 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memórias do Instituto Oswaldo Cruz, Vol. 104, No. 5, August, 2009, pp. 797-800 SHORT COMMUNICATIONS Performance levels of four Latin American laboratories for the serodiagnosis of Chagas disease in Mexican sera samples Alejandro O LuquettiI; Bertha EspinozaII; Ignacio MartínezII; Nidia Hernández-BecerrilIII; Carlos PonceIV; Elisa PonceIV; Pedro A ReyesIII; Oscar HernándezV; Ruth LópezV; Victor MonteónIII, V, + IInstituto
de Patología Tropical e Saúde Pública, Universidade Federal
de Goiás, Goiania, Brasil Financial support: DGAPA (IN226402), UNAM (BE), PROMEP/ 103.5/04/833 (VM) Received 19 January
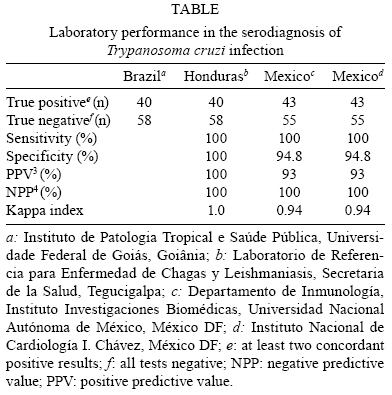
2009 Code Number: oc09174 ABSTRACT In nearly all of the previous multicentre studies evaluating serological tests for Trypanosoma cruzi infection, sera samples from Central or South American countries have been used preferentially. In this work we compared the reliability of the serological tests using Mexican sera samples that were evaluated in four independent laboratories. This included a reference laboratory in Brazil and three participant laboratories, including one in Central America and two in Mexico. The kappa index between Brazilian and Honduran laboratories reached 1.0 and the index for the Mexican laboratories reached 0.94. Another finding of this study was that the source of antigen did not affect the performance of the serological tests. Key words: Trypanosoma cruzi - Chagas disease - serological tests - blood donors - Mexican strains American trypanosomiasis, also commonly known as Chagas disease, is caused by the protozoan flagellate Trypanosoma cruzi. Diagnosis of the chronic phase is typically based on the detection of IgG antibodies in the sera of patients. The serological tests currently in use are indirect immunofluorescence (IIF), indirect hemagglutination (IHA) and enzyme-linked immunosorbent assay (ELISA). They regularly use crude antigenic T. cruzi preparations or semipurified fractions and more recently these tests have used recombinant antigens (Oeleman et al. 1998, Luquetti et al. 2003, Umezawa et al. 2004, Cooley et al. 2008). Although many screening methods and sources of antigens have been evaluated, sensitivity and specificity levels have seldom reached 100%. It has been suggested that variability among T. cruzi isolates in conjunction with immunogenetic features of the human host and environmental factors could affect the performance of serological tests (Umezawa et al. 1999, Luquetti et al. 2003). T. cruzi consists of a pool of sub-populations that presents high heterogeneity in both biological parameters and genetic characteristics (Souto et al. 1996, Espinoza et al. 1998, Briones et al. 1999). As a whole, serum samples from infected patients react better to whole parasite extracts than recombinant antigens, which is likely due to the presence of a large number of antigenic determinants. Nevertheless, some variation of ELISA absorbance values in serum samples from different countries has been observed (Umezawa et al. 1999). Furthermore, higher titers of anti T. cruzi antibodies have been detected in individuals residing in high endemic regions for T. cruzi infection when compared against infected individuals living in low endemic areas (Borges-Pereira & Coura 1986, Sosa-Jurado et al. 2003). The same observations hold true for those symptomatic with chronic chagasic cardiopathy when compared against those who are asymptomatic for chronic chagasic cardiopathy (Nava et al. 2001). In nearly all of the previously conducted multicentric studies that evaluated serological tests of T.cruzi infection, only sera samples from Central or South American countries have been evaluated. The aim of this work was to compare the reliability of serological tests using Mexican blood samples and Mexican T. cruzi isolates. We then wanted to compare these results to those from several South and Central American laboratories. México is the most northern country in the American continents in which T. cruzi infections are endemic, with an estimated infected population of approximately 1,768,376. Within the infected population, acute, cardiac and symptomless human cases have been described (Mendoza et al. 1995, Monteon-Padilla et al. 1999, Mazariego-Arana et al. 2001, Ramsay et al. 2003). The predominate T. cruzi group identified in Mexican chagasic patients has been lineage I (Bosseno et al. 2002, Ruíz-Sánchez et al. 2005). The samples used in this current study were collected at the Instituto Nacional de Cardiología I. Chavéz, which is located in México City. A panel of 98 serum samples consisting of seropositive and seronegative blood donor sera was used. This included a group of 15 sera samples from chronic chagasic cardiopathy patients (CCC) who underwent a clinical evaluation (ECG, chest X-ray, ECO tests) and also had two serologic positive tests carried out at the Instituto Nacional Cardiología I. Chavéz. In addition, five of the sera samples were from non-chagasic cardiopathy patients and used as negative controls. Samples were stored in 50% glycerol for serum reactivity preservation and were sent to the participating laboratories in Brazil [Instituto de Patologia Tropical e Saúde Pública, Universidade Federal de Goiás (UFG), Goiania], Honduras [Laboratorio de Referencia para Enfermedad de Chagas y Leishmaniasis, Secretaria de la Salud (SS), Tegucigalpa] and México [Departamento de Inmunología, Instituto Investigaciones Biomédicas (IIB), Universidad Nacional Autónoma de México, México DF]. A fourth set of samples remained at the Instituto Nacional de Cardiología I. Chávez, in México City. All blood donors were clinically evaluated by the blood banking service before their acceptance as candidates. Each participating laboratory applied their individual routine serologic techniques to establish T. cruzi infection. The Brazilian laboratory (UFG) was considered to be the reference centre for our study. In this institution, the IIF was performed using formaldehyde-treated epimastigote forms of T. cruzi (Y strain). Results were considered to be positive when a dilution of 1/40 or above showed positivity (Umezawa et al. 1999). An "in house" ELISA was performed using a crude extract of Y strain epimastigotes and the results were expressed as an index. The index was obtained by dividing the optical density (OD) of the sample by the OD of the plate cut-off. An index value that was equal to or greater than 1.2 was considered to be positive. For IHA, the results were expressed as the reciprocal of titer dilution. Titers equal to or above 32 were considered to be positive. The detection of anti-T. cruzi antibodies by three different serologic tests was the criterion used to characterise an infected individual. In addition, anti-leishmania IIF serology was used as a complementary test. In the Honduras laboratory (SS), two commercial ELISA versions were used. This included ELISA using the crude native extract (Wiener Lab) and ELISA using recombinant antigens (Wiener Lab). In both cases, the manufacturer's instructions were followed. A third rapid immunochromatographic screening test (Chembio Diagnostic Systems, Medford, NY, USA) was also used for the detection of anti-T.cruzi antibodies. IIF was performed using formaldehyde-treated epimastigote forms of T. cruzi (Y strain) and fluorescein-isothiocyanate sheep anti-human IgG (Fluoline G, Biolab Diagnóstica SA, RJ, Brazil). The results were considered positive when a dilution equal to or above 1/40 was observed. In the Mexican (IIB) laboratory, two serologic "in house" tests were performed, which were ELISA and western blot. ELISA was performed using a crude extract from the Queretaro Mexican T. cruzi isolate. Each test was carried out in duplicate. Negative and positive sera controls were run for each plate. The ELISA cut-off point was obtained by calculating the OD average of negative controls + 2.5 standard deviations. For the western blot, proteins of the total extract (Queretaro isolate) were separated by SDS-PAGE and transferred to nitrocellulose membranes (100 μg of protein each). After an overnight saturation in PBS containing 10% skimmed milk at 4ºC with constant shaking, the nitrocellulose membrane was cut into strips and these strips were individually incubated for 2 h at RT in 1 mL of human serum diluted 1:500 in PBS/10% skimmed milk with constant shaking. Positive and negative control sera were included in each experiment (Sanchez et al. 2001). A positive result was noted when two or more bands were present. In the Mexican (INC) laboratory, two serologic homemade tests were performed. An IIF assay was carried out as reported (Ramos-Echavarria et al. 1993). To briefly explain, a drop of epimastigote (Ninoa Mexican Strain) suspension was air dried on a slide. Human experimental and control sera were then diluted at 1:32 (cut-off dilution) in PBS and incubated in a humidified chamber for 30 min. If fluorescence of the parasites was observed, the sample was scored as positive. ELISA was then conducted using polystyrene plates (Immunolon II Thermo Labsystems, Franklin, Mass.) coated with 10 μg/ml of T. cruzi protein (Ninoa Mexican strain) extract in an alkaline-buffered solution. Human serum was diluted at 1:200 and anti-human IgG-peroxidase conjugate was used at a 1:15,000 dilution (Zymed Lab, Santa Cruz Ca, USA). The reaction was revealed by the addition of O-phenilen-diamine and read at 490 nm in an automatic ELISA reader (Biorad, Palo Alto Ca, USA). The cut off value was set by testing the sera from 30 healthy seronegative people, which was then pooled and individually tested. Mean OD ratios obtained between an individual negative sample and the pooled negative sample were analyzed for their distribution. The mean OD ratio of seronegative healthy individuals plus 3 SD was fixed to set the cut off. All healthy individuals had values classified as negative. The determination of anti-leishmania antibodies by IIF was also included in the study as a complementary test. Using the laboratory values obtained in Brazil as a reference, we estimated the sensitivity, specificity and º index. Positive samples were those with at least two serological positive results, whereas negative samples were either samples with all negative results or two negative results and one positive result. Despite the fact that Mexican laboratories used T. cruzi Mexican isolates that belonged to lineage I (Ninoa and Queretaro), their diagnostic performance and reliability showed acceptable results. The Kappa index indicated a high proportion of true agreement among the four participating laboratories. For the SS, the index was 1.0, which is an excellent result. Sensitivity, which is the ability of the method to identify true positives, reached levels of 100%. The sensitivity parameter is very important for avoiding false negatives. The specificity levels also reached 100% as well. Although the SS ranked the highest in all parameters, the results reached in Mexican laboratories were very close and comparable. The sensitivity in both laboratories reached 100% and specificities were found to be between 91-98% with Kappa indices between 0.93-0.98 (Table). Even though the participating laboratories applied their own techniques and antigens, high concordance, specificities and sensitivities were observed when examining the Mexican samples of both infected and uninfected individuals. A remarkable finding was the excellent agreement with the CCC samples, given that the four laboratories recognised all of them as positive. However, when we compared the results of blood donor samples the concordance was lower for the Mexican laboratories. On the other hand, in Brazil (UFG), 14 leishmaniasis reactive samples in the blood donor group were detected by IIF, eight of which reacted to both leishmania and T. cruzi antigens. We believe that the cross-reactivity is due to membrane antigens, because the sera were negative in both the ELISA and IHA tests. The remaining six positive anti-leishmania samples reacted solely to leishmania antigens. On the other hand, in Mexico (INC), only six samples out of the 14 initially identified as positive in Brazil (UFG) tested positive. Among these, five reacted solely to leishmania antigens. This finding may suggest that the IIF assay may be more cross-reactive with antigens between the two species when compared against the ELISA or IHA assays. Another interesting finding was that the recombinant antigens used in Honduras (SS) showed identical performances to the crude extract that was used (Wiener Lab ELISA). In addition, similar results were obtained with the rapid immunochromatographic test (Chembio Diagnostic Systems, Medford, NY, USA), suggesting its use as a reliable testing method. To sum up, the data indicate that humoral immune responses of Mexican chagasic infected individuals are able to recognise antigens from either Mexican or Brazilian parasite strains, independent of which T. cruzi lineage they belong to. In conclusion, our data strongly support that serological tests in Mexican laboratories are acceptable and that both the geographical origin of the serum samples and the use of T. cruzi I as a source of antigens do not affect the performance of serological assays. ACKNOWLEDGEMENTS To Silvia Monteón, for English correction of the manuscript. REFERENCES
Copyright 2009 - Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc09174t1.jpg] |
| |||||||||

{kind=link}