 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
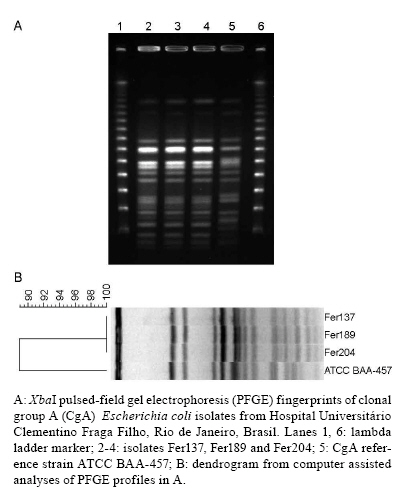
Memórias do Instituto Oswaldo Cruz, Vol. 104, No. 5, August, 2009, pp. 787-789 SHORT COMMUNICATIONS Identification of uropathogenic Escherichia coli clonal group A (CgA) in hospitalised patients Rubens CS DiasI; Denise V MarangoniII; Lee W RileyI; Beatriz M MoreiraIII, + ISchool
of Public Health, University of California, Berkeley, CA, USA Financial support: CNPq, CAPES, FAPERJ, Fogarty International Program in Global Infectious Diseases (TW006563) of National Institutes of Health (AI059523) Received 2 January
2009 Code Number: oc09172 ABSTRACT This study provides the first description of healthcare-associated infections with Escherichia coli clonal group A (CgA) isolates in Latin America. Isolates were typed by enterobacterial repetitive intergenic consensus-PCR, pulsed-field gel electrophoresis, E. coli phylogenetic grouping, multilocus sequence typing and fimH single nucleotide polymorphism analysis. Out of 42 E. coli hospital isolates studied, three belonged to E. coli phylogenetic group D and ST69 and had fimH sequences identical to that of the CgA reference strain ATCC BAA-457. E. coli CgA is another potential source of resistant infections in hospitals. Key words: community E. coli clonal group - hospital infections - antimicrobial resistance In 2001, Manges et al. (2001) identified an Escherichia coli clonal group A (CgA) designated based on enterobacterial repetitive intergenic consensus (ERIC)-PCR electrophoretic banding pattern. CgA isolates accounted for up to 50% of trimethoprim-sulfamethoxazole (SXT)-resistant E. coli isolated from women with acute uncomplicated urinary tract infections (UTI) in one university community (Manges et al. 2001). CgA isolates have been recovered from women in the United States with cystitis, pyelonephritis and bloodstream infections (Manges et al. 2001, 2004, Johnson et al. 2002, Petrof et al. 2002). CgA isolation has also been described in other parts of the world (Johnson et al. 2005, Manges et al. 2008). The isolates in Latin America studied to date were found among a collection of 60 E. coli isolates of unknown origin in Curitiba, state of Paraná, Brazil. CgA was found in three urine isolates by random amplification of polymorphic DNA and phylogenetic grouping analyses (Johnson et al. 2005). In the present report, we describe the identification of three CgA E. coli isolates from a public university-affiliated hospital in Rio de Janeiro, Brazil, exhibiting the four predominant ERIC-PCR bands of approximately 1145, 1029, 908 and 720 bp that are typically observed for CgA (Manges et al. 2001). These isolates were further characterised as described below. Initially, E. coli isolates were evaluated by ERIC-PCR and pulsed-field gel electrophoresis (PFGE), as previously described (Bender et al. 1997, Dias et al. 2008). Briefly, for ERIC-PCR, amplifications were carried out in a total volume of 25 μL. Each reaction contained buffer, 0.1 mM of each dNTP, 3 mM MgCl2, 0.3 μM ERIC2 primer (5'-AAGTAAGTGACTGGGGTGAGCG-3'), 1.5 U Taq DNA polymerase (BIOTOOLS) and 3 μL template DNA. Reaction conditions were as follows: a 2 min initial denaturation at 94ºC followed by 40 cycles of a 30 sec denaturation at 94ºC, a 1 min annealing at 54ºC and a 4 min extension at 72ºC and a final extension step of 1 min at 72ºC. Amplification products were electrophoresed on 1.5% agarose gels. For PFGE, chromosomal DNA in the plugs was digested with XbaI (New England BioLabs) at 37ºC according to the instructions of the manufacturer. The restriction fragments were separated by PFGE on 1% agarose gels and electrophoresis was carried out in a CHEF DR II system (Bio-Rad Laboratories) at 13ºC and 6 V/cm for 22 h with pulse times ranging from 2.2-54.2 sec. DNA-banding patterns were interpreted by visual inspection and with the GelCompar II program version 4.01 (Applied Maths, Sint-Martens-Latem, Belgium). The CgA reference strain ATCC BAA-457 was included for comparison in all experiments. For phylogenetic analysis, E. coli phylogrouping (A, B1, B2 or D) was assessed using a previously reported triplex PCR-based assay (Clermont et al. 2000). In addition, multilocus sequence typing (MLST) was performed using a standardised protocol for E. coli maintained at the MLST Databases at the ERI, University College Cork website (http://mlst.ucc.ie/). Briefly, amplifications were carried out in a total volume of 50 μL. Each reaction contained buffer, 0.2 mM of each dNTP, 1.5 mM MgCl2, 0.2 μM of each primer, 2.5 U AmpliTaq Gold (Applied Biosystems) and 2 μL template DNA. Reaction conditions were as follows: a 2 min initial denaturation at 95ºC followed by 30 cycles of a 1 min denaturation at 95ºC, a 1 min annealing at the temperature specified for each gene (http://mlst.ucc.ie/) and a 2 min extension at 72ºC and a final extension step of 5 min at 72ºC. fimH single nucleotide polymorphism analysis was performed as reported previously (Tartof et al. 2007) with modifications. Primers used for PCR amplification and partial fimH gene sequencing were FimH-f (5'-CGAGTTATTACCCTGTTTGCTG-3') and FimH-r (5'-ACGCCAATAATCGATTGCAC-3'). Both strands of the 878 bp PCR-amplified fragment were sequenced. After visual inspection and editing with BioEdit version 7.0.9.0, fragments of 424 bp fimH sequences (located at bp 401-824 of E. coli sequence accession #NC000913, GenBank) were compared to the CgA reference sequence. The three putative CgA strains were recovered from three female patients older than 45 years of age with healthcare-associated infections. Two isolates (Fer137 and Fer204) were obtained from the urine of patients with symptomatic (fever without any other identifiable causes and/or abdominal pain) UTI. One isolate was from a transplant patient with a bladder catheter-associated UTI and the other from a patient admitted to investigate a respiratory disease, but without a urinary catheter. The third isolate (Fer189) was obtained from a blood culture of a patient with collagen disease. This patient had a central vascular catheter in place and the bloodstream infection was considered to be a central vascular catheter-associated infection. All patients were admitted to the hospital between May 11-29 2001 and the E. coli isolates were recovered 6-20 days after admission. The three isolates were detected as SXT and cephalothin-resistant by disk diffusion testing (CLSI 2009) and they exhibited indistinguishable ERIC2-PCR and PFGE band patterns. The ERIC2-PCR band patterns of the isolates were also indistinguishable from that of the CgA reference strain ATCC BAA-457 (100% similarity), whereas the PFGE patterns of the isolates showed four band differences compared to the reference strain (89% similarity) (Figure). All isolates belonged to E. coli phylogroup D and ST69 by MLST and had identical fimH sequence to CgA reference strain. The reference strain ATCC BAA-457 also belongs to phylogroup D and ST69 (Tartof et al. 2005). This is the first time E. coli CgA has been detected in patients in Rio de Janeiro, Brazil, and the first confirmed case of healthcare-associated CgA infections in Latin America. The possible sources of CgA in Brazil are unknown. It has been suggested that CgA can be spread by contaminated food (Manges et al. 2007) and its presence in sewage effluents may provide an additional source (Boczek et al. 2007). We believe a common source or cross-transmission of the CgA probably occurred among the three patients in the hospital because they were clustered in place and time and the isolates had identical PFGE patterns. PFGE bands may change in short periods of time (Tenover et al. 1995); therefore, the finding of identical patterns strongly suggests a close common ancestor. However, since CgA is a community pathogen, we cannot exclude the possibility that patients already had CgA isolates in their own microflora before admission, acquired from a community source. CgA E. coli isolates have been shown to harbour integron-borne resistance gene cassettes, including the recently identified dihydrofolate-reductase dfr17 gene (France et al. 2005, Solberg et al. 2006). CgA in Rio de Janeiro, especially in a healthcare setting, may facilitate dissemination of these resistance genes and serve as yet another source of resistant infections in our hospitals as well as in our community. REFERENCES
Copyright 2009 - Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc09172f1.jpg] |
| |||||||||

{kind=link}