 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memórias do Instituto Oswaldo Cruz, Vol. 104, No. 4, July, 2009, pp. 665-667 SHORT COMMUNICATIONS Low frequency of human papillomavirus detection in prostate tissue from individuals from Northern Brazil Rodrigo Vellasco Duarte SilvestreI; Mariana Ferreira LealII; Samia DemachkiI; Márcia Cristina de Souza NahumI; Julio Guilherme Balieiro BernardesIII; Silvia Helena Barem RabenhorstIV; Marília de Arruda Cardoso SmithII; Wyller Alencar de MelloV; Adriana Costa GuimarãesVI; Rommel Rodríguez BurbanoVI, + IDepartamento
de Anatomia Patológica Financial support: MCT/CNPq/MS-SCTIE-DECIT (409678/2006-6), CNPq (RRB, MACS are fellowship), FAPESP (MFL is fellowship). Received 26 October
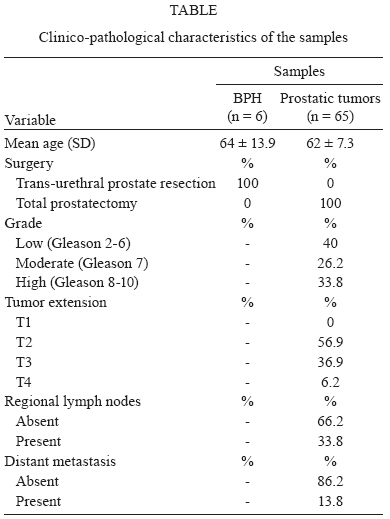
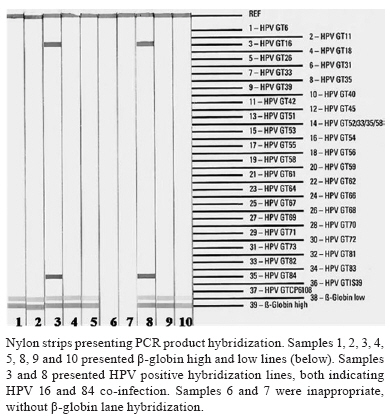
2008 Code Number: oc09149 ABSTRACT The presence of human papillomavirus (HPV) was evaluated in 65 samples of prostate tumours and six samples of prostates with benign prostatic hyperplasia from individuals from Northern Brazil. We used a highly sensitive test, the Linear Array HPV Genotyping Test, to detect 37 high and low-risk HPV types. In this study, only 3% of tumour samples showed HPV infection. Our findings support the conclusion that, despite the high incidence of HPV infection in the geographic regions studied, HPV was not associated with a higher risk of prostate cancer. To our knowledge, this is the first study evaluating the frequency of HPV detection in prostatic tissue of individuals from Brazil. Key words: human papillomavirus - prostate cancer - benign prostate hyperplasia Prostate cancer is the fifth most common cancer in the world and the second most common cancer in men (Parkin et al. 2005). In Brazil, an estimated 49,530 cases were newly diagnosed in 2008. However, in Northern Brazil, the incidence rates are lower than the national average rate (INCA 2007). In general, inflammation is associated with multiple cancers and prostate inflammation, in particular, has been suggested to be a factor in the development and progression of prostate cancer. Infections, particularly sexually transmitted and other ascending urogenital infections, are possible causes of intraprostatic inflammation and/or prostate cancer. Infectious organisms have been described to be important for the maintenance of local inflammation processes and can be responsible for the cellular alterations that lead to genetic and epigenetic alterations bringing cells to transformation (De Marzo et al. 2007). Several studies have suggested that the ethnic differences observed in the incidence rates of prostate cancer could be derived from cultural variations in sexual behaviour. The possible relationship between high risk human papillomavirus (HPV) infection and prostate cancer has been investigated previously (Anwar et al. 1992, Tu et al. 1994, Strickler & Goedert 2001, Adami et al. 2003, Carozzi et al. 2004, May et al. 2008). HPV codes for the oncoproteins E6 and E7 that are able to immortalise many cellular types, including prostate tissue cells, in vitro through the inactivation of the tumour suppressor genes, P53 and PRb (Choo et al. 1999). Epidemiological data also demonstrate that men with a history of anal cancer, a tumour associated with HPV infection, have an increased risk of developing prostate cancer (Rabkin et al. 1992). A clear association between HPV infection and the development of prostate cancer and/or progression has still not been established. To our knowledge, this is the first study evaluating the frequency of HPV infection in individuals with prostate cancer in Brazil. This study aims to detect high and low-risk HPV DNA, using a highly sensitive assay, in samples of prostate tumours and of prostates with benign prostatic hyperplasia (BPH), from individuals from Northern Brazil. The study included 65 cases of prostate cancer and six cases of BPH from patients who underwent surgical treatment. For each patient with BPH, samples were obtained from the urothelial region in the urethra and from the deep prostate tissue (without urothelial cells). Specimens were obtained from patients of several hospitals of state of Pará, Northern Brazil. All patients had negative histories of exposure to either chemotherapy or radiotherapy prior to surgery and the patients had no other diagnosed cancers. Informed consent with approval of the ethics committee of João de Barros Barreto University Hospital was obtained from all patients. Tumours were staged using standard criteria by Gleason score and TNM staging. No sample had a Gleason score lower than 5. Table shows the cases along with their clinico-pathological characteristics To extract DNA, tumour fragments and BPH samples were incubated in 200 μL TE solution (1 mM EDTA, Tris 10 mM, pH 7.4) with 20 mg/mL of proteinase K at 65°C overnight or until complete fragment digestion. Subsequently, the proteinase K was inactivated at 95°C for 15 min and the total product was used for phenol-chloroform DNA extraction. The Linear Array HPV Genotyping Test (Roche Molecular Diagnostic, Alameda, CA) was used for HPV detection in 100 ng DNA samples. The Linear Array test uses the PGMY09/11 L1 consensus primer system to amplify a HPV fragment of 450 bp and includes coamplification of a human cellular target, β-globin, as a control to DNA viability. Positive and negative HPV samples provided with the Linear Array HPV Genotyping Test were used as controls. Detection and HPV genotyping were achieved using a reverse line-blot method, and this test included probes to the genotypes of 37 high and low-risk HPV types [6, 11, 16, 18, 26, 31, 33, 35, 39, 40, 42, 45, 51, 52, 54, 55, 56, 58, 59, 61, 62, 64, 66, 67, 68, 69, 70, 71, 72, 73(MM9), 81, 82(MM4), 83(MM7), 84(MM8), IS39 and CP6108]. The PCR reaction was carried out using the following conditions; 2 min at 50°C followed by 9 min at 95°C; then, 40 cycles at 95°C for 30 s, 55°C for 1 min and 72°C for 1 min. Finally, reactions were subjected to a final extension for 5 min at 72°C. PCR products were separated by electrophoresis through a 1% agarose gel and the denatured PCR products were hybridised onto the strip containing specific probes for 37 HPV genotypes and β-globin reference lines. Adequate samples were those that showed β-globin amplification fragments in the agarose gel and in the strip after PCR product hybridization. HPV-positive samples were those that showed any hybridization line corresponding to a high and/or low-risk HPV type. The strips were interpreted using the HPV reference guide provided. Results from specimens that failed to amplify the β-globin internal control, indicating poor DNA recovery and an invalid sample, were excluded from the study. No BPH samples from the urothelial region or from deep prostate tissue showed HPV infection. Only two of 65 (3%) tumour samples showed HPV fragments and both of these were HPV 16 (Figure). All HPV 16-infected patients were co-infected with HPV 84. The two HPV-positive samples were classified as pT3aN1M0 and had a concerning, high grade Gleason score (final score of 8 and 9). The two patients with HPV infection were 62 and 65 years old. Many different pathogenic organisms can cause an inflammatory response in the prostate. Viral infections such as HPV, human herpes simplex virus type 2, cytomegalovirus and human herpes virus type 8 have been detected in prostate tissue. McNicol and Dodd (1990a, b) observed a high frequency of HPV infection in BPH and prostatic carcinoma samples. Other studies also found a possible association between HPV and prostate carcinogenesis (Anwar et al. 1992, Kuczyk et al. 2000, May et al. 2008). However, a clear association between HPV infection and prostate cancer has not been established. To evaluate the frequency of HPV infection in prostatic samples, we used the Linear Array HPV Genotyping Test, a sensitive assay for the detection of a large spectrum of HPV types. The Linear Array HPV Genotyping Test also has β-globin reference lines to guarantee the quality of DNA extraction and exclude some false negatives. In the present study, only 3% of prostate carcinoma samples showed HPV (16 and 84) infection and no BPH samples showed infection. Although HPV 16 has been associated with the carcinogenesis process, our findings corroborated those from other studies that did not find any association between HPV infection and prostate cancer due to the low frequency of this virus in prostatic samples (Ibrahim et al. 1992, Wideroff et al. 1996, Noda et al. 1998, Strickler et al. 1998, Saad et al. 1999, Adami et al. 2003). Thus, these studies do not support an aetiological role of HPV in prostate cancer. Moreover, HPV 84 is classified as a type with low oncogenic risk and tends to occur as a multiple-type infection involving HPV 16 (Franco et al. 1999). The low frequency of HPV that we found in prostate samples is probably not related to a low risk of sexually transmitted diseases in our population. In 2007, we observed a high incidence of HPV infection in Amazon communities in Northern Brazil. HPV was detected in 31.64% of 158 histologically-normal penile and vaginal smears, using the Linear array HPV Genotyping Test (unpublished observations). To our knowledge, this is the first study evaluating the presence of HPV in prostate tissue of individuals from Brazilian populations. Our findings do not support the involvement of HPV in the aetiology or progression of prostate carcinogenesis. REFERENCES
Copyright 2009 - Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc09149f1.jpg] [oc09149t1.jpg] |
| |||||||||

{kind=link}
{kind=link}