 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memórias do Instituto Oswaldo Cruz, Vol. 104, No. 5, August, 2009, pp. 755-763 ARTICLES Frequency and types of human papillomavirus among pregnant and non-pregnant women with human immunodeficiency virus infection in Recife determined by genotyping Vírginia da Conceição Ribes Amorim Bezerra BrandãoI, II, III, +; Heloisa Ramos LacerdaII, IV; Norma Lucena-SilvaV, VI; Ricardo Arraes de Alencar XimenesII, IV ICentro
Integrado de Saúde Amaury de Medeiros, Recife, PE, Brasil Financial support: MS, PAHO Received 4 February
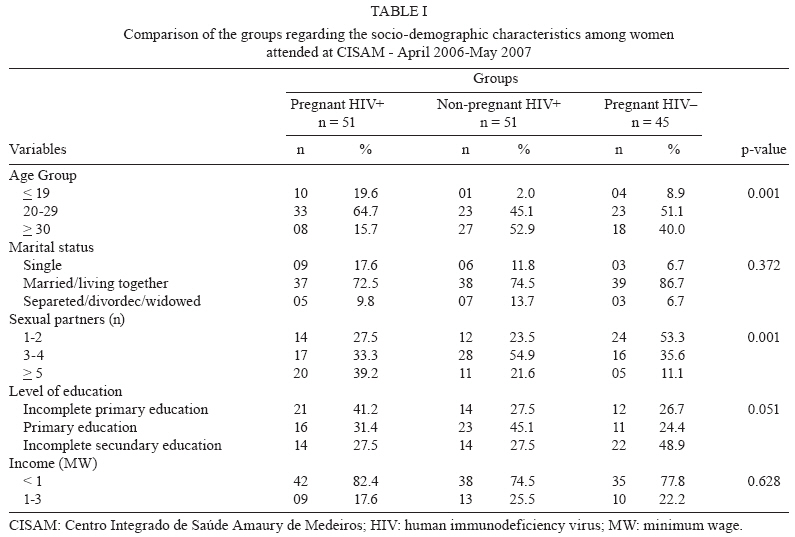
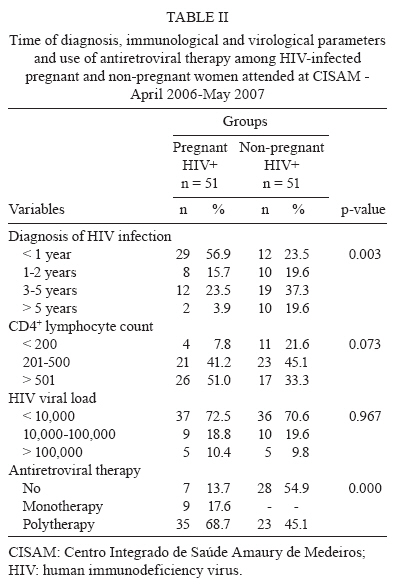
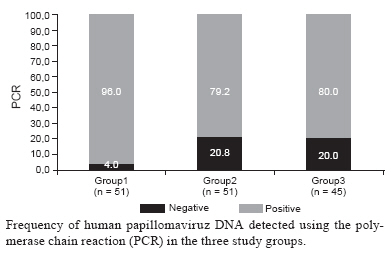
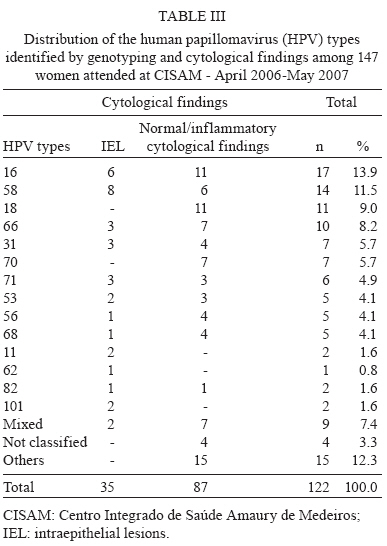
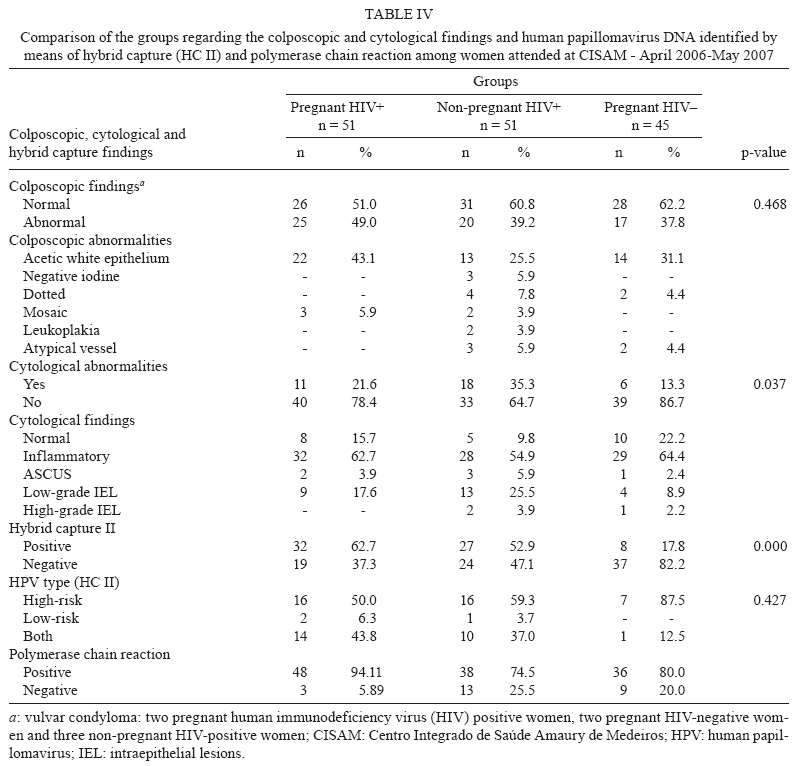
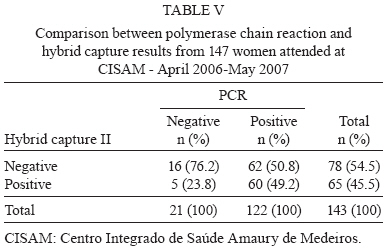
2009 Code Number: oc09167 ABSTRACT Women with human immunodeficiency virus (HIV) infection present a higher risk of infection by the human papillomavirus (HPV) and cervical cancer. To determine HPV genotypes and frequencies among HIV-positive women, an analytical cross-sectional study was carried out on 147 women (51 were pregnant and HIV-positive, 45 pregnant and HIV-negative and 51 HIV-positive and not pregnant), who were attended at a maternity hospital in Recife between April 2006-May 2007. They answered a questionnaire and underwent a gynaecological examination, with samples collected for HPV investigation by PCR, hybrid capture II, oncotic colpocytology (Papanicolau) and colposcopy. The frequency of HPV DNA was 85.3% (122/143), with a high proportion of HPV types that have been identified as high risk for cervical cancer. Among HIV-positive pregnant women, there was an HPV prevalence of 96% (48/50), of whom 60.4% (29/48) were high-risk. HPV 16, 58, 18, 66 and 31 were the most frequent types. Colpocytological abnormalities were observed in 35.3% (18/51) of HIV-positive non-pregnant women, 21.6% (11/51) of HIV-positive pregnant women and 13.3% (6/45) of HIV-negative pregnant women with a predominance of low-level lesions. A high prevalence of HPV infection was identified, especially with the high-risk types 16, 58, 18 and 66. This study identified high-risk HPV types in all three groups examined (HIV-positive pregnant women, HIV-negative pregnant women and HIV-positive not pregnant), characterising its distribution in this setting. Key words: human papillomavirus - human immunodeficiency virus - squamous intraepithelial lesion - pregnancy - polymerase chain reaction Genital infection due to oncogenic types of human papillomavirus (HPV) is the main etiological factor for uterine cervical cancer, although it is not sufficient by itself to cause the disease. In fact, the coexistence of various factors that allow the transition from infection to cancer is necessary (Nicol et al. 2005, Muñoz et al. 2006, Villa & Denny 2006, Zimmermann et al. 2006). The viral factors include the genotype, viral load, persistency and viral DNA integration with the host cell genome (Lillo et al. 2005). The host factors include an early start to sexual relations, multiparity (Muñoz et al. 2003), multiple sexual partners (Muñoz et al. 2006) oral contraceptive use (Moreno et al. 2002, Castrllsague & Muñoz 2003), smoking (Castrllsague & Muñoz 2003, Harris et al. 2004) and a history of sexually transmissible diseases such as herpes simplex (Hessol et al. 2004), Chlamydia trachomatis (Di Felice et al. 2005, Trotier & Franco 2006, Wright et al. 2006, Madaleine et al. 2007) and acquired immunodeficiency syndrome (Berrébi et al. 2008, Denny et al. 2008). Various studies have shown that cervical intraepithelial lesions (IEL) are more frequent and recurrent among seropositive women, with faster progression and worse response to standard treatment (Ellerbrock et al. 2000, Duerr et al. 2001, Jamieson et al. 2002, Ferenczy et al. 2003, Coelho et al. 2004, Levi et al. 2004, Campos et al. 2005, Palefsky 2006, Denny et al. 2008). This greater aggressiveness has a direct relationship with high-risk HPV genotypes, which are more frequent in the cervix of women infected with human immunodeficiency virus (HIV) (Berrébi et al. 2008). The high prevalence of HPV among HIV-positive women can be explained by the tendency for HPV to persist, thus differing from what occurs among immunocompetent individuals (Nappi et al. 2005, Hawes et al. 2006, Palefsky 2006, Berrébi et al. 2008, Denny et al. 2008). A reduction in immunity occurs during the gestational period. Specifically in the genital organs, the vaginal flora presents an imbalance that, associated with the greater dampness particular to that area, favours the development of infectious agents, among them HPV. Moreover, the hormonal factors and immunosuppression, which are necessary for maintaining a foetus, predispose a woman to the acquisition and development of lesions induced by HPV (Rando et al. 1989, Armbruster-Moraes et al. 2000, Costa et al. 2000, Correia et al. 2006). Anatomical modifications of the genital tract such as hypertrophy, congestion and ectopy also increase, followed by metaplasia. The area of immature squamous metaplasia is more susceptible to the development of preneoplastic lesions and HPV infections (Mota 2002, Correia et al. 2006). The incidence of HPV increases over the course of pregnancy (Schneider et al. 1987, Rando et al. 1989, Meisels 1992), with variations according to the population studied, gestational phase and diagnostic technique. During the first trimester of pregnancy, there is a low immune response to HPV, which explains the higher frequency of persistence of the virus during pregnancy. However, this deficient response undergoes an intense recovery at the start of the third trimester, with reinforcement during the postpartum period and consequent regression of the infection (Puig-Tintoré et al. 2002). The main objective of the present study was to evaluate the frequency and main types of HPV detected among HIV-positive pregnant women in Recife and to compare these findings with those among seronegative pregnant women and HIV-positive women who were not pregnant. PATIENTS, MATERIALS AND METHODS This was an analytical, cross-sectional study on 51 HIV-positive pregnant women who were attended at the Centro Integrado de Saúde Amaury de Medeiros (CISAM), Recife, Pernambuco, between April 2006-May 2007. Two comparison groups were formed. The first consisted of 51 HIV-positive women who were not pregnant, seen at Hospital Correia Picanço, State Health Department of Pernambuco, Recife or at CISAM and the second consisted of 45 HIV-negative pregnant women who came to CISAM for antenatal consultations. CISAM is a state reference unit for HIV-positive pregnant women, but it is also attended by HIV-negative women. Correia Picanço Hospital is the state reference unit for HIV-positive patients. Patients were consecutively selected in both units during the study period. The diagnosis of HIV infection was confirmed by means of two ELISA tests and one confirmatory test (indirect immunofluorescence) (MS 2005). Pregnancy was confirmed by means of a positive β-HCG examination or a confirmatory pregnancy ultrasound. The group of HIV-positive women who were not pregnant included women with HIV that had been confirmed using the above tests, but who were negative for β-HCG at the time of the examination. The HIV-negative pregnant women were selected from among those who sought the antenatal outpatient clinic of CISAM at any time during the pregnancy and were negative for anti-HIV (ELISA). In all seropositive patients, the most recent quantification of HIV viral load and TCD4-lymphocyte count was registered, provided that it had been carried out not more than six months before the time of the interview/examination. The viral load was quantified by means of the Cobas Amplicor HIV-1 monitoring test (Roche®), which uses the PCR technique and CD4+ lymphocytes were quantified using flow cytometry. Patients were excluded if they presented with genital bleeding, intense vulvovaginitis at the time of the examination or any mental deficit. The patients who agreed to participate in the study signed a free and informed consent statement and answered a questionnaire. A gynaecological examination was carried out, following a pre-established sequence: (i) the inspection insertion of a vaginal speculum, (ii) collection of material for HPV identification using PCR (MY09/MY11) and hybrid capture II (HC II) and (iii) collection of material for oncotic colpocytological examination. After insertion of the vaginal speculum, a brush (cytobrush®) was used to collect material from the endocervix. The material was distributed in a TE buffer solution (Tris-HCl + ethylenediaminetetracetic acid in pH 8) by shaking the brush in a previously identified Eppendorf tube. The samples were then transported to the Molecular Biology Laboratory of the Professor Fernando Figueira Integral Medicine Institute. DNA extraction, PCR and sequencing were used to detect HPV DNA. DNA extraction was carried out using the proteinase K technique, in which 20 μL of proteinase K enzyme (10 mg/mL, Invitrogen, USA) was added to 100 μL of the sample. This solution was incubated at 65ºC (overnight), followed by a thermal shock at 95ºC for 10 min. The extracted DNA was first submitted to amplification of a human constitutive gene (gpdH) to verify the quality of the DNA obtained. Samples that were positive for gpdH (glucose phosphate dehydrogenase) amplification were then submitted to the specific amplification for HPV detection using primers MY09 and MY11 and reagents supplied by Invitrogen (USA) as described by Manos et al. (1989). A negative control (no DNA) was included in each PCR run to ensure no cross contamination. The PCR product was submitted to 1% agarose gel electrophoresis, stained with ethidium bromide and visualised on a transilluminator using ultraviolet light. The DNA bands from all positive samples were purified and sequenced to identify the HPV type using the Big-Dye protocol, as recommended by the manufacturer and the Genetic Analysing ABI 3100 sequencer, with 96 capillary tubes (Applied Biosystems, USA). The results were analysed with the aid of the BlastN tool, which is available from the website of the National Centre for Biotechnology Information (2007) (http://www.ncbi.nlm.nih.gov/). For the Hybrid Capture II, the manufacturer's technical protocols were followed. With the uterine cervix exposed, samples were collected with a single-use sterile swab at the entrance to the endocervix, the ectocervix and the vaginal walls. The biological specimens were packed in tubes containing transportation buffer (Specimen Transport Medium, STM) and were sent within 12 days to Digene Brazil (São Paulo, Brazil) for interpretation. The HC II uses RNA probes that are highly specific for detecting 18 types of HPV divided into two groups: group A (low-risk HPV, subtypes 6, 11, 42, 43 and 44) and group B (high and intermediate-risk HPV, subtypes 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59 and 68). The results were presented using relative light unit (RLU) value for the sample/calibrator. The RLU rate for the examination to be considered positive was 1.0, which corresponds to 1 pg/mL of HPV DNA. The next step consisted of collecting material for oncotic cytological examination, using Ayre's spatula to scrape the ectocervix (squamocolumnar junction) and a brush (cytobrush®) to collect an endocervical sample. The smears were placed on previously identified glass slides and fixed with 95% alcohol. After staining using the Papanicolaou method, the smears were evaluated in the Cytopathology Laboratory of CISAM. The reports issued were based on the Bethesda system (Berek 2003). Colposcopy was the final stage of the examination. Firstly, a 0.9% physiological solution was introduced for cervical inspection. Next, 3% acetic acid was applied to the uterine cervix, with the aim of investigating areas that were reactive to it. Schiller's test was performed using Lugol and the examination was concluded. The colposcopic image descriptions were in line with the Rome international classification for the nomenclature of colposcopic characteristics, as authenticated by the International Federation for Cervical Pathology and Colposcopy (Walker et al. 2003). The data were stored and analysed using Epi-Info software, version 6.04 and SPSS software, version 9.0 and the variables were described as percentages. HPV proportions among groups were analysed using Pearson's chi-squared test. A p value < 0.05 was considered statistically significant. This study and research project had previously been evaluated and approved by the Ethical in Research Committee of the University of Pernambuco (protocol CISAM/009/05). RESULTS The three groups analysed in the present study were shown to be similar in various demographic and socioeconomic categories (Table I). Women in the three groups were of lower socioeconomic status, none of them had reached a university level or had a salary greater than three times the minimum wage. There was a higher proportion of adolescents in the HIV-positive pregnant women than in the HIV-positive non-pregnant group and the HIV-negative pregnant group. Most of the women in all three groups were either married or had a permanent partner (Brandão 2008). Though age and the number of sexual partners were associated to belonging to the three groups, they were not associated with HPV infection: age and HPV infection (p = 0.504); number of sexual partners and HPV infection (0.185). The predominant form of contamination among the HIV-infected patients was sexual contact. Patient characteristics relating to time of diagnosis of HIV infection, CD4+ lymphocyte count, HIV viral load and antiretroviral therapy are shown in Table II. There was a difference, though not statistically significant, in relation to the stage of pregnancy (0.0876) between the two groups of pregnant women. Age group (p = 0.493), number of sexual partners (0.986), diagnosis of HIV infection (0.390) and CD4+ lymphocyte count (p = 0.368) were not associated with HPV infection, although they were associated with pregnancy in HIV-positive women. Only the use of antiretroviral therapy was associated with both the group (0.000) and HPV infection (0.037). When both variables were introduced in a bivariate model, only group remained in the model, indicating that the association with group is independent of the use of antiretroviral therapy. Of the 147 patients, one HIV-positive pregnant woman and three HIV-positive non-pregnant women (2.7%) were negative for GPDH (i.e., their samples had inhibitors of the amplification reaction). Using PCR, 21 of the 143 patients examined using the in-house PCR protocol were negative for HPV DNA and 122 patients were positive for HPV DNA (85.3%). The HIV-positive pregnant group had the highest percentage (96% or 48/50 patients). Figure shows the frequency distribution of HPV DNA in the three study groups. For four of the 122 patients who were positive for HPV DNA (3.3%), it was not possible to type the HPV strain; this was possibly due to infection by multiple types of HPV, which makes the interpretation of the ambiguous sequence difficult using the software. In all of the study groups, the high-risk type of HPV was predominant (Table III). HPV was detected using hybrid capture in 67 of the 147 patients studied (45.6%), with the following distribution: HIV-positive pregnant women, 62.7% (32/51), HIV-positive non-pregnant women, 52.9% (27/51) and HIV-negative pregnant women, 17.7% (8/45). Among the 32 HIV-positive pregnant women, 30 (93.8%) had high-risk HPV and the eight HIV-negative pregnant women were all positive for high-risk HPV (Table IV). The hybrid capture II and PCR molecular methods were compared in the 143 patients who underwent both tests. Although there was a significant agreement between the PCR and HC II methods (p = 0.031), it translated to a weak kappa value of 0.119. PCR did not detect HPV DNA in five samples (1 HIV-positive pregnant woman, 3 HIV-positive non-pregnant women and 1 HIV-negative pregnant woman), while the HC II method failed to detect it in 62 samples (Table V). The sensitivity of HC II was 49.2%, its specificity was 76.2%, PPV was 92.3% and NPV was 20.5%. Of the 62 samples shown to be false negatives by HC II, 66.1% (41/62) had types of HPV that were not included in probes A and/or B. Theremaining 33.9% (21/62) consisted of HPV types that were included in theprobes. The cytological analysis found a high frequency of smears with inflammatory abnormalities in the three study groups. Abnormalities in squamous cells were more frequently present among the HIV-positive groups, represented by three times as many cases among the seropositive women (18; 35.3%) and twice as many among the HIV-positive pregnant women (11; 21.6%), than in the HIV-negative pregnant women (6; 13.3%) (p = 0.037) (Table IV). Among the seropositive women who were not pregnant, 12 (66.7%) presented cytomorphological findings that were compatible with HPV infection: koilocytosis, binucleation and keratinisation. Among the HIV-positive pregnant women, all lesions were low grade and HPV was identified in six patients (54.4%) through cytological analysis. There were some patients in all groups with more than one colposcopic abnormality, the most frequent of which was acetic white epithelium. Biopsies were not carried out on the women who were pregnant (Puig-Tintoré et al. 2002), except in one case of an HIV-negative pregnant woman presenting colpocytological findings of high-grade intraepithelial lesion (CIN III - Ca in situ), with colposcopic findings of acetic white epithelium and atypical vessels, who had a histological report of in situ carcinoma, although there was the possibility of invasion. This patient underwent high-frequency surgery and grade II invasive epidermoid carcinoma was diagnosed, with multiple foci of vascular invasion. PCR identified HPV 66 and HC II was positive for group B. DISCUSSION In the present study, the prevalence of HPV was highest among the HIV-positive pregnant women and there was a high prevalence of high-risk HPV, regardless of the study group. The cervical environment probably favoured the establishment of oncogenic types of HPV due to the set of local immunological factors, such as immunoglobulin secretions, local levels of CD4, Langerhans cells and concomitant infections (Mota 2002, Nicol et al. 2005, Santegoets et al. 2008). Pregnancy can hasten and intensify infection by high-risk HPV (in particular, by HPV 16) and presents highly sensitive conditions for HPV activation, persistence and transformation (Armbruster-Moraes et al. 2000). In similar studies using the same molecular test (PCR), a high prevalence of HPV was also found among HIV-positive pregnant women in different settings (Mota 2002, Bollen et al. 2006, Minkoff et al. 2006). In a multicentre study involving seven countries, Muñoz et al. (2002) found that HPV 16 was the most common type in all of them, with percentages ranging from 43.9% (in the Philippines) to 72.4% (in Morocco). HPV 16 and 18 (Muñoz et al. 2002, Rabelo-Santos et al. 2003, Silva 2004, Fernandes et al. 2004, Ho et al. 2005, Lin et al. 2006, Wright et al. 2006) have been shown to be the types most frequently found in cervical infections, such that HPV 16 was associated with more than half of all cervical carcinoma cases (Zerbini et al. 2001) and HPV 18 with 12% (Welkovic 2007). Women who are positive for high-risk HPV DNA have a higher likelihood of developing CIN II or CIN III during follow up than do women who are negative for HPV DNA. This likelihood increases when HPV 16 or 18 is present (Wright et al. 2006). According to Sun et al. (1997), HPV 16 and 18 are the types with the highest frequency among HIV-infected women. In the present sample, HPV 16 and 18 corresponded to the first and third most frequent types. In addition, nine patients were identified with two types of HPV, of which at least one type was high risk. This could be associated with the persistence of infection (Trotier & Franco 2006). Mota (2002) identified a high rate of persistence of high-oncogenic-risk HPV infection (69.4%) among HIV-positive women who were pregnant and the most frequent types were HPV 16 and 58. HPV 58, 66, 31 and 70 were other frequently found types in the present study. Chan et al. (1999) suggested that HPV 58 also had a significant role in the aetiology of cervical carcinoma. The viral types 16, 31, 33, 38, 52, 58 and 67 are all grouped in the same branch of the phylogenetic tree, thus indicating their similarity regarding oncogenic potential (IARC 2007). In the present study, the high prevalence of HPV 58 is in agreement with other studies that revealed the importance of this type in some regions of Brazil (North, Northeast and Centre-West) and in the Orient (Mota 2002, Câmara et al. 2003, Yokoyama et al. 2003, Clifford et al. 2005, Nicol et al. 2005, Lin et al. 2006, Wright et al. 2006, Pereira et al. 2007). The results obtained here corroborate the idea that there are regional variations of certain HPV types in Brazil (Câmara et al. 2003, Queiroz et al. 2004, Pereira et al. 2007). Attention is drawn to the high frequency of HPV 66, which was included among the high-risk types of HPV in the new IARC classification (2007). In our study, its presence was identified in 13 cases: in 10 cases alone and in association with another high-risk type in three cases. The agreement between the molecular methods used in the present study was significant, albeit weak (Kappa = 0.119; p = 0.031). The PCR method was shown to be extremely sensitive, coinciding with data in the literature (Villa & Denny 2006), whereas HC II presented a lower sensitivity, in fact, less than what other authors have reported (Dillner 2001, Castle et al. 2002, Koliopoulos et al. 2007, De Francesco et al. 2008). In a meta-analysis on tests for identifying HPV, Arbyn et al. (2006) found that the HC II method presented high sensitivity. Some of the findings responsible for the low sensitivity of HC II seen in the present study may be due to the fact that 41 of the 62 HIV-positive patients had HPV types determined using PCR that did not appear in the HC II probes. Among the 21 cases that were positive by PCR and negative by HC II and whose HPV-DNA types were contained in probes A and/or B, the number of copies was lower than the cut-off suggested by the manufacturer. For probe A, the mean was 0.27, with a standard deviation of 0.14 (minimum 0.10 and maximum 0.89), while for probe B, the mean was 0.35 with a standard deviation of 0.19 (minimum 0.14 and maximum 0.96). PCR is the most sensitive technique for identifying HPV DNA (Villa & Denny 2006, IARC 2007). Despite its unquestionable value, this technique may present false negative results. In the present study, PCR did not diagnose five patients (3.5%) who had a positive HC II. False negative results are frequently related to the presence of inhibitors of PCR in the samples or impairment of primer-template annealing due to local DNA modifications or inappropriate annealing temperature during the cycling. The significant percentage of inflammatory processes, along with the bleeding inherent to the gestational period could have been a source of amplification inhibitors. However, it would be unlikely, since we were able to amplify the gpdH gene from these five patients. The annealing temperature of the HPV-specific PCR is low to allow primer-template annealing using degenerate primers. Nevertheless, further modification of the DNA sequence could prevent primer-template annealing and amplification. The possibility of having not added the template in the reaction was not considered as the reaction was repeated more than twice. The prevalence of IEL observed from oncotic cytological analysis in the HIV-positive groups was similar to what has been found in other studies (Levi et al. 2002, Mota 2002, Silva 2004, Silva et al. 2005, Parham et al. 2006). Parham et al. (2006) identified the presence of IEL in 114 (76%) of 150 HIV-positive women who were examined using cytological analysis. Among these, 49 cases were high risk (32.6%). They concluded that the presence of a high-risk HPV type was associated with the presence of severe cytological abnormality. Despite recognising that the cervicovaginal inflammatory processes that are frequent among HIV-positive women create difficulties in the oncological interpretation of colpocytological findings, Wright et al. (1994) determined a sensitivity of 81% and a specificity of 87%. To improve the accuracy of investigations, it has been recommended that colposcopic examinations should be performed in conjunction with colpocytological analysis for IEL screening (Nappi et al. 2005). A significant proportion of women with normal cytological findings have been diagnosed positive for high-risk HPV DNA by means of molecular tests. It can be inferred that such cases were either recent infections, which had not had time for cytological lesion development or slow infections that were only identified by molecular means (Fernandes et al. 2004). Another possible explanation would be the use of antiretrovirals. Low viral loads associated with TCD4 counts greater than 200 cells/mm³ indicate immunity that has not been greatly altered in the study groups. Women who used antiretroviral therapy have been found to present higher rates of IEL regression (Minkoff et al. 2001, Ahdieh-Grant et al. 2004). This seems plausible, since antiretroviral therapy reverses immunodeficiency, thereby increasing the number of TCD4 cells (Heard et al. 1998) and reducing the viral load (Wagner et al. 2001). The availability of a vaccine against HPV with a selective protection spectrum for some viral types makes it important to know the regional distribution of the different types of HPV (Mammas et al. 2008). In addition to HPV 16 and 18, which have the highest incidence worldwide, types 58 and 66 were identified, sometimes in multiple infections. These results reveal that the use of existing vaccines may not sufficiently reflect the realities of HPV in all regions (i.e., regional variations in virus type have greater importance than what was supposed) and that the planning for future immunisation programmes must respect such regional characteristics. REFERENCES
Copyright 2009 - Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc09167t5.jpg] [oc09167t1.jpg] [oc09167t4.jpg] [oc09167t2.jpg] [oc09167t3.jpg] [oc09167f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}