jpg] [oc09104f1.jpg] [oc09104t3.jpg] [oc09104f3.jpg] [oc09104f5.jpg] [oc09104t2.jpg] [oc09104t1.jpg] [oc09104f4.jpg] [oc09104f6.jpg] [oc09104f2.jpg] [oc09104f8.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}